Verification Committee Concerning Hansen's Disease Problem
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Powerful Warriors and Influential Clergy Interaction and Conflict Between the Kamakura Bakufu and Religious Institutions
UNIVERSITY OF HAWAllllBRARI Powerful Warriors and Influential Clergy Interaction and Conflict between the Kamakura Bakufu and Religious Institutions A DISSERTATION SUBMITTED TO THE GRADUATE DIVISION OF THE UNIVERSITY OF HAWAI'I IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF DOCTOR OF PHILOSOPHY IN HISTORY MAY 2003 By Roy Ron Dissertation Committee: H. Paul Varley, Chairperson George J. Tanabe, Jr. Edward Davis Sharon A. Minichiello Robert Huey ACKNOWLEDGMENTS Writing a doctoral dissertation is quite an endeavor. What makes this endeavor possible is advice and support we get from teachers, friends, and family. The five members of my doctoral committee deserve many thanks for their patience and support. Special thanks go to Professor George Tanabe for stimulating discussions on Kamakura Buddhism, and at times, on human nature. But as every doctoral candidate knows, it is the doctoral advisor who is most influential. In that respect, I was truly fortunate to have Professor Paul Varley as my advisor. His sharp scholarly criticism was wonderfully balanced by his kindness and continuous support. I can only wish others have such an advisor. Professors Fred Notehelfer and Will Bodiford at UCLA, and Jeffrey Mass at Stanford, greatly influenced my development as a scholar. Professor Mass, who first introduced me to the complex world of medieval documents and Kamakura institutions, continued to encourage me until shortly before his untimely death. I would like to extend my deepest gratitude to them. In Japan, I would like to extend my appreciation and gratitude to Professors Imai Masaharu and Hayashi Yuzuru for their time, patience, and most valuable guidance. -

Nihontō Compendium
Markus Sesko NIHONTŌ COMPENDIUM © 2015 Markus Sesko – 1 – Contents Characters used in sword signatures 3 The nengō Eras 39 The Chinese Sexagenary cycle and the corresponding years 45 The old Lunar Months 51 Other terms that can be found in datings 55 The Provinces along the Main Roads 57 Map of the old provinces of Japan 59 Sayagaki, hakogaki, and origami signatures 60 List of wazamono 70 List of honorary title bearing swordsmiths 75 – 2 – CHARACTERS USED IN SWORD SIGNATURES The following is a list of many characters you will find on a Japanese sword. The list does not contain every Japanese (on-yomi, 音読み) or Sino-Japanese (kun-yomi, 訓読み) reading of a character as its main focus is, as indicated, on sword context. Sorting takes place by the number of strokes and four different grades of cursive writing are presented. Voiced readings are pointed out in brackets. Uncommon readings that were chosen by a smith for a certain character are quoted in italics. 1 Stroke 一 一 一 一 Ichi, (voiced) Itt, Iss, Ipp, Kazu 乙 乙 乙 乙 Oto 2 Strokes 人 人 人 人 Hito 入 入 入 入 Iri, Nyū 卜 卜 卜 卜 Boku 力 力 力 力 Chika 十 十 十 十 Jū, Michi, Mitsu 刀 刀 刀 刀 Tō 又 又 又 又 Mata 八 八 八 八 Hachi – 3 – 3 Strokes 三 三 三 三 Mitsu, San 工 工 工 工 Kō 口 口 口 口 Aki 久 久 久 久 Hisa, Kyū, Ku 山 山 山 山 Yama, Taka 氏 氏 氏 氏 Uji 円 円 円 円 Maru, En, Kazu (unsimplified 圓 13 str.) 也 也 也 也 Nari 之 之 之 之 Yuki, Kore 大 大 大 大 Ō, Dai, Hiro 小 小 小 小 Ko 上 上 上 上 Kami, Taka, Jō 下 下 下 下 Shimo, Shita, Moto 丸 丸 丸 丸 Maru 女 女 女 女 Yoshi, Taka 及 及 及 及 Chika 子 子 子 子 Shi 千 千 千 千 Sen, Kazu, Chi 才 才 才 才 Toshi 与 与 与 与 Yo (unsimplified 與 13 -

No.724 (May Issue)
NBTHK SWORD JOURNAL ISSUE NUMBER 724 May, 2017 Meito Kansho Examination of Important Swords Juyo Bunkazai Important culurual property Type: Tachi Owner: Hayashibara Museum Mei: Bishu ju Takamitsu saku Genkyo 22 nen, 7 gatsu bi Length: 2 shaku 5 sun 5 bu 4 rin (77.4 cm) Sori: 9 bu 4 rin (2.85 cm) Motohaba: 9 bu 2 rin (2.8 cm) Sakihaba: 4 bu 6 rin (1.4 cm) Motokasane: 2 bu (0.6 cm) Sakikasane: 1 bu 2 rin (0.35 cm) Kissaki length: 6 bu 5 rin (1.95 cm) Nakago length: 5 sun 9 bu 4 rin (18.0 cm) Nakago sori: 1 bu (0.3 rin) Commentary This is a shinogi zukuri tachi with an ihorimune, a narrow width, and a large difference in the widths at the moto and saki. There is a large koshi-sori with funbari, and there is a small kissaki. The jihada is itame mixed with mokume, there is some nagare jihada, the entire jihada is well forged, and there is a fine visible jihada. There are ji-nie, frequent chikei, very clear mizukage type utsuri at the koshimoto which almost looks like the yakiba, and a continuous pale jifu type utsuri. The hamon is chu-suguha mixed with ko-gunome and ko-notare. There are frequent ashi and yo, the hamon has a nioiguchi, there are dense ha-nie, some fine sunagashi, kinsuji, and a tight nioiguchi around the center. The entire hamon is gentle and clear. The boshi on the omote is straight with an o-maru, and the boshi on the the ura is yakizume. -
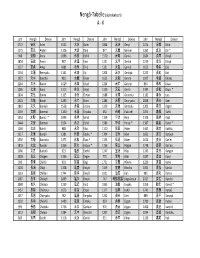
Nengo Alpha.Xlsx
Nengô‐Tabelle (alphabetisch) A ‐ K Jahr Nengō Devise Jahr Nengō Devise Jahr Nengō Devise Jahr Nengō Devise 1772 安永 An'ei 1521 大永 Daiei 1864 元治 Genji 1074 承保 Jōhō 1175 安元 Angen 1126 大治 Daiji 877 元慶 Genkei 1362 貞治 Jōji * 968 安和 Anna 1096 永長 Eichō 1570 元亀 Genki 1684 貞享 Jōkyō 1854 安政 Ansei 987 永延 Eien 1321 元亨 Genkō 1219 承久 Jōkyū 1227 安貞 Antei 1081 永保 Eihō 1331 元弘 Genkō 1652 承応 Jōō 1234 文暦 Benryaku 1141 永治 Eiji 1204 元久 Genkyū 1222 貞応 Jōō 1372 文中 Bunchū 983 永観 Eikan 1615 元和 Genna 1097 承徳 Jōtoku 1264 文永 Bun'ei 1429 永享 Eikyō 1224 元仁 Gennin 834 承和 Jōwa 1185 文治 Bunji 1113 永久 Eikyū 1319 元応 Gen'ō 1345 貞和 Jōwa * 1804 文化 Bunka 1165 永万 Eiman 1688 元禄 Genroku 1182 寿永 Juei 1501 文亀 Bunki 1293 永仁 Einin 1184 元暦 Genryaku 1848 嘉永 Kaei 1861 文久 Bunkyū 1558 永禄 Eiroku 1329 元徳 Gentoku 1303 嘉元 Kagen 1469 文明 Bunmei 1160 永暦 Eiryaku 650 白雉 Hakuchi 1094 嘉保 Kahō 1352 文和 Bunna * 1046 永承 Eishō 1159 平治 Heiji 1106 嘉承 Kajō 1444 文安 Bunnan 1504 永正 Eishō 1989 平成 Heisei * 1387 嘉慶 Kakei * 1260 文応 Bun'ō 988 永祚 Eiso 1120 保安 Hōan 1441 嘉吉 Kakitsu 1317 文保 Bunpō 1381 永徳 Eitoku * 1704 宝永 Hōei 1661 寛文 Kanbun 1592 文禄 Bunroku 1375 永和 Eiwa * 1135 保延 Hōen 1624 寛永 Kan'ei 1818 文政 Bunsei 1356 延文 Enbun * 1156 保元 Hōgen 1748 寛延 Kan'en 1466 文正 Bunshō 923 延長 Enchō 1247 宝治 Hōji 1243 寛元 Kangen 1028 長元 Chōgen 1336 延元 Engen 770 宝亀 Hōki 1087 寛治 Kanji 999 長保 Chōhō 901 延喜 Engi 1751 宝暦 Hōreki 1229 寛喜 Kanki 1104 長治 Chōji 1308 延慶 Enkyō 1449 宝徳 Hōtoku 1004 寛弘 Kankō 1163 長寛 Chōkan 1744 延享 Enkyō 1021 治安 Jian 985 寛和 Kanna 1487 長享 Chōkyō 1069 延久 Enkyū 767 神護景雲 Jingo‐keiun 1017 寛仁 Kannin 1040 長久 Chōkyū 1239 延応 En'ō -

Encyclopedia of Japanese History
An Encyclopedia of Japanese History compiled by Chris Spackman Copyright Notice Copyright © 2002-2004 Chris Spackman and contributors Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, Version 1.1 or any later version published by the Free Software Foundation; with no Invariant Sections, with no Front-Cover Texts, and with no Back-Cover Texts. A copy of the license is included in the section entitled “GNU Free Documentation License.” Table of Contents Frontmatter........................................................... ......................................5 Abe Family (Mikawa) – Azukizaka, Battle of (1564)..................................11 Baba Family – Buzen Province............................................... ..................37 Chang Tso-lin – Currency............................................... ..........................45 Daido Masashige – Dutch Learning..........................................................75 Echigo Province – Etō Shinpei................................................................ ..78 Feminism – Fuwa Mitsuharu................................................... ..................83 Gamō Hideyuki – Gyoki................................................. ...........................88 Habu Yoshiharu – Hyūga Province............................................... ............99 Ibaraki Castle – Izu Province..................................................................118 Japan Communist Party – Jurakutei Castle............................................135 -
Encyclopedia of Japanese History Version 0.3.1
Encyclopedia of Japanese History version 0.3.1 compiled by Chris Spackman July 6, 2002 2 Contents 1 Frontmatter 5 2 Main Entries: Abe—Zeami 15 A Chronological List of Emperors 281 B Prime Ministers, 1885 to Present 285 C Alphabetical List of the Prefectures 289 D Provinces and Corresponding Prefectures 291 E Chronological List of Nengo 295 F List of the Shogun¯ 303 G GNU Free Documentation License 305 Bibliography 315 Index 317 3 Chapter 1 Frontmatter Copyright Notice Copyright c 2002 Chris Spackman Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, Version 1.1 or any later version published by the Free Software Foundation; with no Invariant Sections, with no Front-Cover Texts, and with no Back-Cover Texts. A copy of the license is in- cluded in the section entitled “GNU Free Documentation License.” 5 6 CHAPTER 1. FRONTMATTER History This encyclopedia started as a web site back in 1998. As I added more and more pages, the limitations of html for a large project began to show, so in late 2000 I switched everything over to LATEX. This work was originally published under the Open Content License but I repub- lished it under the GNU Free Documentation License in March 2001. Please see the copyright section and the GNU License at the back of the book for more de- tails. 0.3.1 There are several new appendices, one of which is the list of emperors that used to be included in the emperor entry. -

Encyclopedia of Shinto Chronological Supplement
Encyclopedia of Shinto Chronological Supplement 『神道事典』巻末年表、英語版 Institute for Japanese Culture and Classics Kokugakuin University 2016 Preface This book is a translation of the chronology that appended Shinto jiten, which was compiled and edited by the Institute for Japanese Culture and Classics, Kokugakuin University. That volume was first published in 1994, with a revised compact edition published in 1999. The main text of Shinto jiten is translated into English and publicly available in its entirety at the Kokugakuin University website as "The Encyclopedia of Shinto" (EOS). This English edition of the chronology is based on the one that appeared in the revised version of the Jiten. It is already available online, but it is also being published in book form in hopes of facilitating its use. The original Japanese-language chronology was produced by Inoue Nobutaka and Namiki Kazuko. The English translation was prepared by Carl Freire, with assistance from Kobori Keiko. Translation and publication of the chronology was carried out as part of the "Digital Museum Operation and Development for Educational Purposes" project of the Institute for Japanese Culture and Classics, Organization for the Advancement of Research and Development, Kokugakuin University. I hope it helps to advance the pursuit of Shinto research throughout the world. Inoue Nobutaka Project Director January 2016 ***** Translated from the Japanese original Shinto jiten, shukusatsuban. (General Editor: Inoue Nobutaka; Tokyo: Kōbundō, 1999) English Version Copyright (c) 2016 Institute for Japanese Culture and Classics, Kokugakuin University. All rights reserved. Published by the Institute for Japanese Culture and Classics, Kokugakuin University, 4-10-28 Higashi, Shibuya-ku, Tokyo, Japan. -

Download the Japan Style Sheet, 3Rd Edition
JAPAN STYLE SHEET JAPAN STYLE SHEET THIRD EDITION The SWET Guide for Writers, Editors, and Translators SOCIETY OF WRITERS, EDITORS, AND TRANSLATORS www.swet.jp Published by Society of Writers, Editors, and Translators 1-1-1-609 Iwado-kita, Komae-shi, Tokyo 201-0004 Japan For correspondence, updates, and further information about this publication, visit www.japanstylesheet.com Cover calligraphy by Linda Thurston, third edition design by Ikeda Satoe Originally published as Japan Style Sheet in Tokyo, Japan, 1983; revised edition published by Stone Bridge Press, Berkeley, CA, 1998 © 1983, 1998, 2018 Society of Writers, Editors, and Translators All rights reserved No part of this book may be reproduced in any form without permission from the publisher Printed in Japan Contents Preface to the Third Edition 9 Getting Oriented 11 Transliterating Japanese 15 Romanization Systems 16 Hepburn System 16 Kunrei System 16 Nippon System 16 Common Variants 17 Long Vowels 18 Macrons: Long Marks 18 Arguments in Favor of Macrons 19 Arguments against Macrons 20 Inputting Macrons in Manuscript Files 20 Other Long-Vowel Markers 22 The Circumflex 22 Doubled Letters 22 Oh, Oh 22 Macron Character Findability in Web Documents 23 N or M: Shinbun or Shimbun? 24 The N School 24 The M School 24 Exceptions 25 Place Names 25 Company Names 25 6 C ONTENTS Apostrophes 26 When to Use the Apostrophe 26 When Not to Use the Apostrophe 27 When There Are Two Adjacent Vowels 27 Hyphens 28 In Common Nouns and Compounds 28 In Personal Names 29 In Place Names 30 Vernacular Style -

Eihei Dogen: Mystical Realist
Buddhism Eihei Do–gen, the founder of the Japanese So–to– Zen school, is considered one of KIM THE CLASSIC INTRODUCTION TO the world’s most remarkable religious philosophers. Eihei Do–gen: Mystical Realist is a comprehensive introduction to the genius of this brilliant thinker. DO¯ GEN’S LIFE AND TEACHING “Down through the years and through its earlier editions, it was always to Dr. Kim’s book that – I turned first in any matter relating to Dogen. Now from his retirement from a fine academic EIHEIDO career, we have the fruit of his lifetime of research and meditation. I am very grateful.” — ROBERTAITKEN, author of Taking the Path of Zen and The Morning Star “This book is an excellent comprehensive introduction to Do–gen’s massive corpus of intricate writings as well as to his elegantly simple yet profound practice. It stands as the best overall general introduction to Do–gen’s teaching.” – EIHEI GEN — from the new foreword by TAIGENDANLEIGHTON, editor and co-translator of Do–gen’s Extensive Record: A Translation of the Eihei Ko–roku and Visions of Awakening Space – and Time: Dogen and the Lotus Sutra DOGEN MYSTICALREALIST “While there have been many developments in the historical and philosophical understanding of Do–gen’s contribution to Zen Buddhism, Kim’s work still stands out for the depth and clarity of its elucidation of Do–gen as a religious thinker and practitioner.” MYSTICAL — PROFESSORMARKUNNO, Journal of Religious Ethics, and author of Shingon Refractions: Myoe and the Mantra of Light REALIST “Do–gen is no easy read—fortunately Kim’s book, itself a polished gem, expertly guides a reader into what is simultaneously rich and playful in Do–gen’s Buddhist vision.” — WILLIAMR.LAFLEUR, author of Awesome Nightfall: The Life, Times, and Poetry of Saigyo “An essential volume in any Do–gen library.” — ZOKETSUNORMANFISCHER, former abbot, San Francisco Zen Center, and author of Taking Our Places: The Buddhist Path to Truly Growing Up HEE-JINKIM is professor emeritus at the University of Oregon. -

Pearl in the Shrine a Genealogy of the Buddhist Jewel of the Japanese Sovereign
Japanese Journal of Religious Studies 2002 29/1-2 Pearl in the Shrine A Genealogy of the Buddhist Jewel of the Japanese Sovereign Brian O. R uppert This study attempts to re-imagine early Japanese sovereignty through an examination of the relationship between the so-called “three regalia ” of the ruler and Buddhism. Based on an analysis of relevant primary sources in printed and archival collections as well as drawing on the recent research of Japanese scholars such as Abe Yasurd, Shirayama Yoshitard and Sato Hiroo, tms paper focuses especially on the connection between the jewel among the regalia and the wish-fulfilling' jewel of esoteric Buddhism to argue that Shinto as we know it is inexorably linked with Buddhism. Cler ics of Kenmitsu Buddhist traditions, together with the sovereigns who patronized them, constituted by the fourteenth century a milieu that assumed possession of the remlia guaranteed royal sovereignty—a view that was produced primarily within and through the theories and practices of esoteric Buddhism. This conclusion enables us not only to reenvision the Buddmst character of Japanese sovereignty, but also to embark on a renewed examination of the Buddhist roots of royal Shinto discourse and ideology. Keywords: Nyoi hdju — relics — reffalia — Ise — Tsukai — Shinto — Kitabatake Chikafusa This study began with a query: How did people come to the belief that the shrine of the royal family, Ise Daymgru 伊勢大ネ中宮,enshrined relics, even though it was the only major shrine (yashiro 社,jin ja 神社) in the country that was apparently not an object of the governmental Buddha Relics Offering marking royal accession? During the course of research on relics, I was surprised to notice that people believed Ise Daijmgu enshrined relics. -

Tendai Buddhist Rituals, Iconography, and Veneration in Japan and China*
On the ‘Shintō’ Statues of Matsuo Shrine: Tendai Buddhist Rituals, Iconography, and Veneration in Japan and China* GEORGE A. KEYWORTH University of Saskatchewan [email protected] Keywords: Shintō statues, Matsuo shrine, Enchin, Tendai Buddhism, Shinra myōjin, Japanese history DOI: https://dx.doi.org/10.15239/hijbs.01.02.03 Abstract: Matsuno’o (Matsuo) shrine possesses some of the oldest statues of kami in Japan. A large statue of the male deity Ōyamakui may have been sponsored by Enchin (814–891), thereby illustrating how early we can document connections between the Tendaishū monastic institutions of Enryakuji and Miidera (Onjōji) and Matsuo shrine. In this paper I introduce the statues kept in the Shinzōkan at Matsuo shrine and discuss several key historical documents that tie Matsuo shrine with the Tendai Buddhist establishment in medieval Japan. I also demonstrate how statues of kami also now kept in the Shinzōkan speak to the sponsorship of the Matsuo shrine manuscript Buddhist canon by father and son shrine priests (kannushi) Hata no Chikatō and Hata no Yorichika during the twelfth century. Finally, I discuss a colophon from 1558 that shows how the Matsuo kami * This research is supported by an Insight Grant from the Social Sciences and Humanities Research Council of Canada. The following abbreviations are used throughout: 70 Hualin International Journal of Buddhist Studies, 1.2 (2018): 70–110 ‘SHINTŌ’ STATUES OF MATSUO SHRINE 71 shrine-temple complex (jingūji) maintained a special ritual connec- tion to Enchin and the kami associated with Miidera through the sixteenth century. NBZ Dai Nihon bukkyō zensho [Complete Buddhist 大日本佛教全書 Works of Japan]. -

FINE JAPANESE ART Thursday 10 November 2016
FINE JAPANESE ART Thursday 10 November 2016 SPECIALIST AND AUCTION ENQUIRIES LONDON Suzannah Yip Yoko Chino Masami Yamada NEW YORK Jeff Olson SENIOR CONSULTANTS Neil Davey Joe Earle FINE JAPANESE ART Thursday 10 November 2016 at 1pm 101 New Bond Street, London VIEWING ENQUIRIES CUSTOMER SERVICES Please see page 2 for bidder Saturday 5 November Specialist, Head of Department Monday to Friday 8.30 to 6.00 information including after-sale 11am to 5pm Suzannah Yip +44 (0) 20 7447 7447 collection and shipment Sunday 6 November +44 (0) 20 7468 8368 11am to 5pm [email protected] Please see page 4 for bidder For the sole purpose of providing Monday 7 November information including after-sale estimates in three currencies in 9am to 7.30pm Cataloguer collection and shipment the catalogue the conversion Tuesday 8 November Yoko Chino has been made at the exchange 9am to 4.30pm +44 (0) 20 7468 8372 Physical Condition of Lots in rate of approx. Wednesday 9 November [email protected] this Auction £1: ¥128.1115 9am to 4.30pm £1: USD1.2400 Department Assistant PLEASE NOTE THAT THERE Please note that this rate may well SALE NUMBER: Masami Yamada IS NO REFERENCE IN THIS have changed at the date of CATALOGUE TO THE PHYSICAL the auction. 23270 +44 (0) 20 7468 8217 [email protected] CONDITION OF ANY LOT. INTENDING BIDDERS MUST お品物のコンディションについて CATALOGUE: Senior Consultants SATISFY THEMSELVES AS TO £25.00 Neil Davey THE CONDITION OF ANY LOT 本カタログにはお品物の損傷等 +44 (0) 20 7468 8288 AS SPECIFIED IN CLAUSE 15 コンディションの記述は記載 BIDS [email protected] OF THE NOTICE TO BIDDERS されていないことを、予めご了 +44 (0) 20 7447 7447 CONTAINED AT THE END OF 承ください。入札をご希望の +44 (0) 20 7447 7401 fax Joe Earle THIS CATALOGUE.