The Role of DNA Damage-Induced Cellular Senescence in the Pathophysiology of Mtbi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
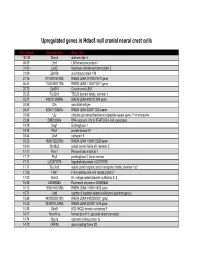
Supp Table 1.Pdf
Upregulated genes in Hdac8 null cranial neural crest cells fold change Gene Symbol Gene Title 134.39 Stmn4 stathmin-like 4 46.05 Lhx1 LIM homeobox protein 1 31.45 Lect2 leukocyte cell-derived chemotaxin 2 31.09 Zfp108 zinc finger protein 108 27.74 0710007G10Rik RIKEN cDNA 0710007G10 gene 26.31 1700019O17Rik RIKEN cDNA 1700019O17 gene 25.72 Cyb561 Cytochrome b-561 25.35 Tsc22d1 TSC22 domain family, member 1 25.27 4921513I08Rik RIKEN cDNA 4921513I08 gene 24.58 Ofa oncofetal antigen 24.47 B230112I24Rik RIKEN cDNA B230112I24 gene 23.86 Uty ubiquitously transcribed tetratricopeptide repeat gene, Y chromosome 22.84 D8Ertd268e DNA segment, Chr 8, ERATO Doi 268, expressed 19.78 Dag1 Dystroglycan 1 19.74 Pkn1 protein kinase N1 18.64 Cts8 cathepsin 8 18.23 1500012D20Rik RIKEN cDNA 1500012D20 gene 18.09 Slc43a2 solute carrier family 43, member 2 17.17 Pcm1 Pericentriolar material 1 17.17 Prg2 proteoglycan 2, bone marrow 17.11 LOC671579 hypothetical protein LOC671579 17.11 Slco1a5 solute carrier organic anion transporter family, member 1a5 17.02 Fbxl7 F-box and leucine-rich repeat protein 7 17.02 Kcns2 K+ voltage-gated channel, subfamily S, 2 16.93 AW493845 Expressed sequence AW493845 16.12 1600014K23Rik RIKEN cDNA 1600014K23 gene 15.71 Cst8 cystatin 8 (cystatin-related epididymal spermatogenic) 15.68 4922502D21Rik RIKEN cDNA 4922502D21 gene 15.32 2810011L19Rik RIKEN cDNA 2810011L19 gene 15.08 Btbd9 BTB (POZ) domain containing 9 14.77 Hoxa11os homeo box A11, opposite strand transcript 14.74 Obp1a odorant binding protein Ia 14.72 ORF28 open reading -

A B-Cell Receptor-Related Gene Signature Predicts Survival in Mantle
Published Ahead of Print on February 22, 2018, as doi:10.3324/haematol.2017.184325. Copyright 2018 Ferrata Storti Foundation. A B-cell receptor-related gene signature predicts survival in mantle cell lymphoma: results from the “Fondazione Italiana Linfomi” MCL-0208 trial by Riccardo Bomben, Simone Ferrero, Tiziana D'Agaro, Michele Dal Bo, Alessandro Re, Andrea Evangelista, Angelo Michele Carella, Alberto Zamò, Umberto Vitolo, Paola Omedè, Chiara Rusconi, Luca Arcaini, Luigi Rigacci, Stefano Luminari, Andrea Piccin, Delong Liu, Adrien Wiestner, Gianluca Gaidano, Sergio Cortelazzo, Marco Ladetto, and Valter Gattei Haematologica 2018 [Epub ahead of print] Citation: Riccardo Bomben, Simone Ferrero, Tiziana D'Agaro, Michele Dal Bo, Alessandro Re, Andrea Evangelista, Angelo Michele Carella, Alberto Zamò, Umberto Vitolo, Paola Omedè, Chiara Rusconi, Luca Arcaini, Luigi Rigacci, Stefano Luminari, Andrea Piccin, Delong Liu, Adrien Wiestner, Gianluca Gaidano, Sergio Cortelazzo, Marco Ladetto, and Valter Gattei. A B-cell receptor-related gene signature predicts survival in mantle cell lymphoma: results from the “Fondazione Italiana Linfomi” MCL-0208 trial. Haematologica. 2018; 103:xxx doi:10.3324/haematol.2017.184325 Publisher's Disclaimer. E-publishing ahead of print is increasingly important for the rapid dissemination of science. Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts that have completed a regular peer review and have been accepted for publication. E-publishing of this PDF file has been approved by the authors. After having E-published Ahead of Print, manuscripts will then undergo technical and English editing, typesetting, proof correction and be presented for the authors' final approval; the final version of the manuscript will then appear in print on a regular issue of the journal. -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -

Identifying Lineage Relationships in Human T Cell Populations
Identifying lineage relationships in human T cell populations by Celia Lara Menckeberg A thesis submitted to The University of Birmingham for the degree of DOCTOR OF PHILOSOPHY School of Immunity and Infection College of Medical and Dental Sciences The University of Birmingham December 2010 University of Birmingham Research Archive e-theses repository This unpublished thesis/dissertation is copyright of the author and/or third parties. The intellectual property rights of the author or third parties in respect of this work are as defined by The Copyright Designs and Patents Act 1988 or as modified by any successor legislation. Any use made of information contained in this thesis/dissertation must be in accordance with that legislation and must be properly acknowledged. Further distribution or reproduction in any format is prohibited without the permission of the copyright holder. ii ABSTRACT CD4+ and CD8+ T cell populations can be divided into subpopulations based on expression of surface markers CCR7 and CD45RA. The resulting populations are referred to as naive, central memory, effector memory and effector memory RA+ (EMRA). The aim of this study was to identify potential lineage relationships between these subpopulations for both CD4+ and CD8+ T cells through microarray analysis. The genes found to distinguish between these subpopulations include many molecules with known functions in T cell differentiation, including CCR7, CD45RA, granzymes, L-selectin and TNF receptors. Several genes from the tetraspanin family of proteins were found to be differentially expressed at mRNA and protein level; suggesting a possible role for these genes in CD4+ and CD8+ T cell activation, migration and lysosomal function. -

View / Download 3.3 Mb
Identification of Mechanisms and Pathways Involved in MLL2-Mediated Tumorigenesis by Chun-Chi Chang Department of Pathology Duke University Date:_______________________ Approved: ___________________________ Yiping He, Supervisor ___________________________ Salvatore Pizzo ___________________________ Hai Yan Thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in the Department of Pathology in the Graduate School of Duke University 2013 ABSTRACT Identification of Mechanisms and Pathways Involved in MLL2-Mediated Tumorigenesis by Chun-Chi Chang Department of Pathology Duke University Date:_______________________ Approved: ___________________________ Yiping He, Supervisor ___________________________ Salvatore Pizzo ___________________________ Hai Yan An abstract of a thesis submitted in partial fulfillment of the requirements for the degree of Master of Science in the Department of Pathology in the Graduate School of Duke University 2013 Copyright by Chun-Chi Chang 2013 Abstract Myeloid/lymphoid or mixed-lineage leukemia (MLL)-family genes encode histone lysine methyltransferases that play important roles in epigenetic regulation of gene transcription, and these genes are frequently mutated in human cancers. While MLL1 and MLL4 have been the most extensively studied, MLL2 and its homolog MLL3 are not well-understood. Specifically, little is known regarding the extent of global MLL2 involvement in the regulation of gene expression and the mechanism underlying its alterations in mediating tumorigenesis. To study the role of MLL2 in tumorigenesis, we somatically knocked out MLL2 in a colorectal carcinoma cell line, HCT116. We observed that the MLL2 loss of function results in significant reduction of cell growth and multinuclear morphology. We further profiled MLL2 regulated genes and pathways by analyzing gene expression in MLL2 wild-type versus MLL2-null isogenic cell lines. -

Supp Table 6.Pdf
Supplementary Table 6. Processes associated to the 2037 SCL candidate target genes ID Symbol Entrez Gene Name Process NM_178114 AMIGO2 adhesion molecule with Ig-like domain 2 adhesion NM_033474 ARVCF armadillo repeat gene deletes in velocardiofacial syndrome adhesion NM_027060 BTBD9 BTB (POZ) domain containing 9 adhesion NM_001039149 CD226 CD226 molecule adhesion NM_010581 CD47 CD47 molecule adhesion NM_023370 CDH23 cadherin-like 23 adhesion NM_207298 CERCAM cerebral endothelial cell adhesion molecule adhesion NM_021719 CLDN15 claudin 15 adhesion NM_009902 CLDN3 claudin 3 adhesion NM_008779 CNTN3 contactin 3 (plasmacytoma associated) adhesion NM_015734 COL5A1 collagen, type V, alpha 1 adhesion NM_007803 CTTN cortactin adhesion NM_009142 CX3CL1 chemokine (C-X3-C motif) ligand 1 adhesion NM_031174 DSCAM Down syndrome cell adhesion molecule adhesion NM_145158 EMILIN2 elastin microfibril interfacer 2 adhesion NM_001081286 FAT1 FAT tumor suppressor homolog 1 (Drosophila) adhesion NM_001080814 FAT3 FAT tumor suppressor homolog 3 (Drosophila) adhesion NM_153795 FERMT3 fermitin family homolog 3 (Drosophila) adhesion NM_010494 ICAM2 intercellular adhesion molecule 2 adhesion NM_023892 ICAM4 (includes EG:3386) intercellular adhesion molecule 4 (Landsteiner-Wiener blood group)adhesion NM_001001979 MEGF10 multiple EGF-like-domains 10 adhesion NM_172522 MEGF11 multiple EGF-like-domains 11 adhesion NM_010739 MUC13 mucin 13, cell surface associated adhesion NM_013610 NINJ1 ninjurin 1 adhesion NM_016718 NINJ2 ninjurin 2 adhesion NM_172932 NLGN3 neuroligin -

Supplemental Table S1. Primers for Sybrgreen Quantitative RT-PCR Assays
Supplemental Table S1. Primers for SYBRGreen quantitative RT-PCR assays. Gene Accession Primer Sequence Length Start Stop Tm GC% GAPDH NM_002046.3 GAPDH F TCCTGTTCGACAGTCAGCCGCA 22 39 60 60.43 59.09 GAPDH R GCGCCCAATACGACCAAATCCGT 23 150 128 60.12 56.52 Exon junction 131/132 (reverse primer) on template NM_002046.3 DNAH6 NM_001370.1 DNAH6 F GGGCCTGGTGCTGCTTTGATGA 22 4690 4711 59.66 59.09% DNAH6 R TAGAGAGCTTTGCCGCTTTGGCG 23 4797 4775 60.06 56.52% Exon junction 4790/4791 (reverse primer) on template NM_001370.1 DNAH7 NM_018897.2 DNAH7 F TGCTGCATGAGCGGGCGATTA 21 9973 9993 59.25 57.14% DNAH7 R AGGAAGCCATGTACAAAGGTTGGCA 25 10073 10049 58.85 48.00% Exon junction 9989/9990 (forward primer) on template NM_018897.2 DNAI1 NM_012144.2 DNAI1 F AACAGATGTGCCTGCAGCTGGG 22 673 694 59.67 59.09 DNAI1 R TCTCGATCCCGGACAGGGTTGT 22 822 801 59.07 59.09 Exon junction 814/815 (reverse primer) on template NM_012144.2 RPGRIP1L NM_015272.2 RPGRIP1L F TCCCAAGGTTTCACAAGAAGGCAGT 25 3118 3142 58.5 48.00% RPGRIP1L R TGCCAAGCTTTGTTCTGCAAGCTGA 25 3238 3214 60.06 48.00% Exon junction 3124/3125 (forward primer) on template NM_015272.2 Supplemental Table S2. Transcripts that differentiate IPF/UIP from controls at 5%FDR Fold- p-value Change Transcript Gene p-value p-value p-value (IPF/UIP (IPF/UIP Cluster ID RefSeq Symbol gene_assignment (Age) (Gender) (Smoking) vs. C) vs. C) NM_001178008 // CBS // cystathionine-beta- 8070632 NM_001178008 CBS synthase // 21q22.3 // 875 /// NM_0000 0.456642 0.314761 0.418564 4.83E-36 -2.23 NM_003013 // SFRP2 // secreted frizzled- 8103254 NM_003013 -

In Vivo and in Vitro Analysis of Dll1 and Pax6 Function in the Adult Mouse Pancreas
TECHNISCHE UNIVERSITÄT MÜNCHEN Lehrstuhl für Experimentelle Genetik In vivo and in vitro analysis of Dll1 and Pax6 function in the adult mouse pancreas Davide Cavanna Vollständiger Abdruck der von der Fakultät Wissenschaftszentrum Weihenstephan für Ernährung, Landnutzung und Umwelt der Technischen Universität München zur Erlangung des akademischen Grades eines Doktors der Naturwissenschaften genehmigten Dissertation. Vorsitzender: Univ.-Prof. Dr. D. Langosch Prüfer der Dissertation: 1. Univ.-Prof. Dr. M. Hrabé de Angelis 2. Univ.-Prof. A. Schnieke, Ph.D. Die Dissertation wurde am 03.07.2013 bei der Technischen Universität München eingereicht und durch die Fakultät Wissenschaftszentrum Weihenstephan für Ernährung, Landnutzung und Umwelt am 10.12.2013 angenommen. I. Table of contents I. TABLE OF CONTENTS .................................................................................................. I II. FIGURES AND TABLES ................................................................................................ V III. ABBREVIATIONS ................................................................................................. VIII IV. PUBLICATIONS, TALKS, AND POSTERS ................................................................... XI V. ACKNOWLEDGMENTS .............................................................................................. XII VI. AFFIRMATION ..................................................................................................... XIV 1. SUMMARY/ZUSAMMENFASSUNG ............................................................................ -

Supplemental Materials
The infection-tolerant mammalian reservoir of Lyme disease and other zoonoses broadly counters the inflammatory effects of endotoxin Supplemental Materials Figures S1-S5 Tables S1-S20 Figure S1. Digital photograph of two adult Peromyscus leucopus with exudative conjunctivitis and huddled together. The animals had received 10 mg/gm body of Escherichia coli lipopolysaccharide intraperitoneally the day before. Figure S2. Species- and tissue-specific responses to LPS. Independent differential gene expression analysis of RNA-seq data were performed for blood, spleen, and liver tissues of P. leucopus and M. musculus collected 4 h after injection with LPS or buffer alsone as control. These are represented as volcano plots with range- adjusted scales for the log2-transformed fold-changes on x-axes and log10-transformed FDR p values on y- axes. Colors of symbols denote the following: red, up-regulated gene with absolute fold-change > 4.0 and p value < 0.05; purple, down-regulated gene with absolute fold-change > 4.0 and p value < 0.05; and gray, all others. Numbers at the top left and right corners in each plot respresent numbers of down- and up-regulated genes, respectively. Figure 3 is same data with constant scales for x- and y-axes across the plots. Numerical values for each gene in the 6 datasets are provided in Tables S4-S9. Figure S3. Correlation of IL-10 and IL-10 P. leucopus and M. musculus from RNA-seq of spleen and of Figure 6B and TaBle S14. The scatter plot is log10 values of normalized unique reads of one coding sequence against another for each of the four groups, as defined in the legend for Figure 6 and indicated By different symBols. -

Universitat Aut`Onoma De Barcelona Towards Objective Human Brain
Universitat Aut`onoma de Barcelona Departament de Bioqu´ımica i Biologia Molecular Towards Objective Human Brain Tumours Classification using DNA microarrays Dissertation for the degree of Doctor of Biochemistry and Molecular Biology presented by Xavier Castells Domingo This work was performed at the Department of Biochemistry and Molecular Biology of the Universitat Aut`onoma de Barcelona under the supervision of Dr. Carles Ar´us Caralt´o, Dr. Joaqu´ın Ari˜no Carmona and Dr. Anna Barcel´o Vernet Undersigned by Dr. Carles Ar´us Caralt´o Dr. Joaqu´ın Ari˜no Carmona Dr. Anna Barcel´oVernet Xavier Castells Domingo Cerdanyola del Vall`es, 7 May 2009 En agra¨ıment a totes les persones que van decidir donar un tros de bi`opsia al noste grup. Especialment vull dedicar aquesta tesi a la mem`oriade les persones que han mort durant el transcurs de la meva tesi, i de les quals he tingut el gran honor de poder extreure RNA de les seves bi`opsies. Contents Abbreviations xvii 1 INTRODUCTION1 INTRODUCTION1 1.1 Overview on human brain tumours (HBT) . .3 1.1.1 Incidence and mortality of HBT . .3 1.1.2 Description of HBT . .3 1.1.2.1 Diagnosis of HBT in current clinical practice . .3 1.1.2.2 Overview on HBT classification . .5 1.1.3 World Health Organization (WHO) classification criteria . .5 1.1.3.1 Historical overview . .5 1.1.3.2 Entities, variants and patterns . .6 1.1.3.3 Malignancy grade schemes . .7 1.1.3.4 Differences between classification schemes . .7 1.1.3.5 Survival of patients suffering from HBT . -

Autocrine IFN Signaling Inducing Profibrotic Fibroblast Responses By
Downloaded from http://www.jimmunol.org/ by guest on September 23, 2021 Inducing is online at: average * The Journal of Immunology , 11 of which you can access for free at: 2013; 191:2956-2966; Prepublished online 16 from submission to initial decision 4 weeks from acceptance to publication August 2013; doi: 10.4049/jimmunol.1300376 http://www.jimmunol.org/content/191/6/2956 A Synthetic TLR3 Ligand Mitigates Profibrotic Fibroblast Responses by Autocrine IFN Signaling Feng Fang, Kohtaro Ooka, Xiaoyong Sun, Ruchi Shah, Swati Bhattacharyya, Jun Wei and John Varga J Immunol cites 49 articles Submit online. Every submission reviewed by practicing scientists ? is published twice each month by Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts http://jimmunol.org/subscription Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html http://www.jimmunol.org/content/suppl/2013/08/20/jimmunol.130037 6.DC1 This article http://www.jimmunol.org/content/191/6/2956.full#ref-list-1 Information about subscribing to The JI No Triage! Fast Publication! Rapid Reviews! 30 days* Why • • • Material References Permissions Email Alerts Subscription Supplementary The Journal of Immunology The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2013 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. This information is current as of September 23, 2021. The Journal of Immunology A Synthetic TLR3 Ligand Mitigates Profibrotic Fibroblast Responses by Inducing Autocrine IFN Signaling Feng Fang,* Kohtaro Ooka,* Xiaoyong Sun,† Ruchi Shah,* Swati Bhattacharyya,* Jun Wei,* and John Varga* Activation of TLR3 by exogenous microbial ligands or endogenous injury-associated ligands leads to production of type I IFN. -

Identifikation Von Kardiomyozyten-Differenzierungs-Genen Durch Einen Sirna-Basierenden Screeningansatz
Identifikation von Kardiomyozyten-Differenzierungs-Genen durch einen siRNA-basierenden Screeningansatz Inaugural-Dissertation Zur Erlangung des Doktorgrades der Naturwissenschaften (Dr. rer. nat.) An der Justus Liebig Universität Gießen Fachbereich 08 „Biologie und Chemie“ angefertigt am Max-Planck-Institut für Herz- und Lungenforschung Bad Nauheim vorgelegt von Stefanie Köhler-Bachmann aus Hilden März 2011 Dekan: Prof. Dr. Volkmar Wolters 1.Gutachter: Prof. Dr. Adriaan Dorresteijn 2.Gutachter: Prof. Dr. Dr. Thomas Braun Tag der mündlichen Prüfung: Unsere Bestimmung verfügt über uns, auch wenn wir sie noch nicht kennen; es ist die Zukunft, die unserm Heute die Regel gibt. Friedrich Nietzsche Menschliches, Allzumenschliches Inhalt Abkürzungen _____________________________________ 1 1. Einleitung ______________________________________ 3 1.1. Die frühe Entwicklung des Herzens ____________________________________ 5 1.1.1. Die Bildung der Keimblätter: Gastrulation in Vertebraten _______________ 6 1.1.2. Bildung des kardialen Mesoderms_______________________________________ 8 1.1.3. Frühe Morphogenese des embryonalen Herzens _______________________ 11 1.2. in vitro Differenzierung embryonaler Stammzellen _________________ 12 1.2.1. Differenzierung von Kardiomyozyten aus murinen Embryonalen Stammzellen __________________________________________________________ 14 1.3. RNA Interferenz ________________________________________________________ 16 1.3.1. Vektor-basierende Expressions-Systeme für Säugerzellen _____________ 21 1.3.2. siRNA Bibliotheken