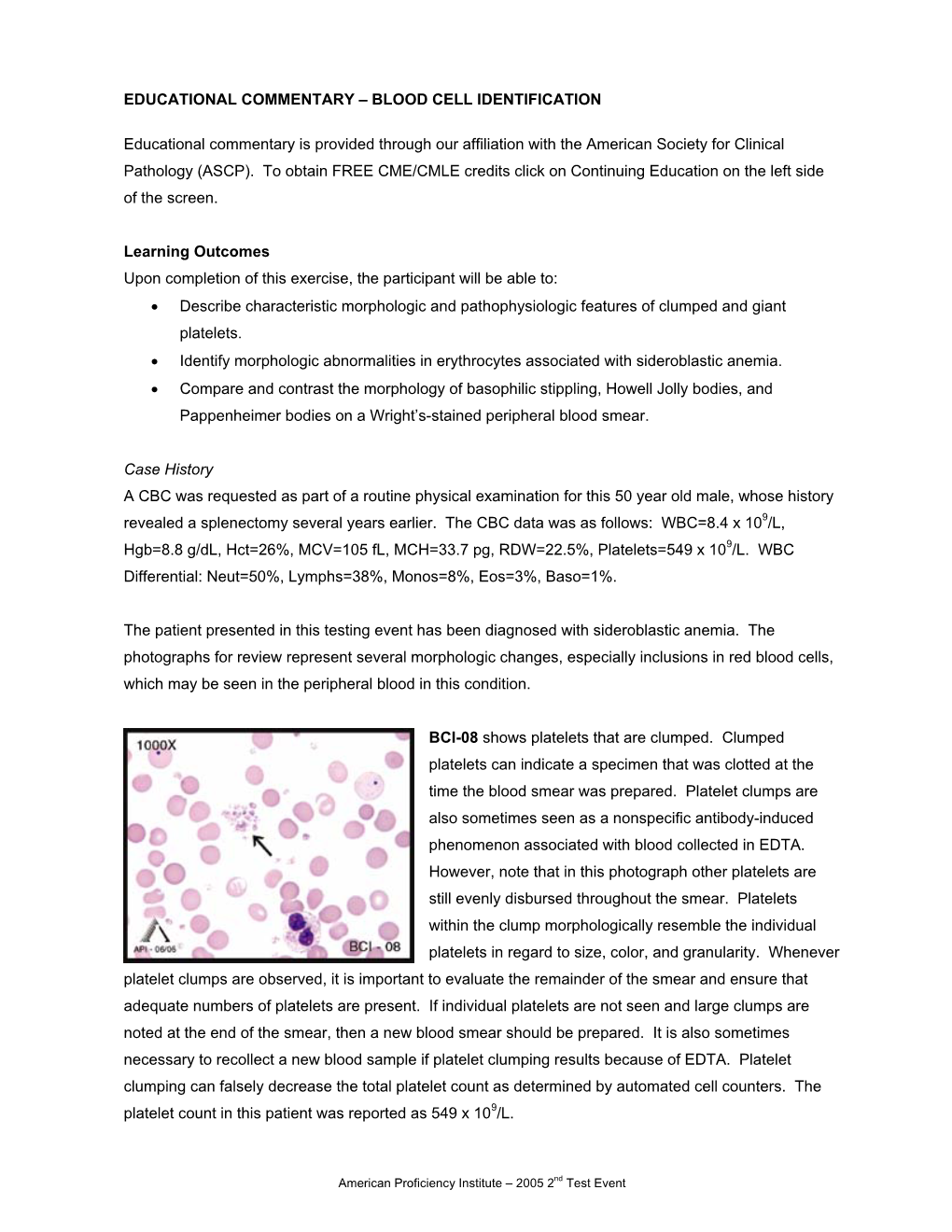
Educational Commentary – Blood Cell Identification
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Erythrocytes: Overview, Morphology, Quantity by AH Rebar Et
In: A Guide to Hematology in Dogs and Cats, Rebar A.H., MacWilliams P.S., Feldman B.F., Metzger F.L., Pollock R.V.H. and Roche J. (Eds.). Publisher: Teton NewMedia, Jackson WY (www.veterinarywire.com). Internet Publisher: International Veterinary Information Service, Ithaca NY (www.ivis.org), 8-Feb-2005; A3304.0205 Erythrocytes: Overview, Morphology, Quantity A.H. Rebar1, P.S. MacWilliams2, B.F. Feldman 3, F.L. Metzger 4, R.V.H. Pollock 5 and J. Roche 6 1Dept of Veterinary Pathobiology, School of Veterinary Medicine, Purdue University, IN,USA. 2Dept of Pathobiological Sciences, School of Veterinary Medicine, University of Wisconsin, WI, USA. 3Dept of Biomedical Sciences & Pathobiology, VA-MD - Regional College of Veterinary Medicine, Virginia Tech, VA, USA. 4Metzger Animal Hospital,State College,PA, USA. 5Fort Hill Company, Montchanin, DE, USA. 6 Hematology Systems, IDEXX Laboratories, Westbrook, ME, USA. Overview Production Red blood cells (RBC) are produced in the bone marrow. Numbers of circulating RBCs are affected by changes in plasma volume, rate of RBC destruction or loss, splenic contraction, erythropoietin (EPO) secretion, and the rate of bone marrow production. A normal PCV is maintained by an endocrine loop that involves generation and release of erythropoietin (EPO) from the kidney in response to renal hypoxia. Erythropoietin stimulates platelet production as well as red cell production. However, erythropoietin does not stimulate white blood cell (WBC) production. Erythropoiesis and RBC numbers are also affected by hormones from the adrenal cortex, thyroid, ovary, testis, and anterior pituitary. Destruction Red cells have a finite circulating lifespan. In dogs, the average normal red cell circulates approximately 100 days. -

The Hematological Complications of Alcoholism
The Hematological Complications of Alcoholism HAROLD S. BALLARD, M.D. Alcohol has numerous adverse effects on the various types of blood cells and their functions. For example, heavy alcohol consumption can cause generalized suppression of blood cell production and the production of structurally abnormal blood cell precursors that cannot mature into functional cells. Alcoholics frequently have defective red blood cells that are destroyed prematurely, possibly resulting in anemia. Alcohol also interferes with the production and function of white blood cells, especially those that defend the body against invading bacteria. Consequently, alcoholics frequently suffer from bacterial infections. Finally, alcohol adversely affects the platelets and other components of the blood-clotting system. Heavy alcohol consumption thus may increase the drinker’s risk of suffering a stroke. KEY WORDS: adverse drug effect; AODE (alcohol and other drug effects); blood function; cell growth and differentiation; erythrocytes; leukocytes; platelets; plasma proteins; bone marrow; anemia; blood coagulation; thrombocytopenia; fibrinolysis; macrophage; monocyte; stroke; bacterial disease; literature review eople who abuse alcohol1 are at both direct and indirect. The direct in the number and function of WBC’s risk for numerous alcohol-related consequences of excessive alcohol increases the drinker’s risk of serious Pmedical complications, includ- consumption include toxic effects on infection, and impaired platelet produc- ing those affecting the blood (i.e., the the bone marrow; the blood cell pre- tion and function interfere with blood cursors; and the mature red blood blood cells as well as proteins present clotting, leading to symptoms ranging in the blood plasma) and the bone cells (RBC’s), white blood cells from a simple nosebleed to bleeding in marrow, where the blood cells are (WBC’s), and platelets. -

Hematology Unit Lab 1 Review Material
Hematology Unit Lab 1 Review Material Objectives Laboratory instructors: 1. Facilitate lab discussion and answer questions Students: 1. Review the introductory material below 2. Study and review the assigned cases and questions in small groups before the Lab. This includes the pathological material using Virtual Microscopy 3. Be prepared to present your cases, questions and answers to the rest of your Lab class during the Lab Erythropoiesis: The process of red blood cell (RBC) production • Characterized by: − Increasing hemoglobin synthesis Erythroid maturation stages (Below): − Decreasing cell size - Average of 4 cell divisions during maturation − Decreasing cytoplasmic basophilia [One pronormoblast gives rise to 16 red cells] (increasing pink color) - pronormoblast → reticulocyte = 7 days − Progressive chromatin condensation of the - reticulocytes → mature RBC =1-2 days nuclei − Extrusion of nucleus (orthochromatic stage) − Extruded nuclei are subsequently phagocytized − Loss of mitotic capability after the early stage of polychromatophilic normoblast • Picture below: Erythroid progenitors (normoblasts) cluster around macrophages (arrows) in the bone marrow and spleen • Macrophages store iron • Iron is transferred from macrophages to erythroid precursor cells • Iron is used by normoblasts for hemoglobin synthesis aka nucleated rbc aka reticulocyte 1 Mature Red Blood Cell 7-8 microns; round / ovoid biconcave disc with orange-red cytoplasm, no RNA, no nucleus; survives ~120 days in circulation Classification of Anemia by Morphology 1. -

Complete Blood Count in Primary Care
Complete Blood Count in Primary Care bpac nz better medicine Editorial Team bpacnz Tony Fraser 10 George Street Professor Murray Tilyard PO Box 6032, Dunedin Clinical Advisory Group phone 03 477 5418 Dr Dave Colquhoun Michele Cray free fax 0800 bpac nz Dr Rosemary Ikram www.bpac.org.nz Dr Peter Jensen Dr Cam Kyle Dr Chris Leathart Dr Lynn McBain Associate Professor Jim Reid Dr David Reith Professor Murray Tilyard Programme Development Team Noni Allison Rachael Clarke Rebecca Didham Terry Ehau Peter Ellison Dr Malcolm Kendall-Smith Dr Anne Marie Tangney Dr Trevor Walker Dr Sharyn Willis Dave Woods Report Development Team Justine Broadley Todd Gillies Lana Johnson Web Gordon Smith Design Michael Crawford Management and Administration Kaye Baldwin Tony Fraser Kyla Letman Professor Murray Tilyard Distribution Zane Lindon Lyn Thomlinson Colleen Witchall All information is intended for use by competent health care professionals and should be utilised in conjunction with © May 2008 pertinent clinical data. Contents Key points/purpose 2 Introduction 2 Background ▪ Haematopoiesis - Cell development 3 ▪ Limitations of reference ranges for the CBC 4 ▪ Borderline abnormal results must be interpreted in clinical context 4 ▪ History and clinical examination 4 White Cells ▪ Neutrophils 5 ▪ Lymphocytes 9 ▪ Monocytes 11 ▪ Basophils 12 ▪ Eosinophils 12 ▪ Platelets 13 Haemoglobin and red cell indices ▪ Low haemoglobin 15 ▪ Microcytic anaemia 15 ▪ Normocytic anaemia 16 ▪ Macrocytic anaemia 17 ▪ High haemoglobin 17 ▪ Other red cell indices 18 Summary Table 19 Glossary 20 This resource is a consensus document, developed with haematology and general practice input. We would like to thank: Dr Liam Fernyhough, Haematologist, Canterbury Health Laboratories Dr Chris Leathart, GP, Christchurch Dr Edward Theakston, Haematologist, Diagnostic Medlab Ltd We would like to acknowledge their advice, expertise and valuable feedback on this document. -

Nucleated Red Blood Cell Count in Term and Preterm Newborns: Reference
F174 Arch Dis Child Fetal Neonatal Ed: first published as 10.1136/adc.2004.051326 on 21 February 2005. Downloaded from SHORT REPORT Nucleated red blood cell count in term and preterm newborns: reference values at birth S Perrone, P Vezzosi, M Longini, B Marzocchi, D Tanganelli, M Testa, T Santilli, G Buonocore, on behalf of the Gruppo di Studio di Ematologia Neonatale della Societa`Italiana di Neonatologia ............................................................................................................................... Arch Dis Child Fetal Neonatal Ed 2005;90:F174–F175. doi: 10.1136/adc.2004.051326 discrepancy, neonatal Dubowitz evaluation was used. All The prognostic value of nucleated red blood cell count at babies with congenital malformation, haematopoietic birth in relation to neonatal outcome has been established. anomalies, Rh and/or ABO incompatibility, inborn error of However, reference values were needed to usefully interpret metabolism, sepsis, a mother with diabetes, multiple gesta- this variable. The normal range of reference values for tion, smoking, drug abuse, anaemia, placenta previa, abrup- absolute nucleated red blood cell count in 695 preterm and tion, or infarcts were excluded from the study to eliminate term newborns is reported. risks that could affect the number of circulating NRBCs. We also prospectively collected specific neonatal data: Apgar score at five minutes, birth weight, cord pH. After excluding neonates documented to have a five minute Apgar ucleated red blood cells (NRBCs) are immature score ,6, cord pH,7.2, birth weight more than 2 SDs below erythrocytes, commonly found in the peripheral blood the mean, according to the growth chart of Yudkin et al,5 we of newborns at birth. -

Red Blood Cell Morphology in Patients with Β-Thalassemia Minor
J Lab Med 2017; 41(1): 49–52 Short Communication Carolin Körber, Albert Wölfler, Manfred Neubauer and Christoph Robier* Red blood cell morphology in patients with β-thalassemia minor DOI 10.1515/labmed-2016-0052 Keywords: β-thalassemia minor; erythrocytes; red blood Received July 11, 2016; accepted October 20, 2016; previously published cells; red blood cell morphology. online December 10, 2016 Abstract In β-thalassemias, the examination of a peripheral blood (PB) smear may provide relevant clues to initial diagnosis. Background: A systematic analysis of the occurrence of Complete laboratory investigation consists of the determina- red blood cell (RBC) abnormalities in β-thalassemia minor tion of the complete blood count, assessment of red blood has not been performed to date. This study aimed to iden- cell (RBC) morphology, high performance liquid chroma- tify and quantify the frequency of RBC abnormalities in tography (HPLC), hemoglobin electrophoresis and, where patients with β-thalassemia minor. necessary, DNA analysis [1]. Especially in the clinically Methods: We examined blood smears of 33 patients with severe forms referred to as β-thalassemia major and interme- β-thalassemia minor by light microscopy for the occur- dia, RBC abnormalities are often markedly apparent [2]. In rence of 15 defined RBC abnormalities. In the case of posi- β-thalassemia minor, also called β-thalassemia trait, the car- tivity, the abnormal cells/20 high power fields (HPF) at riers are usually clinically asymptomatic, showing persistent 1000-fold magnification were counted. microcytosis and hypochromia or mild microcytic anemia [1, Results: Anisocytosis, poikilocytosis and target cells 3]. The PB smear may show microcytosis, hypochromia and, (median 42/20 HPF) were observed in all, and ovalocytes infrequently, poikilocytosis [2]. -

Laboratory Diagnosis Review
Laboratory Diagnosis Review Hematology Definition: The study of the three cellular elements of blood: Red Blood Cells (RBCs), White Blood Cells (WBCs), and Platelets Hemoglobin (Hgb or Hb): The oxygen carrying compound in RBCs Reference Range: Men 14-18 g/dL, Women 12-16 g/dL, Boy and girl levels are equal till age 11 Smoking increases, Pregnancy decreases, Capillary levels in newborns are higher than venous levels, Race, Position, and Time of day have minor effects, High WBCs may falsely raise Hgb. Below normal Hgb = anemia Red Blood Cell Count Reference Range: Men 4l5-6 million / cubic ml, Women4.0-5.5 million / ml3. Hematocrit (Hct): The ratio of RBCs to plasma Reference Range, Men 40%-54%, Women 37%-47%, Depends mostly on the number of RBCs but is slightly effected by the average RBC size, Not measured directly, but is calculated from the RBC count and the mean corpuscular volume (MCV). Increased by smoking, Decrease = anemia Useful Relationships: Hb X 3 = Hct RBCs (millions) X 3 = Hgb RBCs (millions) X 9 = Hct Wintrobe Indices: These indices are only significant if the RBCs, Hgb, and/or Hct. is abnormal MCV: Mean Corpuscular Volume MCH: Mean Corpuscular Hemoglobin MCHC: Mean Corpuscular Hemoglobin Concentration RDW: Red blood cell Distribution Width MCV: Reference Ranges: Men 80-95 fl (femtoliters), Women 81-99 fl (femto = 1 quadrillionth) Increased MCV = Macrocytosis, Decreased = Microcytosis MCV is increased by smoking, by B12 and/or folic acid deficiency, chronic liver disease, chronic alcoholism, Cardiorespiratory problems… Some macrocytic patients will not have macrocytosis MCV is decreased by iron deficiency, thalassemia, and anemia of chronic disease MCH: Reference Range 27-31 pg MCH is increased by Macrocytic anemias. -

Unique Monoclonal Antibodies Specifically Bind Surface
EXPERIMENTAL CELL RESEARCH 319 (2013) 2700– 2707 Available online at www.sciencedirect.com journal homepage: www.elsevier.com/locate/yexcr Research Article Unique monoclonal antibodies specifically bind surface structures on human fetal erythroid blood cells Silke Zimmermanna,n,1, Christiane Hollmannb,1, Stefan A. Stachelhausc,1 aHannover Clinical Trial Center GmbH, Carl-Neuberg-Strasse. 1/k27, 30625 Hannover, Germany bGlaxoSmithKline GmbH & Co. KG, Prinzregentenplatz 9, 81675, Munich, Germany cHuman Gesellschaft für Biochemica und Diagnostica mbH, Stegelitzer Str. 3, 39126 Magdeberg, Germany article information abstract Article Chronology: Background: Continuing efforts in development of non-invasive prenatal genetic tests have Received 6 March 2013 focused on the isolation of fetal nucleated red blood cells (NRBCs) from maternal blood for Received in revised form decades. Because no fetal cell-specific antibody has been described so far, the present study 22 June 2013 focused on the development of monoclonal antibodies (mAbs) to antigens that are expressed Accepted 24 June 2013 exclusively on fetal NRBCs. Available online 29 June 2013 Methods: Mice were immunized with fetal erythroid cell membranes and hybridomas screened for Abs using a multi-parameter fluorescence-activated cell sorting (FACS). Selected mAbs were Keywords: evaluated by comparative FACS analysis involving Abs known to bind erythroid cell surface Monoclonal antibody markers (CD71, CD36, CD34), antigen-i, galactose, or glycophorin-A (GPA). Specificity was further Immunophenotyping confirmed by extensive immunohistological and immunocytological analyses of NRBCs from Fetal nucleated red blood cells umbilical cord blood and fetal and adult cells from liver, bone marrow, peripheral blood, and Prenatal diagnostics lymphoid tissues. Results: Screening of 690 hybridomas yielded three clones of which Abs from 4B8 and 4B9 clones demonstrated the desired specificity for a novel antigenic structure expressed on fetal erythroblast cell membranes. -

Diagnostic Efficacy of Nucleated Red Blood Cell Count in the Early Diagnosis of Neonatal Sepsis
Original Research Diagnostic efficacy of Nucleated Red blood cell count in the early diagnosis of neonatal sepsis Abhishek M G1,*, Sanjay M2 1Associate Professor, 2Assistant Professor, Department of Pathology, Adichunchanagiri Institute of Medical Sciences, B.G. Nagara, Mandya district, Karnataka state, India 571448 *Corresponding Author: E-mail: [email protected] ABSTRACT: Objective: To determine the efficacy of Nucleated Red blood cell count in the Early diagnosis of neonatal sepsis. Material and Methods: Cross sectional diagnostic study conducted over a period of 1 year from Oct 2013 to Sept 2014, which included 60 neonates with clinical suspicious of sepsis at birth and within 72 hours or had maternal history of infection. The cord blood was collected immediately after delivery for NRBCs count under peripheral smear. Statistical analysis was performed and Sensitivity, specificity, positive predictive value and negative predictive value was calculated. Result: NRBCs count was higher in all sepsis cases. Sensitivity of NRBc for detecting proven sepsis was 35%, its specificity 53.48%, its positive predictive value was 23.07% and its negative predictive value was 67.64%. Conclusion: It is a simple and cost effective test in early diagnosis of early neonatal sepsis. It will help the clinicians in early diagnosis and treatment whenever applicable, thereby reducing the neonatal morbidity and mortality. Keywords: Nucleated red blood cells, Early onset neonatal sepsis, Blood culture, Hematological parameters. INTRODUCTION The present study aims to determine the Neonatal sepsis, characterized by systemic efficacy of Nucleated Red blood cell count in the response to bacterial infection, is the leading cause of diagnosis of neonatal sepsis in a rural setup. -

10 11 Cyto Slides 81-85
NEW YORK STATE CYTOHEMATOLOGY PROFICIENCY TESTING PROGRAM Glass Slide Critique ~ November 2010 Slide 081 Diagnosis: MDS to AML 9 WBC 51.0 x 10 /L 12 Available data: RBC 3.39 x 10 /L 72 year-old female Hemoglobin 9.6 g/dL Hematocrit 29.1 % MCV 86.0 fL Platelet count 16 x 109 /L The significant finding in this case of Acute Myelogenous Leukemia (AML) was the presence of many blast forms. The participant median for blasts, all types was 88. The blast cells in this case (Image 081) are large, irregular in shape and contain large prominent nucleoli. It is difficult to identify a blast cell as a myeloblast without the presence of an Auer rod in the cytoplasm. Auer rods were reported by three participants. Two systems are used to classify AML into subtypes, the French- American-British (FAB) and the World Health Organization (WHO). Most are familiar with the FAB classification. The WHO classification system takes into consideration prognostic factors in classifying AML. These factors include cytogenetic test results, patient’s age, white blood cell count, pre-existing blood disorders and a history of treatment with chemotherapy and/or radiation therapy for a prior cancer. The platelet count in this case was 16,000. Reduced number of platelets was correctly reported by 346 (94%) of participants. Approximately eight percent of participants commented that the red blood cells in this case were difficult to evaluate due to the presence of a bluish hue around the red blood cells. Comments received included, “On slide 081 the morphology was difficult to evaluate since there was a large amount of protein surrounding RBC’s”, “Slide 081 unable to distinguish red cell morphology due to protein” and “Unable to adequately assess morphology on slide 081 due to poor stain”. -

Advanced Blood Cell Id: Peripheral Blood Findings in Sickle Cell Anemia
ADVANCED BLOOD CELL ID: PERIPHERAL BLOOD FINDINGS IN SICKLE CELL ANEMIA Educational commentary is provided for participants enrolled in program #259- Advanced Blood Cell Identification. This virtual blood cell identification program includes case studies with more difficult challenges. To view the blood cell images in more detail, click on the sample identification numbers underlined in the paragraphs below. This will open a virtual image of the selected cell and the surrounding fields. If the image opens in the same window as the commentary, saving the commentary PDF and opening it outside your browser will allow you to switch between the commentary and the images more easily. Click on this link for the API ImageViewerTM Instructions. Learning Outcomes After completing this exercise, participants should be able to: • describe morphologic features of normal peripheral blood leukocytes. • identify morphologic characteristics distinctive of sickle cells. • distinguish selected RBC inclusions based on morphologic features. • describe significant morphologic characteristics of nucleated red blood cells. Case Study The CBC from a 30 year old African American male is as follows: WBC=9.5 x 109/L, RBC=1.66 x 1012/L, Hgb=5.0 g/dL, Hct=13.9%, MCV=83.7 fL, MCH=30.1 pg, MCHC=36.0 g/dL, RDW-CV=24.9%, MPV=9.6 fL, Platelet=326 x 109/L. Educational Commentary The cells and RBC inclusions chosen for identification in this testing event were seen in the peripheral blood of a man with a severe anemia resulting from sickle cell disease. The cell shown in ABI-08 contains a Howell-Jolly body. -

Research Article
z Available online at http://www.journalcra.com INTERNATIONAL JOURNAL OF CURRENT RESEARCH International Journal of Current Research Vol. 9, Issue, 12, pp.62497-62502, December, 2017 ISSN: 0975-833X RESEARCH ARTICLE INCLUSION BODIES - A REVIEW 1Dr. Mrunalini Mahesh Dadpe, 2, *Dr. Sourab Kumar, 3Dr. Mahesh Dadpe, 4Dr. Payoshnee Bhalinge Jadhav, 5Dr. Abhishek Jadhav and 6Dr. Shilpi Suman 1, 4Department of Oral Pathology, M A Rangoonwala Dental College, Aazam Campus, Camp, Pune 411001, India 2, 5, 6Department of oral Pathology, D.Y. Patil School of Dentistry, Nerul, Navi Mumbai 400706, India 3MIDSR Dental College, Vishwanathpuram, Amba Jogai Road, Latur 413531, India ARTICLE INFO ABSTRACT Article History: The word inclusion means incorporation. Inclusion bodies are nuclear or cytoplasmic aggregates of Received 16th September, 2017 stainable substances which are usually ‘proteins’. They typically represent sites of viral multiplication Received in revised form in bacteria or in a eukaryotic cell and usually consist of viral capsid proteins. Inclusion bodies are 17th October, 2017 typically identified within a cell by their different appearance. Accepted 25th November, 2017 Published online 27th December, 2017 Key words: Proteins, Viral, Types, Structures Copyright © 2017, Mrunalini Mahesh Dadpe et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Citation: Dr. Mrunalini Mahesh Dadpe, Dr. Sourab Kumar, Dr. Mahesh Dadpe, Dr. Payoshnee Bhalinge Jadhav, Dr. Abhishek Jadhav and Dr. Shilpi Suman, 2017. “Inclusion Bodies - A Review”, International Journal of Current Research, 9, (12), 62497-62502. Classification INTRODUCTION Viral inclusion bodies Inclusion bodies (IB) can also be hallmarks of genetic diseases, as in the case of Neuronal Inclusion bodies in neural disorders, A.