Kidney News | October/November 2011
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

RANDY SCHEKMAN Department of Molecular and Cell Biology, Howard Hughes Medical Institute, University of California, Berkeley, USA
GENES AND PROTEINS THAT CONTROL THE SECRETORY PATHWAY Nobel Lecture, 7 December 2013 by RANDY SCHEKMAN Department of Molecular and Cell Biology, Howard Hughes Medical Institute, University of California, Berkeley, USA. Introduction George Palade shared the 1974 Nobel Prize with Albert Claude and Christian de Duve for their pioneering work in the characterization of organelles interrelated by the process of secretion in mammalian cells and tissues. These three scholars established the modern field of cell biology and the tools of cell fractionation and thin section transmission electron microscopy. It was Palade’s genius in particular that revealed the organization of the secretory pathway. He discovered the ribosome and showed that it was poised on the surface of the endoplasmic reticulum (ER) where it engaged in the vectorial translocation of newly synthesized secretory polypeptides (1). And in a most elegant and technically challenging investigation, his group employed radioactive amino acids in a pulse-chase regimen to show by autoradiograpic exposure of thin sections on a photographic emulsion that secretory proteins progress in sequence from the ER through the Golgi apparatus into secretory granules, which then discharge their cargo by membrane fusion at the cell surface (1). He documented the role of vesicles as carriers of cargo between compartments and he formulated the hypothesis that membranes template their own production rather than form by a process of de novo biogenesis (1). As a university student I was ignorant of the important developments in cell biology; however, I learned of Palade’s work during my first year of graduate school in the Stanford biochemistry department. -

A Short History of DNA Technology 1865 - Gregor Mendel the Father of Genetics
A Short History of DNA Technology 1865 - Gregor Mendel The Father of Genetics The Augustinian monastery in old Brno, Moravia 1865 - Gregor Mendel • Law of Segregation • Law of Independent Assortment • Law of Dominance 1865 1915 - T.H. Morgan Genetics of Drosophila • Short generation time • Easy to maintain • Only 4 pairs of chromosomes 1865 1915 - T.H. Morgan •Genes located on chromosomes •Sex-linked inheritance wild type mutant •Gene linkage 0 •Recombination long aristae short aristae •Genetic mapping gray black body 48.5 body (cross-over maps) 57.5 red eyes cinnabar eyes 67.0 normal wings vestigial wings 104.5 red eyes brown eyes 1865 1928 - Frederick Griffith “Rough” colonies “Smooth” colonies Transformation of Streptococcus pneumoniae Living Living Heat killed Heat killed S cells mixed S cells R cells S cells with living R cells capsule Living S cells in blood Bacterial sample from dead mouse Strain Injection Results 1865 Beadle & Tatum - 1941 One Gene - One Enzyme Hypothesis Neurospora crassa Ascus Ascospores placed X-rays Fruiting on complete body medium All grow Minimal + amino acids No growth Minimal Minimal + vitamins in mutants Fragments placed on minimal medium Minimal plus: Mutant deficient in enzyme that synthesizes arginine Cys Glu Arg Lys His 1865 Beadle & Tatum - 1941 Gene A Gene B Gene C Minimal Medium + Citruline + Arginine + Ornithine Wild type PrecursorEnz A OrnithineEnz B CitrulineEnz C Arginine Metabolic block Class I Precursor OrnithineEnz B CitrulineEnz C Arginine Mutants Class II Mutants PrecursorEnz A Ornithine -
Humankind 2.0: the Technologies of the Future 6. Biotech
Humankind 2.0: The Technologies of the Future 6. Biotech Piero Scaruffi, 2017 See http://www.scaruffi.com/singular/human20.html for the full text of this discussion A brief History of Biotech 1953: Discovery of the structure of the DNA 2 A brief History of Biotech 1969: Jon Beckwith isolates a gene 1973: Stanley Cohen and Herbert Boyer create the first recombinant DNA organism 1974: Waclaw Szybalski coins the term "synthetic biology” 1975: Paul Berg organizes the Asilomar conference on recombinant DNA 3 A brief History of Biotech 1976: Genentech is founded 1977: Fred Sanger invents a method for rapid DNA sequencing and publishes the first full DNA genome of a living being Janet Rossant creates a chimera combining two mice species 1980: Genentech’s IPO, first biotech IPO 4 A brief History of Biotech 1982: The first biotech drug, Humulin, is approved for sale (Eli Lilly + Genentech) 1983: Kary Mullis invents the polymerase chain reaction (PCR) for copying genes 1986: Leroy Hood invents a way to automate gene sequencing 1986: Mario Capecchi performs gene editing on a mouse 1990: William French Anderson’s gene therapy 1990: First baby born via PGD (Alan Handyside’s lab) 5 A brief History of Biotech 1994: FlavrSavr Tomato 1994: Maria Jasin’s homing endonucleases for genome editing 1996: Srinivasan Chandrasegaran’s ZFN method for genome editing 1996: Ian Wilmut clones the first mammal, the sheep Dolly 1997: Dennis Lo detects fetal DNA in the mother’s blood 2000: George Davey Smith introduces Mendelian randomization 6 A brief History of Biotech -

Guide to Biotechnology 2008
guide to biotechnology 2008 research & development health bioethics innovate industrial & environmental food & agriculture biodefense Biotechnology Industry Organization 1201 Maryland Avenue, SW imagine Suite 900 Washington, DC 20024 intellectual property 202.962.9200 (phone) 202.488.6301 (fax) bio.org inform bio.org The Guide to Biotechnology is compiled by the Biotechnology Industry Organization (BIO) Editors Roxanna Guilford-Blake Debbie Strickland Contributors BIO Staff table of Contents Biotechnology: A Collection of Technologies 1 Regenerative Medicine ................................................. 36 What Is Biotechnology? .................................................. 1 Vaccines ....................................................................... 37 Cells and Biological Molecules ........................................ 1 Plant-Made Pharmaceuticals ........................................ 37 Therapeutic Development Overview .............................. 38 Biotechnology Industry Facts 2 Market Capitalization, 1994–2006 .................................. 3 Agricultural Production Applications 41 U.S. Biotech Industry Statistics: 1995–2006 ................... 3 Crop Biotechnology ...................................................... 41 U.S. Public Companies by Region, 2006 ........................ 4 Forest Biotechnology .................................................... 44 Total Financing, 1998–2007 (in billions of U.S. dollars) .... 4 Animal Biotechnology ................................................... 45 Biotech -

Documenting the Biotechnology Industry in the San Francisco Bay Area
Documenting the Biotechnology Industry In the San Francisco Bay Area Robin L. Chandler Head, Archives and Special Collections UCSF Library and Center for Knowledge Management 1997 1 Table of Contents Project Goals……………………………………………………………………….p. 3 Participants Interviewed………………………………………………………….p. 4 I. Documenting Biotechnology in the San Francisco Bay Area……………..p. 5 The Emergence of An Industry Developments at the University of California since the mid-1970s Developments in Biotech Companies since mid-1970s Collaborations between Universities and Biotech Companies University Training Programs Preparing Students for Careers in the Biotechnology Industry II. Appraisal Guidelines for Records Generated by Scientists in the University and the Biotechnology Industry………………………. p. 33 Why Preserve the Records of Biotechnology? Research Records to Preserve Records Management at the University of California Records Keeping at Biotech Companies III. Collecting and Preserving Records in Biotechnology…………………….p. 48 Potential Users of Biotechnology Archives Approaches to Documenting the Field of Biotechnology Project Recommendations 2 Project Goals The University of California, San Francisco (UCSF) Library & Center for Knowledge Management and the Bancroft Library at the University of California, Berkeley (UCB) are collaborating in a year-long project beginning in December 1996 to document the impact of biotechnology in the Bay Area. The collaborative effort is focused upon the development of an archival collecting model for the field of biotechnology to acquire original papers, manuscripts and records from selected individuals, organizations and corporations as well as coordinating with the effort to capture oral history interviews with many biotechnology pioneers. This project combines the strengths of the existing UCSF Biotechnology Archives and the UCB Program in the History of the Biological Sciences and Biotechnology and will contribute to an overall picture of the growth and impact of biotechnology in the Bay Area. -
How Old Is Biotechnology? the Word Biotechnology Can Be Traced to 1917, When It Was Used to Refer to a Large-Scale Production of Materials from Microbes Grown in Vats
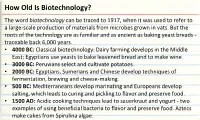
How Old Is Biotechnology? The word biotechnology can be traced to 1917, when it was used to refer to a large-scale production of materials from microbes grown in vats. But the roots of the technology are as familiar and as ancient as baking yeast breads - traceable back 6,000 years. • 4000 BC: Classical biotechnology: Dairy farming develops in the Middle East; Egyptians use yeasts to bake leavened bread and to make wine. • 3000 BC: Peruvians select and cultivate potatoes. • 2000 BC: Egyptians, Sumerians and Chinese develop techniques of fermentation, brewing and cheese-making. • 500 BC: Mediterraneans develop marinating and Europeans develop salting, which leads to curing and pickling to flavor and preserve food. • 1500 AD: Acidic cooking techniques lead to sauerkraut and yogurt - two examples of using beneficial bacteria to flavor and preserve food. Aztecs make cakes from Spirulina algae. How Old Is Biotechnology? (continued) • 1859: On the Origin of Species - English naturalist Charles Darwin's theory of evolution - is published in London. • 1861: French chemist Louis Pasteur develops pasteurization - preserving food by heating it to destroy harmful microbes. • 1865: Austrian botanist and monk Gregor Mendel describes his experiments in heredity, founding the field of genetics. • 1879: William James Beal develops the first experimental hybrid corn • 1910: American biologist Thomas Hunt Morgan discovers that genes are located on chromosomes. • 1928: F. Griffith discovers genetic transformation - genes can transfer from one strain of bacteria to another. • 1941: Danish microbiologist A. Jost coins the term genetic engineering in a lecture on sexual reproduction in yeast. How Old Is Biotechnology? (continued) • 1943: Oswald Avery, Colin MacLead and Maclyn McCarty use bacteria to show that DNA carries the cell's genetic information. -

SHALOM NWODO CHINEDU from Evolution to Revolution
Covenant University Km. 10 Idiroko Road, Canaan Land, P.M.B 1023, Ota, Ogun State, Nigeria Website: www.covenantuniversity.edu.ng TH INAUGURAL 18 LECTURE From Evolution to Revolution: Biochemical Disruptions and Emerging Pathways for Securing Africa's Future SHALOM NWODO CHINEDU INAUGURAL LECTURE SERIES Vol. 9, No. 1, March, 2019 Covenant University 18th Inaugural Lecture From Evolution to Revolution: Biochemical Disruptions and Emerging Pathways for Securing Africa's Future Shalom Nwodo Chinedu, Ph.D Professor of Biochemistry (Enzymology & Molecular Genetics) Department of Biochemistry Covenant University, Ota Media & Corporate Affairs Covenant University, Km. 10 Idiroko Road, Canaan Land, P.M.B 1023, Ota, Ogun State, Nigeria Tel: +234-8115762473, 08171613173, 07066553463. www.covenantuniversity.edu.ng Covenant University Press, Km. 10 Idiroko Road, Canaan Land, P.M.B 1023, Ota, Ogun State, Nigeria ISSN: 2006-0327 Public Lecture Series. Vol. 9, No.1, March, 2019 Shalom Nwodo Chinedu, Ph.D Professor of Biochemistry (Enzymology & Molecular Genetics) Department of Biochemistry Covenant University, Ota From Evolution To Revolution: Biochemical Disruptions and Emerging Pathways for Securing Africa's Future THE FOUNDATION 1. PROTOCOL The Chancellor and Chairman, Board of Regents of Covenant University, Dr David O. Oyedepo; the Vice-President (Education), Living Faith Church World-Wide (LFCWW), Pastor (Mrs) Faith A. Oyedepo; esteemed members of the Board of Regents; the Vice- Chancellor, Professor AAA. Atayero; the Deputy Vice-Chancellor; the -

Dnai DVD and the Dnai Teacher Guide Dnai
DNAi DVD 1 DNAi DVD and the DNAi Teacher Guide The DNA Interactive (DNAi) DVD carries approximately four hours of video interviews with 11 Nobel Laureates and more than 50 other scientists, clinicians, and patients. It also holds the complete set of 3-dimensional animations produced for the DNA TV series and DNAi project. The following pages list video clips and animations from the DVD that would be appropriate to show with specific activities in the DNAi Teacher Guide. The clips and animations are listed under “themes” and “additional animations.” The “themes” listing includes relevant interviews and animations that can be accessed from the “themes” section of the DVD. The “additional animations” are best accessed from “animations” button in the DVD main menu. You can access the DNAi Teacher Guide by registering at www.dnai.org/teacher. Activity 1: DNAi Timeline: a scavenger hunt THEMES • DNA MOLECULE • Discovery of DNA A pre-1953 notion _ biology prior to discovery of the double helix . François Jacob DNA is the genetic material _ the experiment that identified DNA as the genetic material . Maclyn McCarty Chargaff's ratios _ the DNA base ratio rules . Erwin Chargaff The answer _ the X-ray diffraction picture that revealed the helix . Maurice Wilkins DNA: the key to understanding _ why the discovery of DNA's structure was so important . Francis Crick Structure of DNA The correct model _ Meselson and Franklin Stahl's experiment to determine the correct DNA replication mode . Matthew Meselson • DNA IN ACTION • The genetic code Defining the gene _ matching the gene to protein sequence . -
Dna Learning Center
DNA LEARNING CENTER DNA LEARNING CENTER ADMINISTRATION INSTRUCTION MULTIMEDIA David Micklos Scott Bronson Susan Lauter Judy Cumella-Korabik Amanda McBrien Shirley Chan Nancy Daidola Danielle Sixsmith Chun-hua Yang Vin Torti Veronique Bourdeau Susan Conova Elna Carrasco Uwe Hilgert Maureen Cowan We stand at the threshold of a new century with the whole human genome stretched out before us. Messages from science and the popular media suggest a world of seemingly limitless opportunities to improve human health and productivity. Yet, at the turn of the last century, science and society faced a similar rush to exploit human genetics. The story of eugenics—humankind’s first venture into a “gene age”—holds a cautionary lesson for our current preoccupation with genes. Eugenics was the effort to apply principles of genetics to improve the human race. Most people equate eugenics with the atrocities committed for the sake of racial purity in Nazi Germany. Most are unaware of the “positive” eugenics movement, exemplified in England, which advocated voluntary efforts by families to improve their own heredity. Fewer still realize that a coercive, “negative” eugenics movement flourished in the United States, that it involved numerous prominent scientists and civic lead- ers, and that it made its intellectual home at the forerunner of the now prestigious Cold Spring Harbor Laboratory. During the first decade of the 20th century, eugenics was organized as a scientific field by the con- fluence of Mendelian genetics and experimental breeding. This synthesis was embodied by Charles Benedict Davenport, who is considered the father of the American eugenics movement. When Charles Da v e n p o r t arrived at Cold Spring Harbor in 1898, he assumed the directorship of The Biological La b o r a t o r y, a prog r essive, if somewhat sleepy, “summer camp” for the study of evolution. -

How Scientist/Founders Lead Successful
HOW SCIENTIST/FOUNDERS LEAD SUCCESSFUL BIOPHARMACEUTICAL ORGANIZATIONS: A STUDY OF THREE COMPANIES Lynn Johnson Langer A DISSERTATION Submitted to the Ph.D. in Leadership & Change Program of Antioch University in partial fulfillment of the requirements for the degree of Doctor of Philosophy May, 2008 This is to certify that the dissertation entitled: HOW SCIENTIST/FOUNDERS LEAD SUCCESSFUL BIOPHARMACEUTICAL ORGANIZATIONS: A STUDY OF THREE COMPANIES prepared by Lynn Johnson Langer is approved in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Leadership & Change. Approved by: ______________________________________________________________________ Alan E. Guskin, Ph.D., Chair date ______________________________________________________________________ Jon Wergin, Ph.D., Committee Member date ______________________________________________________________________ Mitch Kusy, Ph.D., Committee Member date ______________________________________________________________________ Alice Sapienza, DBA, External Reader date Copyright 2008 Lynn Johnson Langer All rights reserved Acknowledgements I arrive at this place in my journey to becoming a scholar supported in love and friendship by so many people. I must thank first and foremost my husband, Eric Langer, who has supported me in many ways, but particularly with my education. I thank my daughter, Julia Annemarie, my study partner. We shout across the hall to each other, complaining and laughing about all the work. I thank her for her support and the opportunity to be a role model. She never once complained about the plays and events I missed because I was away at a residency. I thank my son, Adam and his wife, Megan who through their lives, remind me to follow my dreams. I thank my son, Benjamin, who shows me that through hard work, we can accomplish great things. -

Discovery of the Secrets of Life Timeline
Discovery of the Secrets of Life Timeline: A Chronological Selection of Discoveries, Publications and Historical Notes Pertaining to the Development of Molecular Biology. Copyright 2010 Jeremy M. Norman. Date Discovery or Publication References Crystals of plant and animal products do not typically occur naturally. F. Lesk, Protein L. Hünefeld accidentally observes the first protein crystals— those of Structure, 36;Tanford 1840 hemoglobin—in a sample of dried menstrual blood pressed between glass & Reynolds, Nature’s plates. Hunefeld, Der Chemismus in der thierischen Organisation, Robots, 22.; Judson, Leipzig: Brockhaus, 1840, 158-63. 489 In his dissertation Louis Pasteur begins a series of “investigations into the relation between optical activity, crystalline structure, and chemical composition in organic compounds, particularly tartaric and paratartaric acids. This work focused attention on the relationship between optical activity and life, and provided much inspiration and several of the most 1847 HFN 1652; Lesk 36 important techniques for an entirely new approach to the study of chemical structure and composition. In essence, Pasteur opened the way to a consideration of the disposition of atoms in space.” (DSB) Pasteur, Thèses de Physique et de Chimie, Presentées à la Faculté des Sciences de Paris. Paris: Bachelier, 1847. Otto Funcke (1828-1879) publishes illustrations of crystalline 1853 hemoglobin of horse, humans and other species in his Atlas der G-M 684 physiologischen Chemie, Leizpig: W. Englemann, 1853. Charles Darwin and Alfred Russel Wallace publish the first exposition of the theory of natural selection. Darwin and Wallace, “On the Tendency of 1858 Species to Form Varieties, and on the Perpetuation of Varieties and G-M 219 Species by Natural Means of Selection,” J. -

Medicine@Yale
hree years after Yale College and he has discovered several new plant Tjoined with the Connecticut species, including species of milkweed Medical Society to establish the and balsamweed, His garden and Medical Institution of Yale College by conservatory at the Medical Institution an Act of the Legislature, thirty-seven are filled with plants that he uses to Students are soon arriving in New-Haven prepare his efficacious Medicines. from all corners of New England to Dr, JONATHAN KNIGHT, who commence studies in Medicine, Anatomy, graduated from Yale College five years Chemistry, and Materia Medica at the ago, studied Medicine in Philadelphia, new school. Seventeen members of the and his practice in Medicine and class come from Connecticut; the rest Surgery is familiar to many in the come from Vermont, New Hampshire, town. Dr. Knight will instruct the new and Massachusetts. Students in Anatomy. The Students, whose names, towns, The cost to the Students for the full and places of residence in New-Haven course of Lectures, described further in are listed here, met the requirement the Advertisement placed on this page for admission, to “produce satisfactory by Dr. Dwight, will be fifty dollars. evidence of a blameless life and The course will last six months, with conversation.” no vacation, and will be given to all The new Medical Institution has thirty-seven Students. During this a most illustrious and accomplished time, the Medical Professors will faculty, assembled by Dr. TIMOTHY perform Surgical Operations, gratis, DWIGHT, the President of Yale College. upon such patients as will consent to Dr. NATHAN SMITH, late of Hanover, be operated upon in presence of the New Hampshire, where he founded the Students of Medicine.