Slu-Gems-Book.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Integrated Nature of Metamemory and Memory
The Integrated Nature of Metamemory and Memory John Dunlosky and Robert A. Bjork Introduction Memory has been of interest to scholars and laypeople alike for over 2,000 years. In a rather gruesome example from antiquity, Cicero tells the story of Simonides (557– 468 BC), who discovered the method of loci, which is a powerful mental mnemonic for enhancing one’s memory. Simonides was at a banquet of a nobleman, Scopas. To honor him, Simonides sang a poem, but to Scopas’s chagrin, the poem also honored two young men, Castor and Pollux. Being upset, Scopas told Simonides that he was to receive only half his wage. Simonides was later called from the banquet, and legend has it that the banquet room collapsed, and all those inside were crushed. To help bereaved families identify the victims, Simonides reportedly was able to name every- one according to the place where they sat at the table, which gave him the idea that order brings strength to our memories and that to employ this ability people “should choose localities, then form mental images of things they wanted to store in their memory, and place these in the localities” (Cicero, 2001). Tis example highlights an early discovery that has had important applied impli- cations for improving the functioning of memory (see, e.g., Yates, 1997). Memory theory was soon to follow. Aristotle (385–322 BC) claimed that memory arises from three processes: Events are associated (1) through their relative similarity or (2) rela- tive dissimilarity and (3) when they co-occur together in space and time. -
Mnemonics in a Mnutshell: 32 Aids to Psychiatric Diagnosis
Mnemonics in a mnutshell: 32 aids to psychiatric diagnosis Clever, irreverent, or amusing, a mnemonic you remember is a lifelong learning tool ® Dowden Health Media rom SIG: E CAPS to CAGE and WWHHHHIMPS, mnemonics help practitioners and trainees recall Fimportant lists (suchCopyright as criteriaFor for depression,personal use only screening questions for alcoholism, or life-threatening causes of delirium, respectively). Mnemonics’ effi cacy rests on the principle that grouped information is easi- er to remember than individual points of data. Not everyone loves mnemonics, but recollecting diagnostic criteria is useful in clinical practice and research, on board examinations, and for insurance reimbursement. Thus, tools that assist in recalling di- agnostic criteria have a role in psychiatric practice and IMAGES teaching. JUPITER In this article, we present 32 mnemonics to help cli- © nicians diagnose: • affective disorders (Box 1, page 28)1,2 Jason P. Caplan, MD Assistant clinical professor of psychiatry • anxiety disorders (Box 2, page 29)3-6 Creighton University School of Medicine 7,8 • medication adverse effects (Box 3, page 29) Omaha, NE • personality disorders (Box 4, page 30)9-11 Chief of psychiatry • addiction disorders (Box 5, page 32)12,13 St. Joseph’s Hospital and Medical Center Phoenix, AZ • causes of delirium (Box 6, page 32).14 We also discuss how mnemonics improve one’s Theodore A. Stern, MD Professor of psychiatry memory, based on the principles of learning theory. Harvard Medical School Chief, psychiatric consultation service Massachusetts General Hospital How mnemonics work Boston, MA A mnemonic—from the Greek word “mnemonikos” (“of memory”)—links new data with previously learned information. -

Hippocampal–Caudate Nucleus Interactions Support Exceptional Memory Performance
Brain Struct Funct DOI 10.1007/s00429-017-1556-2 ORIGINAL ARTICLE Hippocampal–caudate nucleus interactions support exceptional memory performance Nils C. J. Müller1 · Boris N. Konrad1,2 · Nils Kohn1 · Monica Muñoz-López3 · Michael Czisch2 · Guillén Fernández1 · Martin Dresler1,2 Received: 1 December 2016 / Accepted: 24 October 2017 © The Author(s) 2017. This article is an open access publication Abstract Participants of the annual World Memory competitive interaction between hippocampus and caudate Championships regularly demonstrate extraordinary mem- nucleus is often observed in normal memory function, our ory feats, such as memorising the order of 52 playing cards findings suggest that a hippocampal–caudate nucleus in 20 s or 1000 binary digits in 5 min. On a cognitive level, cooperation may enable exceptional memory performance. memory athletes use well-known mnemonic strategies, We speculate that this cooperation reflects an integration of such as the method of loci. However, whether these feats the two memory systems at issue-enabling optimal com- are enabled solely through the use of mnemonic strategies bination of stimulus-response learning and map-based or whether they benefit additionally from optimised neural learning when using mnemonic strategies as for example circuits is still not fully clarified. Investigating 23 leading the method of loci. memory athletes, we found volumes of their right hip- pocampus and caudate nucleus were stronger correlated Keywords Memory athletes · Method of loci · Stimulus with each other compared to matched controls; both these response learning · Cognitive map · Hippocampus · volumes positively correlated with their position in the Caudate nucleus memory sports world ranking. Furthermore, we observed larger volumes of the right anterior hippocampus in ath- letes. -
CHAPTER 6: MEMORY STRATEGIES: MNEMONIC DEVICES in Order to Remember Information, You First Have to Find It Somewhere in Your Memory
CHAPTER 6: MEMORY STRATEGIES: MNEMONIC DEVICES In order to remember information, you first have to find it somewhere in your memory. To be successful in college you need to use active learning strategies that help you store information and retrieve it. Mnemonic devices can help you do that. Mnemonics are techniques for remembering information that is otherwise difficult to recall. The idea behind using mnemonics is to encode complex information in a way that is much easier to remember. Two common types of mnemonic devices are acronyms and acrostics. Acronyms Acronyms are words made up of the first letters of other words. As a mnemonic device, acronyms help you remember the first letters of items in a list, which in turn helps you remember the list itself. Instructor OLC to accompany 100% Online Student Success 1 Examples The following are examples of popular mnemonic acronyms: HOMES Huron, Ontario, Michigan, Erie, Superior Names of the Great Lakes FACE The letters of the treble clef notes in the spaces from bottom to top spells “FACE”. ROY G. BIV Red, Orange, Yellow, Green, Blue, Indigo, Colors of the spectrum Violet MRS GREN Movement, Respiration, Sensitivity, Growth, Common attributes of living Reproduction, Excretion, Nutrition things Create Your Own Acronym Now think of a few words you need to remember. This could be related to your studies, your work, or just a subject of interest. Five steps to creating acronyms are*: 1. List the information you need to learn in meaningful phrases. 2. Circle or underline a keyword in each phrase. 3. Write down the first letter of each keyword. -

The Three Amnesias
The Three Amnesias Russell M. Bauer, Ph.D. Department of Clinical and Health Psychology College of Public Health and Health Professions Evelyn F. and William L. McKnight Brain Institute University of Florida PO Box 100165 HSC Gainesville, FL 32610-0165 USA Bauer, R.M. (in press). The Three Amnesias. In J. Morgan and J.E. Ricker (Eds.), Textbook of Clinical Neuropsychology. Philadelphia: Taylor & Francis/Psychology Press. The Three Amnesias - 2 During the past five decades, our understanding of memory and its disorders has increased dramatically. In 1950, very little was known about the localization of brain lesions causing amnesia. Despite a few clues in earlier literature, it came as a complete surprise in the early 1950’s that bilateral medial temporal resection caused amnesia. The importance of the thalamus in memory was hardly suspected until the 1970’s and the basal forebrain was an area virtually unknown to clinicians before the 1980’s. An animal model of the amnesic syndrome was not developed until the 1970’s. The famous case of Henry M. (H.M.), published by Scoville and Milner (1957), marked the beginning of what has been called the “golden age of memory”. Since that time, experimental analyses of amnesic patients, coupled with meticulous clinical description, pathological analysis, and, more recently, structural and functional imaging, has led to a clearer understanding of the nature and characteristics of the human amnesic syndrome. The amnesic syndrome does not affect all kinds of memory, and, conversely, memory disordered patients without full-blown amnesia (e.g., patients with frontal lesions) may have impairment in those cognitive processes that normally support remembering. -
Working Memory Training: Assessing the Efficiency of Mnemonic Strategies
entropy Article Working Memory Training: Assessing the Efficiency of Mnemonic Strategies 1, 2 1 1, Serena Di Santo y, Vanni De Luca , Alessio Isaja and Sara Andreetta * 1 Cognitive Neuroscience, Scuola Internazionale Superiore di Studi Avanzati, I-34136 Trieste, Italy; [email protected] (S.D.S.); [email protected] (A.I.) 2 Scuola Peripatetica d’Arte Mnemonica (S.P.A.M.), 10125 Turin, Italy; [email protected] * Correspondence: [email protected] Current address: Center for Theoretical Neuroscience, Columbia University, New York, NY 10027, USA. y Received: 6 April 2020; Accepted: 18 May 2020; Published: 20 May 2020 Abstract: Recently, there has been increasing interest in techniques for enhancing working memory (WM), casting a new light on the classical picture of a rigid system. One reason is that WM performance has been associated with intelligence and reasoning, while its impairment showed correlations with cognitive deficits, hence the possibility of training it is highly appealing. However, results on WM changes following training are controversial, leaving it unclear whether it can really be potentiated. This study aims at assessing changes in WM performance by comparing it with and without training by a professional mnemonist. Two groups, experimental and control, participated in the study, organized in two phases. In the morning, both groups were familiarized with stimuli through an N-back task, and then attended a 2-hour lecture. For the experimental group, the lecture, given by the mnemonist, introduced memory encoding techniques; for the control group, it was a standard academic lecture about memory systems. In the afternoon, both groups were administered five tests, in which they had to remember the position of 16 items, when asked in random order. -

Mnemonic Devices
Mnemonic Devices Mnemonic devices are aids for improving one’s memory. These devices can be much more efficient than rote memory techniques (learning by simple repetition). Mnemonic devices may be effective because they generally attach new information to be learned to old information already mastered, or to catch words or phrases that are more easily remembered. Acronyms (catchwords) Ex) The Great Lakes—“HOMES" Huron, Ontario, Michigan, Erie, Superior Ex) The only spot in the U.S. four where states meet—“CANU” Colorado, Arizona, New Mexico, Utah Acrostics (catch phrases) Ex) The colors of the spectrum--“Roy G. Biv” Red, Orange, Yellow, Green, Blue, Indigo, Violet Ex) The order of the planets from the sun—“My very educated mother just served us nachos” Mercury Venus Earth Mars Jupiter Saturn Uranus Neptune Ex) The order of operations – “Please excuse my dear aunt Sally” Parenthesis Exponents Multiplication Division Addition Subtraction Jingles Ex) Days in each month—“Thirty days hath September, April, June, and November” Ex) Spelling generalization—“i before e except after c” Model Mnemonics • Using images to remember ideas Ex) The story arc's "mountain" shape illustrates how stories typically progress Notetaking with Mnemonics • While taking notes, use alliteration to facilitate recall. Alliteration occurs when words close to one another begin with the same letter or sound. Ex) Take the first sound of the subject and then pick topics you want to relate- "In Biology you can study bacteria, beasts, beings, and botanicals." Adapted from The Leader’s Guide for Supplemental Instruction, University of Missouri -Kansas City. . -
How to Develop a Perfect Memory Will Show You in Simple Language and Easy Stages
HOW TO DEVELOP A DOMINIC O’BRIEN Lybrary.com To my dear mother Pamela who is forever saying, ‘How does he do it!’ The author would like to thank Jon Stock for his invaluable assistance in preparing this book. This is an electronic republication by Lybrary.com of the first edition, 1993 by Pavilion Books Limited. Lybrary.com, PO Box 425281, Cambridge, MA 02142, USA www.lybrary.com ISBN 1-59561-006-5 Copyright © Dominic O’Brien 1993 Electronic Version Copyright © Dominic O’Brien 2005 All rights reserved. The Father of the Bride speech by Richard Curtis and Rowan Atkinson is reproduced by kind permission of The Peters, Fraser & Dunlop Group Ltd and PJB Management. Dominic O'Brien is the eight times winner of the The World Memory Championships and has a number of entries in the Guinness Book of Records including the memorisation of 54 packs of shuffled cards after just a single-sighting of each card. How does he do it? What is his system and how can it help YOU remember names, faces, telephone numbers, pass exams, learn languages, win at Trivial Pursuit and clean up at the Blackjack table? How to Develop a Perfect Memory will show you in simple language and easy stages. 1 INTRODUCTION I know what it is like to forget someone's name. In my time, I have forgotten appointments, telephone numbers, speeches, punch lines of jokes, directions, even whole chapters of my life. Up until recently, I was the most absent- minded, forgetful person you could imagine. I once saw a cartoon of two people dancing rather awkwardly at the Amnesiacs' Annual Ball. -

Mnemonics 1 TITLE PAGE the Use of Melodic and Rhythmic
Mnemonics 1 TITLE PAGE The Use of Melodic and Rhythmic Mnemonics To Improve Memory and Recall in Elementary Students in the Content Areas Orla C. Hayes Submitted in Partial Fulfillment of the Requirements for the Degree Master of Science in Education School of Education Dominican University of California San Rafael, CA May 2009 Mnemonics 2 ACKNOWLEDGEMENTS My sincere thanks to Dr. Madalienne Peters for her expertise, time, accessibility and endless patience with me throughout this process. Many thanks to my supportive classmates for their positive input and ever-present words of encouragement. A special thank you to my brother Robert, who encouraged me to embark on this worthy endeavor and gently prodded me along the sometimes bumpy road. Thank you to Suzanne Roybal and all the knowledgeable librarians at Dominican University of California. To Gary, thank you for your unyielding love and support, financially, technologically and emotionally. And to my two boys, whose unbridled joy and laughter keeps me smiling every day, thank you. Mnemonics 3 TABLE OF CONTENTS TITLE PAGE...................................................................................................................................... 1 ACKNOWLEDGEMENTS..................................................................................................................... 2 TABLE OF CONTENTS ....................................................................................................................... 3 ABSTRACT ...................................................................................................................................... -

Memory Enhancement for Educators. Fastback 365. INSTITUTION Phi Delta Kappa Educational Foundation, Bloomington, Ind
DOCUMENT RESUME ED 368 734 SP 035 194 AUTHOR Kelly, Evelyn B. TITLE Memory Enhancement for Educators. Fastback 365. INSTITUTION Phi Delta Kappa Educational Foundation, Bloomington, Ind. REPORT NO ISBN-0-87367-365-4 PUB DATE 94 NOTE 36p. AVAILABLE FROMPhi Delta Kappa, P.O. Box 789, Bloomington, IN 47402-0789. PUB TYPE Guides Classroom Use Teaching Guides (For Teacher) (052) EDRS PRICE MF01/PCO2 Plus Postage. DESCRIPTORS Elementary Secondary Education; Improvement Programs; *Learning Strategies; *Long Term Memory; *Mnemonics; *Recall (Psychology); *Recognition (Psychology); *Short Term Memory; Skill Development; Student Attitudes; Teaching Methods ABSTRACT This Fastback contends that educators are in the memory business, that memory is probably our mostmaligned faculty, that forgetting is a fact of life, and that overall memory skills can be learned. The booklet addresses the following questions: How justified are people's complaints about memory? How much is myth and how much is fact? What memory strategies can we learn and practice? and How can students be helped to learn memory techniques. Following an introduction, the publication is organizedinto six parts. The first part, "Don't Myth-Interpret Your Memory," provides a quiz that seeks to separate fact from fiction. Part two, "What is Memory?" discusses short-term and long-term memory and how memories actually form, and it provides an initial memory activity. Mnemonics, internal memory strategies, remembering names and faces, andexternal memory strategies are the subject of part three, "Memory Principles." The fourth section, "Helping Students Remember," covers teaching memory techniques to young children and describes the role of mnemonics in the teaching of literature. -
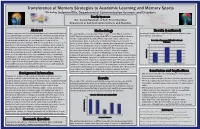
Transference of Memory Strategies to Academic Learning and Memory
Transference of Memory Strategies to Academic Learning and Memory Sports Nicholas Solomon Ellis, Department of Communication Sciences and Disorders Faculty Sponsors Drs. Crystal Randolph, & Ruth Renee Hannibal Department of Communication Sciences and Disorders Abstract Methodology Results (continued) Memory is the process of recalling what has been learned and retained The participant is a college student who began to learn MTs in September memory techniques were higher for the memory games than especially through associative mechanisms. Anatomically, this includes 2015. The participant initially learned the MTs to learn Spanish vocabulary the academic assessment. electrical impulses fired in our brains to relay information. When we and then subsequently used the MTs to help learn course content. The learn new information, we use our memories to help recall the participant was given 2 tasks, one academic learning assessment and 2 Percentage of Responses Attributable to Memory information stored in our brains. Without memory, there is no access to Techniques memory sports games. The academic learning assessment was created by a 120 using stored information. Mnemonics are techniques used to improve professor in the participant’s major department and included 12 questions and enhance memory. Other memory techniques include but are not from content learned in courses taken Fall 2015. The questions were 100 s e s limited to, the method of loci, peg systems, and phonetic systems. n 80 developed based on Bloom’s taxonomy and were related to language o p s E From these systems spawned competitions, memory sports, which R development, phonetics, and general knowledge of CSD. Each section f o 60 e g have created remarkable feats of memorization. -

The Arts of Memory Comparative Perspectives on a Mental Artifact
2012 | HAU: Journal of Ethnographic Theory 2 (2): 451–85 |Translation| The arts of memory Comparative perspectives on a mental artifact Carlo SEVERI, École des Hautes Études en Sciences Sociales Revised and updated by the author Translated from the French by Matthew Carey For linguists, anthropologists and archaeologists, the emblematic image always and everywhere preceded the appearance of the sign. This myth of a figurative language composed by icons—that form the opposite figure of writing—has deeply influenced Western tradition. In this article, I show that the logic of Native American Indian mnemonics (pictographs, khipus) cannot be understood from the ethnocentric question of the comparison with writing, but requires a truly comparative anthropology. Rather than trying to know if Native American techniques of memory are true scripts or mere mnemonics, we can explore the formal aspect both have in common, compare the mental processes they call for. We can ask if both systems belong to the same conceptual universe, to a mental language—to use Giambattista Vico’s phrase—that would characterize the Native American arts of memory. In this perspective, techniques of memory stop being hybrids or imprecise, and we will better understand their nature and functions as mental artifacts. Keywords: art, memory, pictographs, khipu, tradition, iconography There must in the nature of human things be a mental language common to all nations. This axiom is the principle of the hieroglyphs by which all nations spoke in the time of their first barbarism. Giambattista Vico, La scienza nuova, [1744] 1990 Social memory necessarily involves the remembrance of origins.