Laboratory Diagnosis Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Hematological Complications of Alcoholism
The Hematological Complications of Alcoholism HAROLD S. BALLARD, M.D. Alcohol has numerous adverse effects on the various types of blood cells and their functions. For example, heavy alcohol consumption can cause generalized suppression of blood cell production and the production of structurally abnormal blood cell precursors that cannot mature into functional cells. Alcoholics frequently have defective red blood cells that are destroyed prematurely, possibly resulting in anemia. Alcohol also interferes with the production and function of white blood cells, especially those that defend the body against invading bacteria. Consequently, alcoholics frequently suffer from bacterial infections. Finally, alcohol adversely affects the platelets and other components of the blood-clotting system. Heavy alcohol consumption thus may increase the drinker’s risk of suffering a stroke. KEY WORDS: adverse drug effect; AODE (alcohol and other drug effects); blood function; cell growth and differentiation; erythrocytes; leukocytes; platelets; plasma proteins; bone marrow; anemia; blood coagulation; thrombocytopenia; fibrinolysis; macrophage; monocyte; stroke; bacterial disease; literature review eople who abuse alcohol1 are at both direct and indirect. The direct in the number and function of WBC’s risk for numerous alcohol-related consequences of excessive alcohol increases the drinker’s risk of serious Pmedical complications, includ- consumption include toxic effects on infection, and impaired platelet produc- ing those affecting the blood (i.e., the the bone marrow; the blood cell pre- tion and function interfere with blood cursors; and the mature red blood blood cells as well as proteins present clotting, leading to symptoms ranging in the blood plasma) and the bone cells (RBC’s), white blood cells from a simple nosebleed to bleeding in marrow, where the blood cells are (WBC’s), and platelets. -

Hematology Unit Lab 1 Review Material
Hematology Unit Lab 1 Review Material Objectives Laboratory instructors: 1. Facilitate lab discussion and answer questions Students: 1. Review the introductory material below 2. Study and review the assigned cases and questions in small groups before the Lab. This includes the pathological material using Virtual Microscopy 3. Be prepared to present your cases, questions and answers to the rest of your Lab class during the Lab Erythropoiesis: The process of red blood cell (RBC) production • Characterized by: − Increasing hemoglobin synthesis Erythroid maturation stages (Below): − Decreasing cell size - Average of 4 cell divisions during maturation − Decreasing cytoplasmic basophilia [One pronormoblast gives rise to 16 red cells] (increasing pink color) - pronormoblast → reticulocyte = 7 days − Progressive chromatin condensation of the - reticulocytes → mature RBC =1-2 days nuclei − Extrusion of nucleus (orthochromatic stage) − Extruded nuclei are subsequently phagocytized − Loss of mitotic capability after the early stage of polychromatophilic normoblast • Picture below: Erythroid progenitors (normoblasts) cluster around macrophages (arrows) in the bone marrow and spleen • Macrophages store iron • Iron is transferred from macrophages to erythroid precursor cells • Iron is used by normoblasts for hemoglobin synthesis aka nucleated rbc aka reticulocyte 1 Mature Red Blood Cell 7-8 microns; round / ovoid biconcave disc with orange-red cytoplasm, no RNA, no nucleus; survives ~120 days in circulation Classification of Anemia by Morphology 1. -

Complete Blood Count in Primary Care
Complete Blood Count in Primary Care bpac nz better medicine Editorial Team bpacnz Tony Fraser 10 George Street Professor Murray Tilyard PO Box 6032, Dunedin Clinical Advisory Group phone 03 477 5418 Dr Dave Colquhoun Michele Cray free fax 0800 bpac nz Dr Rosemary Ikram www.bpac.org.nz Dr Peter Jensen Dr Cam Kyle Dr Chris Leathart Dr Lynn McBain Associate Professor Jim Reid Dr David Reith Professor Murray Tilyard Programme Development Team Noni Allison Rachael Clarke Rebecca Didham Terry Ehau Peter Ellison Dr Malcolm Kendall-Smith Dr Anne Marie Tangney Dr Trevor Walker Dr Sharyn Willis Dave Woods Report Development Team Justine Broadley Todd Gillies Lana Johnson Web Gordon Smith Design Michael Crawford Management and Administration Kaye Baldwin Tony Fraser Kyla Letman Professor Murray Tilyard Distribution Zane Lindon Lyn Thomlinson Colleen Witchall All information is intended for use by competent health care professionals and should be utilised in conjunction with © May 2008 pertinent clinical data. Contents Key points/purpose 2 Introduction 2 Background ▪ Haematopoiesis - Cell development 3 ▪ Limitations of reference ranges for the CBC 4 ▪ Borderline abnormal results must be interpreted in clinical context 4 ▪ History and clinical examination 4 White Cells ▪ Neutrophils 5 ▪ Lymphocytes 9 ▪ Monocytes 11 ▪ Basophils 12 ▪ Eosinophils 12 ▪ Platelets 13 Haemoglobin and red cell indices ▪ Low haemoglobin 15 ▪ Microcytic anaemia 15 ▪ Normocytic anaemia 16 ▪ Macrocytic anaemia 17 ▪ High haemoglobin 17 ▪ Other red cell indices 18 Summary Table 19 Glossary 20 This resource is a consensus document, developed with haematology and general practice input. We would like to thank: Dr Liam Fernyhough, Haematologist, Canterbury Health Laboratories Dr Chris Leathart, GP, Christchurch Dr Edward Theakston, Haematologist, Diagnostic Medlab Ltd We would like to acknowledge their advice, expertise and valuable feedback on this document. -

10 11 Cyto Slides 81-85
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TESTING PROGRAM Glass Slide Critique ~ November 2010 Slide 081 Diagnosis: MDS to AML 9 WBC 51.0 x 10 /L 12 Available data: RBC 3.39 x 10 /L 72 year-old female Hemoglobin 9.6 g/dL Hematocrit 29.1 % MCV 86.0 fL Platelet count 16 x 109 /L The significant finding in this case of Acute Myelogenous Leukemia (AML) was the presence of many blast forms. The participant median for blasts, all types was 88. The blast cells in this case (Image 081) are large, irregular in shape and contain large prominent nucleoli. It is difficult to identify a blast cell as a myeloblast without the presence of an Auer rod in the cytoplasm. Auer rods were reported by three participants. Two systems are used to classify AML into subtypes, the French- American-British (FAB) and the World Health Organization (WHO). Most are familiar with the FAB classification. The WHO classification system takes into consideration prognostic factors in classifying AML. These factors include cytogenetic test results, patient’s age, white blood cell count, pre-existing blood disorders and a history of treatment with chemotherapy and/or radiation therapy for a prior cancer. The platelet count in this case was 16,000. Reduced number of platelets was correctly reported by 346 (94%) of participants. Approximately eight percent of participants commented that the red blood cells in this case were difficult to evaluate due to the presence of a bluish hue around the red blood cells. Comments received included, “On slide 081 the morphology was difficult to evaluate since there was a large amount of protein surrounding RBC’s”, “Slide 081 unable to distinguish red cell morphology due to protein” and “Unable to adequately assess morphology on slide 081 due to poor stain”. -

Advanced Blood Cell Id: Peripheral Blood Findings in Sickle Cell Anemia
ADVANCED BLOOD CELL ID: PERIPHERAL BLOOD FINDINGS IN SICKLE CELL ANEMIA Educational commentary is provided for participants enrolled in program #259- Advanced Blood Cell Identification. This virtual blood cell identification program includes case studies with more difficult challenges. To view the blood cell images in more detail, click on the sample identification numbers underlined in the paragraphs below. This will open a virtual image of the selected cell and the surrounding fields. If the image opens in the same window as the commentary, saving the commentary PDF and opening it outside your browser will allow you to switch between the commentary and the images more easily. Click on this link for the API ImageViewerTM Instructions. Learning Outcomes After completing this exercise, participants should be able to: • describe morphologic features of normal peripheral blood leukocytes. • identify morphologic characteristics distinctive of sickle cells. • distinguish selected RBC inclusions based on morphologic features. • describe significant morphologic characteristics of nucleated red blood cells. Case Study The CBC from a 30 year old African American male is as follows: WBC=9.5 x 109/L, RBC=1.66 x 1012/L, Hgb=5.0 g/dL, Hct=13.9%, MCV=83.7 fL, MCH=30.1 pg, MCHC=36.0 g/dL, RDW-CV=24.9%, MPV=9.6 fL, Platelet=326 x 109/L. Educational Commentary The cells and RBC inclusions chosen for identification in this testing event were seen in the peripheral blood of a man with a severe anemia resulting from sickle cell disease. The cell shown in ABI-08 contains a Howell-Jolly body. -

Morphologic Evaluation of Anemia – I Adewoyin S
nd M y a ed g ic lo i o n i e B Adewoyin and Ogbenna, Biol Med (Aligarh) 2016, 8:6 DOI: 10.4172/0974-8369.1000322 ISSN: 0974-8369 Biology and Medicine Review Article Open Access Morphologic Evaluation of Anemia – I Adewoyin S. Ademola1* and Ogbenna A. Abiola2 1Department of Haematology and Blood Transfusion, University of Benin Teaching Hospital, PMB 1111, Ugbowo, Benin City, Nigeria 2Department of Haematology and Blood Transfusion, Lagos University Teaching Hospital, Idi-Araba, Lagos, Nigeria *Corresponding author: Adewoyin S. Ademola, Department of Haematology and Blood Transfusion, University of Benin Teaching Hospital, PMB 1111, Ugbowo, Benin City, Nigeria, Tel: +2347033966347; E-mail: [email protected] Received date: June 20, 2016; Accepted date: July 15, 2016; Published date: July 22, 2016 Copyright: © 2016 Adewoyin AS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited. Abstract Anaemia is a feature of many tropical diseases. Anaemia diagnosis therefore remains a crucial intervention among physicians in developing countries. A barrage of laboratory test (anaemic work-up) is usually deployed in differentiating its underlying cause. However, central to anaemia evaluation is the morphology of the red cells and other cell lines. Conventionally, initial laboratory tests include full blood count, reticulocyte count and peripheral blood film (PBF). PBF is often a clinical request, performed by skilled technologist and reported by haematologist/ haematomorphologist. Findings from PBF are reviewed and reported in the light of patient’s clinical history and examination findings. -

Assessment of Splenic Function A
Assessment of splenic function A. P. N. A. Porto, A. J. J. Lammers, R. J. Bennink, I. J. M. Berge, P. Speelman, J. B. L. Hoekstra To cite this version: A. P. N. A. Porto, A. J. J. Lammers, R. J. Bennink, I. J. M. Berge, P. Speelman, et al.. Assessment of splenic function. European Journal of Clinical Microbiology and Infectious Diseases, Springer Verlag, 2010, 29 (12), pp.1465-1473. 10.1007/s10096-010-1049-1. hal-00624509 HAL Id: hal-00624509 https://hal.archives-ouvertes.fr/hal-00624509 Submitted on 19 Sep 2011 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Manuscript Click here to download Manuscript: Review Assessment of Slenic Function.doc Click here to view linked References 1 2 3 4 Title-page. 5 6 7 8 Title: Assessment of splenic function 9 10 11 Authors: A.P.N.A. de Porto1, A.J.J. Lammers1, R.J. Bennink2, I.J.M. ten Berge3, P. Speelman1, 12 4 13 J.B.L. Hoekstra . 14 15 16 Affiliations 17 18 1: Department of Infectious Diseases, Tropical Medicine and AIDS, Academic Medical Center, 19 Meibergdreef 9, 1105 AZ, Amsterdam, Netherlands. -

Containing Granules in Human Erythrocytes and Their Precursors by A
J Clin Pathol: first published as 10.1136/jcp.6.4.307 on 1 November 1953. Downloaded from J. clin. Path. (1953), 6, 307. THE INCIDENCE AND SIGNIFICANCE OF IRON- CONTAINING GRANULES IN HUMAN ERYTHROCYTES AND THEIR PRECURSORS BY A. S. DOUGLAS AND J. V. DACIE From the Department of Pathology, the Postgraduate Medical School of London (RECEIVED FOR PUBLICATION AUGUST 28, 1953) The iron in haemoglobin cannot normally be and Davis (1949) re-investigated the nature of detected in the erythrocytes of healthy human stippling in lead poisoning. They found that adults by means of a staining technique. How- many of the normoblasts in the bone marrow had ever, Gruneberg (1941a and b) used the term large basophilic granules in their cytoplasm, i.e., " siderocyte " to describe erythrocytes containing were stippled, and that a variable proportion of small granules readily demonstrable by means of the granules gave a positive reaction for iron. Perls's (Prussian blue) reaction. He found these Splenectomy of lead-poisoned guinea-pigs resulted cells in small numbers in the blood of normal rat, in a very considerable increase in the frequency of mouse, and human embryos (Gruneberg, 1941a stippled cells in the peripheral blood. and b), and later (Gruneberg, 1942) in large More recently Bilger and Tetzner (1953) have numbers in the blood of mice suffering from con- reported the presence of siderocytes in small copyright. genital anaemia. Doniach, Gruneberg, and Pear- numbers in the peripheral blood of some healthy son (1943) described the occurrence of siderocytes subjects, in newborn infants, and in various haemo- in adult human blood. -
Last Month's Slides
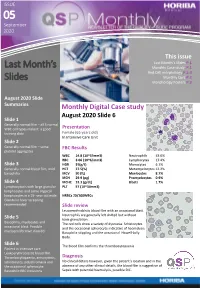
ISSUE 05ISSUE September 2020 This issue Last Month’s Slides P.1 Last Month’s Monthly Case study P.1 Red Cell morphology P.2-3 Slides Monthly Quiz P.2 Morphology Posters P.3 August 2020 Slide Summaries Monthly Digital Case study August 2020 Slide 6 Slide 1 Generally normal film – all 5 normal WBC cell types make it a good Presentation training slide Female (65 years old) In Intensive Care Unit Slide 2 Generally normal film – some FBC Results platelet aggregates WBC 14.8 (10^3/mm3) Neutrophils 53.0% RBC 3.06 (10^6/mm3) Lymphocytes 17.4% Slide 3 HGB 91(g/L) Monocytes 6.1% Generally normal blood film, mild HCT 27.5(%) Metamyelocytes 12.2% basophilia MCV 90 (fL) Myelocytes 8.7% MCH 29.9 (pg) Promyelocytes 0.9% Slide 4 MCHC 33.3 (g/dL) Blasts 1.7% Lymphocytosis with large granular PLT 57 (10^3/mm3) lymphocytes and some atypical lymphocytes in a 19- year old male. NRBCs 20/100WBCs Glandular fever screening recommended Slide review Leucoerythroblstic blood film with an occasional blast. Neutrophils are generally left shifted but without Slide 5 toxic granulation. Basophilia, myelocytes and The red cells show a variety of dyscrasia. Schistocytes occasional blast. Possible and the occasional spherocyte indicative of haemolysis. myeloproliferative disorder Basophilic stippling and the occasional Howell-Jolly Body. Slide 6 The blood film confirms the thrombocytopaenia Patient in intensive care Leukoerythroblastic blood film. Thrombocytopaenia, anisocytosis, Diagnosis schistocytes, polychromasia and No clinical details however, given the patient’s location and in the the occasional spherocyte. -

How I Manage Patients with Atypical Microcytic Anaemia
state of the art review How I manage patients with atypical microcytic anaemia Clara Camaschella Vita-Salute University and San Raffaele Scientific Institute, Milan, Italy Summary growth spurt in adolescents, in menstruating females and in pregnancy. Low dietary iron intake, malabsorption and Microcytic hypochromic anaemias are a result of defective chronic blood losses are the commonest causes of microcytic iron handling by erythroblasts that decrease the haemoglobin anaemia. Furthermore, all of the thalassaemia syndromes content per red cell. Recent advances in our knowledge of iron (alpha, beta-thalassaemia and the thalassaemic haemoglobin- metabolism and its homeostasis have led to the discovery of opathies) lead to decreased Hb per cell because of the defi- novel inherited anaemias that need to be distinguished from ciency of one of the two types of globin chains that assemble common iron deficiency or other causes of microcytosis. to form the Hb tetramer (Hb A) of adult life. Hereditary These atypical microcytic anaemias can be classified as: (i) sideroblastic anaemia, another example of microcytic red defects of intestinal iron absorption (ii) disorders of the trans- cells, is traditionally known to be result of a deficiency of ferrin receptor cycle that impair erythroblast iron uptake (iii) haem synthesis and characterized by the morphological fea- defects of mitochondrial iron utilization for haem or iron sul- ture of ringed sideroblasts, i.e. erythroblasts with mitochon- phur cluster synthesis and (iv) defects of iron recycling. A drial iron deposition visible at Perl’s staining of bone careful patient history and evaluation of laboratory tests may marrow smears. Common causes of microcytic anaemias will enable these rare conditions to be distinguished from the more not be discussed here. -

Hematology Assignment
Hematology Assignment This unit is big, and mastery of the material requires a combination of reading the book, reviewing lecture notes and especially attention to the online exercises. It covers RBC and WBC disorders, problems of coagulation and diseases of the lymph nodes. Do not wait until week before the exam to try and do the reading. All of the material in this unit will be covered on the second exam, and it’s a bunch. You’ll be sunk if you put reading and online assignments off until the just few weeks before the exam. Here’s the scoop on just the hematology unit, the immunopathology comes later. Big Robbins: chapters 13 and 14. Little Robbins: Chapter 11 Wheater: Hematopoietic Slides: For the blood smears, the entire set is online. There are no slides in your box. For the lymph nodes, there are slides in your box and online. There are four online exercises for hematology unit, two cases and two tutorials. The tutorials are rather large but absolutely necessary. Don’t flush these or try to rush through them. Online stuff: Case 11, Mr. Herbert: A man complaining of lethargy. Module 24, Coagulation tutorial Module 19, Leukemia review Case 17, Mrs. Talbot: Woman with a neck mass. Slides and TBL stuff: There are no formal TBLs for this unt. Rather the blood smear section of the slides will serve that purpose. Approach of these cases as if you will see them, their histories and lab values in case studies on the written exam. The reason is, you will. -
A Laboratory Guide to Clinical Hematology
A Laboratory Guide to Clinical Hematology A Laboratory Guide to Clinical Hematology A Laboratory Guide to Clinical Hematology VALENTIN VILLATORO AND MICHELLE TO EDMONTON A Laboratory Guide to Clinical Hematology by Michelle To is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License, except where otherwise noted. Please be aware that the content for the entirety of this eBook is subject to a creative common license: Attribution-NonCommercial 4.0 International (CC BY-NC 4.0) You are free to: Share — copy and redistribute the material in any medium or format Adapt — remix, transform, and build upon the material The licensor cannot revoke these freedoms as long as you follow the license terms. Under the following terms: Attribution — You must give appropriate credit, provide a link to the license, and indicate if changes were made. You may do so in any reasonable manner, but not in any way that suggests the licensor endorses you or your use. NonCommercial — You may not use the material for commercial purposes. No additional restrictions — You may not apply legal terms or technological measures that legally restrict others from doing anything the license permits. Contents Authors & Editors ................................................................................................................................... xii Creative Commons License and Citation ............................................................................................... xiii Contact Information and Feedback ........................................................................................................