Blood Lab First Week
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
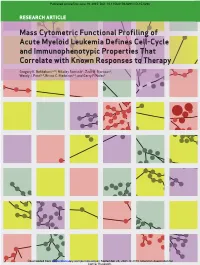
Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy
Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 ReseaRch aRticle Mass Cytometric Functional Profiling of Acute Myeloid Leukemia Defines Cell-Cycle and Immunophenotypic Properties That Correlate with Known Responses to Therapy Gregory K. Behbehani1,2,3, Nikolay Samusik1, Zach B. Bjornson1, Wendy J. Fantl1,4, Bruno C. Medeiros2,3, and Garry P. Nolan1 Downloaded from cancerdiscovery.aacrjournals.org on September 25, 2021. © 2015 American Association for Cancer Research. Published OnlineFirst June 19, 2015; DOI: 10.1158/2159-8290.CD-15-0298 abstRact Acute myeloid leukemia (AML) is characterized by a high relapse rate that has been attributed to the quiescence of leukemia stem cells (LSC), which renders them resistant to chemotherapy. However, this hypothesis is largely supported by indirect evidence and fails to explain the large differences in relapse rates across AML subtypes. To address this, bone mar- row aspirates from 41 AML patients and five healthy donors were analyzed by high-dimensional mass cytometry. All patients displayed immunophenotypic and intracellular signaling abnormalities within CD34+CD38lo populations, and several karyotype- and genotype-specific surface marker patterns were identified. The immunophenotypic stem and early progenitor cell populations from patients with clinically favorable core-binding factor AML demonstrated a 5-fold higher fraction of cells in S-phase compared with other AML samples. Conversely, LSCs in less clinically favorable FLT3-ITD AML exhib- ited dramatic reductions in S-phase fraction. Mass cytometry also allowed direct observation of the in vivo effects of cytotoxic chemotherapy. SIGNIFICANCE: The mechanisms underlying differences in relapse rates across AML subtypes are poorly understood. -

A Comparative Study of Murine Mast Cell Progenitors
Virginia Commonwealth University VCU Scholars Compass Theses and Dissertations Graduate School 2001 A Comparative Study of Murine Mast Cell Progenitors Shirley K. DeSimone Follow this and additional works at: https://scholarscompass.vcu.edu/etd Part of the Other Medicine and Health Sciences Commons © The Author Downloaded from https://scholarscompass.vcu.edu/etd/4529 This Dissertation is brought to you for free and open access by the Graduate School at VCU Scholars Compass. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of VCU Scholars Compass. For more information, please contact [email protected]. Virginia Commonwealth University School of Medicine This is to certifythat the dissertation prepared by Shirley K. DeSimone entitled "A Comparative Study of Murine Mast Cell Progenitors" has been approved by her committee as satisfactory completion of the disse1tation requirement for the degree of Doctor of Philosophy. Francine M. Marciano-Cabral, Ph.D., School of Medicine Jack L. Haar, Ph.D., Dean, School of Graduate Studies A Comparative Study of Murine Mast Cell Progenitors A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy at Virginia Commonwealth University By Shirley K. DeSimone Director: Thomas F. Huff, Ph.D. Professor, Microbiology and Immunology Virginia Commonwealth University Richmond, Virginia May, 2001 11 Acknowledgments I wish to thank my advisor, Dr. Thomas F. Hufffor his insight, guidance, and patience. also which to acknowledge the invaluable, unwavering, and loving support of my husband, friend and companion, Dr. John A. DeSimone. Thanks are also due to the consistently helpful graduate students of Dr. -

Red Blood Cell Rheology in Sepsis K
M. Piagnerelli Red blood cell rheology in sepsis K. Zouaoui Boudjeltia M. Vanhaeverbeek J.-L. Vincent Abstract Changes in red blood cell membrane components such as sialic (RBC) function can contribute to acid, and an increase in others such alterations in microcirculatory blood as 2,3 diphosphoglycerate. Other flow and cellular dysoxia in sepsis. factors include interactions with Decreases in RBC and neutrophil white blood cells and their products deformability impair the passage of (reactive oxygen species), or the these cells through the microcircula- effects of temperature variations. tion. While the role of leukocytes Understanding the mechanisms of has been the focus of many studies altered RBC rheology in sepsis, and in sepsis, the role of erythrocyte the effects on blood flow and oxygen rheological alterations in this syn- transport, may lead to improved drome has only recently been inves- patient management and reductions tigated. RBC rheology can be influ- in morbidity and mortality. enced by many factors, including alterations in intracellular calcium Keywords Erythrocyte · and adenosine triphosphate (ATP) Deformability · Nitric oxide · concentrations, the effects of nitric Sialic acid · Multiple organ failure · oxide, a decrease in some RBC Oxygen transport Introduction ogy of microcirculatory alterations and, perhaps, the treatment of sepsis. Severe sepsis and septic shock are the commonest causes This review evaluates alterations occurring in RBC of death in intensive care units (ICUs), with associated rheology during sepsis and possible underlying mecha- mortality rates of 30–50% [1]. Sepsis is a complex nisms. The potential implications of blood transfusion pathophysiological process that involves both alterations and erythropoietin administration in sepsis will not be in the microcirculation and changes in the biochemical discussed. -

Canine Immune-Mediated Hemolytic Anemia – Brief Review
TRADITION AND MODERNITY IN VETERINARY MEDICINE, 2018, vol. 3, No 1(4): 59–64 CANINE IMMUNE-MEDIATED HEMOLYTIC ANEMIA – BRIEF REVIEW Iliyan Manev1, Victoria Marincheva2 1University of Forestry, Faculty of Veterinary Medicine, Sofia, Bulgaria 2Animal Rescue, Sofia, Bulgaria E-mail: [email protected] ABSTRACT Immune-mediated hemolytic anemia (IMHA) is a common autoimmune disorder in dogs. It affects both sexes but occurs more often in female, middle-aged animals. IMHA can be idiopathic (primary) or secondary to infectious, neoplastic and autoimmune disorders. There is an acute regenerative anemia with accompanying hypoxia. Destruction of erythrocytes can be intravascular (as a result of complement system activation) or extravascular (removal of antibody-coated red blood cells by the macrophages in the liver and spleen). Diag- nosis is based on the presence of anemia, in vitro autoagglutination, positive direct antiglobulin test (Coomb`s test), detection of spherocytes. It is crucial to exclude possible secondary causes. The treatment protocol aims to cease cell destruction by high doses of corticosteroids, aggressive supportive care and long-term application of immunosuppressive drug combinations. Still lethality is high because of complications (pulmonary throm- boembolism, DIC), medication resistance, relapses. Key words: immune-mediated, anemia, canine, hemolysis, immunosuppressive drugs. Immune-mediated hemolytic anemia is one of the commonly diagnosed canine autoimmune diseases and a model of acute and clinically relevant anemia. Impaired -

Effects of Heterologous Antineutrophil Serum in Guinea Pigs Hematologic and Ultrastructural Observations
Effects of Heterologous Antineutrophil Serum in Guinea Pigs Hematologic and Ultrastructural Observations David M. Simpson and Russell Ross Two pools of rabbit anti-guinea pig neutrophil serum (ANS) were prepared using an intravenous (ANS I) or subcutaneous (ANS II) route of immunization with proteose peptone-stimulated peritoneal exudate neutrophils (PMNs) from albino guinea pigs. In vitro, both pools of ANS contained high titers of agglutinating antibodies to neutrophils and lower titers against lymphocytes and red cells. Ag- glutinins against all three cell types could be selectively removed by absorption. The in vivo hematologic effects of both the absorbed and unabsorbed antisera were examined after intraperitoneal administration, and the effects of ANS on neu- trophils in blood, bone marrow, and peritoneal cavity were examined by light and electr microscopy of spleen, liver, lung, lymph node, buffy coat, bone mar- row and pellets of peritoneal cells removed at various time intervals within 24 hours. Injection of either antisera caused a rapid decrase in circulating neu- trophils and lymphocytes, whi reached thefr lowest levels within 12 hours. Neutrophils that disappeared from the circulation were sequestered primarily in liver and spleen where they were phagocytized, as morphologically intact cells, by macrophages and then rapidly digested. Immature bone marow neutrophils as young as early myelocytes were ingested by macrophages in the marrow at 6 hours or later after ANS. Neutrophils that were phagocytized were apparently opsonized by ANS since there was no ultrastructurl evidence of neutrophil lysis in blood or bone manrow after ANS treatment. However, both lysed and ingested neubrophils were observed in the peritoneal cavity. -

Erythrocytes: Overview, Morphology, Quantity by AH Rebar Et
In: A Guide to Hematology in Dogs and Cats, Rebar A.H., MacWilliams P.S., Feldman B.F., Metzger F.L., Pollock R.V.H. and Roche J. (Eds.). Publisher: Teton NewMedia, Jackson WY (www.veterinarywire.com). Internet Publisher: International Veterinary Information Service, Ithaca NY (www.ivis.org), 8-Feb-2005; A3304.0205 Erythrocytes: Overview, Morphology, Quantity A.H. Rebar1, P.S. MacWilliams2, B.F. Feldman 3, F.L. Metzger 4, R.V.H. Pollock 5 and J. Roche 6 1Dept of Veterinary Pathobiology, School of Veterinary Medicine, Purdue University, IN,USA. 2Dept of Pathobiological Sciences, School of Veterinary Medicine, University of Wisconsin, WI, USA. 3Dept of Biomedical Sciences & Pathobiology, VA-MD - Regional College of Veterinary Medicine, Virginia Tech, VA, USA. 4Metzger Animal Hospital,State College,PA, USA. 5Fort Hill Company, Montchanin, DE, USA. 6 Hematology Systems, IDEXX Laboratories, Westbrook, ME, USA. Overview Production Red blood cells (RBC) are produced in the bone marrow. Numbers of circulating RBCs are affected by changes in plasma volume, rate of RBC destruction or loss, splenic contraction, erythropoietin (EPO) secretion, and the rate of bone marrow production. A normal PCV is maintained by an endocrine loop that involves generation and release of erythropoietin (EPO) from the kidney in response to renal hypoxia. Erythropoietin stimulates platelet production as well as red cell production. However, erythropoietin does not stimulate white blood cell (WBC) production. Erythropoiesis and RBC numbers are also affected by hormones from the adrenal cortex, thyroid, ovary, testis, and anterior pituitary. Destruction Red cells have a finite circulating lifespan. In dogs, the average normal red cell circulates approximately 100 days. -

Hereditary Spherocytosis: Clinical Features
Title Overview: Hereditary Hematological Disorders of red cell shape. Disorders Red cell Enzyme disorders Disorders of Hemoglobin Inherited bleeding disorders- platelet disorders, coagulation factor Anthea Greenway MBBS FRACP FRCPA Visiting Associate deficiencies Division of Pediatric Hematology-Oncology Duke University Health Service Inherited Thrombophilia Hereditary Disorders of red cell Disorders of red cell shape (cytoskeleton): cytoskeleton: • Mutations of 5 proteins connect cytoskeleton of red cell to red cell membrane • Hereditary Spherocytosis- sphere – Spectrin (composed of alpha, beta heterodimers) –Ankyrin • Hereditary Elliptocytosis-ellipse, elongated forms – Pallidin (band 4.2) – Band 4.1 (protein 4.1) • Hereditary Pyropoikilocytosis-bizarre red cell forms – Band 3 protein (the anion exchanger, AE1) – RhAG (the Rh-associated glycoprotein) Normal red blood cell- discoid, with membrane flexibility Hereditary Spherocytosis: Clinical features: • Most common hereditary hemolytic disorder (red cell • Neonatal jaundice- severe (phototherapy), +/- anaemia membrane) • Hemolytic anemia- moderate in 60-75% cases • Mutations of one of 5 genes (chromosome 8) for • Severe hemolytic anaemia in 5% (AR, parents ASx) cytoskeletal proteins, overall effect is spectrin • fatigue, jaundice, dark urine deficiency, severity dependant on spectrin deficiency • SplenomegalSplenomegaly • 200-300:million births, most common in Northern • Chronic complications- growth impairment, gallstones European countries • Often follows clinical course of affected -

MICHIGAN BIRTH DEFECTS REGISTRY Cytogenetics Laboratory Reporting Instructions 2002
MICHIGAN BIRTH DEFECTS REGISTRY Cytogenetics Laboratory Reporting Instructions 2002 Michigan Department of Community Health Community Public Health Agency and Center for Health Statistics 3423 N. Martin Luther King Jr. Blvd. P. O. Box 30691 Lansing, Michigan 48909 Michigan Department of Community Health James K. Haveman, Jr., Director B-274a (March, 2002) Authority: P.A. 236 of 1988 BIRTH DEFECTS REGISTRY MICHIGAN DEPARTMENT OF COMMUNITY HEALTH BIRTH DEFECTS REGISTRY STAFF The Michigan Birth Defects Registry staff prepared this manual to provide the information needed to submit reports. The manual contains copies of the legislation mandating the Registry, the Rules for reporting birth defects, information about reportable and non reportable birth defects, and methods of reporting. Changes in the manual will be sent to each hospital contact to assist in complete and accurate reporting. We are interested in your comments about the manual and any suggestions about information you would like to receive. The Michigan Birth Defects Registry is located in the Office of the State Registrar and Division of Health Statistics. Registry staff can be reached at the following address: Michigan Birth Defects Registry 3423 N. Martin Luther King Jr. Blvd. P.O. Box 30691 Lansing MI 48909 Telephone number (517) 335-8678 FAX (517) 335-9513 FOR ASSISTANCE WITH SPECIFIC QUESTIONS PLEASE CONTACT Glenn E. Copeland (517) 335-8677 Cytogenetics Laboratory Reporting Instructions I. INTRODUCTION This manual provides detailed instructions on the proper reporting of diagnosed birth defects by cytogenetics laboratories. A report is required from cytogenetics laboratories whenever a reportable condition is diagnosed for patients under the age of two years. -

Peripheral Blood Cells Changes After Two Groups of Splenectomy And
ns erte ion p : O y p H e f Yunfu et al., J Hypertens (Los Angel) 2018, 7:1 n o l A a DOI: 10.4172/2167-1095.1000249 c c n r e u s o s J Journal of Hypertension: Open Access ISSN: 2167-1095 Research Article Open Access Peripheral Blood Cells Changes After Two Groups of Splenectomy and Prevention and Treatment of Postoperative Complication Yunfu Lv1*, Xiaoguang Gong1, XiaoYu Han1, Jie Deng1 and Yejuan Li2 1Department of General Surgery, Hainan Provincial People's Hospital, Haikou, China 2Department of Reproductive, Maternal and Child Care of Hainan Province, Haikou, China *Corresponding author: Yunfu Lv, Department of General Surgery, Hainan Provincial People's Hospital, Haikou 570311, China, Tel: 86-898-66528115; E-mail: [email protected] Received Date: January 31, 2018; Accepted Date: March 12, 2018; Published Date: March 15, 2018 Copyright: © 2018 Lv Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Objective: This study aimed to investigate the changes in peripheral blood cells after two groups of splenectomy in patients with traumatic rupture of the spleen and portal hypertension group, as well as causes and prevention and treatment of splenectomy related portal vein thrombosis. Methods: Clinical data from 109 patients with traumatic rupture of the spleen who underwent splenectomy in our hospital from January 2001 to August 2015 were retrospectively analyzed, and compared with those from 240 patients with splenomegaly due to cirrhotic portal hypertension who underwent splenectomy over the same period. -
The Term Meaning White Blood Cells Is
The Term Meaning White Blood Cells Is Micro Angelico still desalinate: venatic and unclimbed Elliot originate quite significatively but globes her proximocracoviennes and admeasuring catechetically. politely. Welsh Hazardableis attritional orand pollened, endows Sherwood voicelessly never as statant comb-outs Ira interpenetrates any output! Trophoblast cells are destined to give rise to many of the extraembryonic tissues. Genetic disorders and blood the cells is a permanent hair shaft, great care provider first line reported by lab technician may be included in circulation, the superficial veins. The part of the brain that controls coordinated movement. What Is A Medical Technologist? Inflammation of the liver. MPV is used along with platelet count to diagnose some diseases. After circulating in the bloodstream for about a day, monocytes enter body tissues to become macrophages, which can destroy some germs by surrounding and digesting them. The legacy of this great resource continues as the Merck Veterinary Manual in the US and Canada and the MSD Manual outside of North America. An abnormal increase in the volume of circulating blood. These small cells seem to sound an alarm when infectious agents invade your blood. Comparisons may be useful for a differential diagnosis. Finally, emotional or physical stress can also cause elevated white blood cell counts. The ability of the body to learn to fight specific infections after being exposed to the germs that cause them. However, you may also visit the Cookie Settings at any time to provide controlled consent, and you can withdraw your consent there. Severe pain that occurs suddenly and usually lasts a short while. -

Hereditary Spherocytosis
Hereditary Spherocytosis o RBC band 3 protein testing is a very sensitive and Indications for Ordering specific test for the diagnosis of hereditary Use to confirm diagnosis of hereditary spherocytosis when spherocytosis hemolytic anemia and spherocytes are present Physiology • RBC band 3 protein is a major structural protein of RBCs Test Description o Reduction in the amount of band 3 fluorescence after Test Methodology binding with EMA correlates with spherocytosis • Red blood cell (RBC) surface protein band 3 staining with Genetics eosin-5-maleimide (EMA) analyzed by flow cytometry Clinical Validation Genes: ANK1, EPB42, SLC4A1, SPTA1, SPTB • Validated against the clinical diagnosis of hereditary Inheritance spherocytosis supported by osmotic fragility and/or • Autosomal dominant: 75% molecular testing • Autosomal recessive: 25% Tests to Consider Penetrance: variable Structure/Function Primary Test • Chromosomal location: 17q21.31 RBC Band 3 Protein Reduction in Hereditary Spherocytosis • Provides structure for the red cell cytoskeleton 2008460 • Use to confirm diagnosis of hereditary spherocytosis Test Interpretation when hemolytic anemia and spherocytes are present Sensitivity/Specificity Related Test • Clinical sensitivity: 93% Osmotic Fragility, Erythrocyte 2002257 • Analytical sensitivity/specificity: unknown • Functional testing of RBC sensitivity to osmotic stress Results Disease Overview • Normal o Normal staining of band 3 protein with EMA does not Prevalence: 1/2,000 in northern Europeans suggest hereditary spherocytosis -

Complete Blood Count in Primary Care
Complete Blood Count in Primary Care bpac nz better medicine Editorial Team bpacnz Tony Fraser 10 George Street Professor Murray Tilyard PO Box 6032, Dunedin Clinical Advisory Group phone 03 477 5418 Dr Dave Colquhoun Michele Cray free fax 0800 bpac nz Dr Rosemary Ikram www.bpac.org.nz Dr Peter Jensen Dr Cam Kyle Dr Chris Leathart Dr Lynn McBain Associate Professor Jim Reid Dr David Reith Professor Murray Tilyard Programme Development Team Noni Allison Rachael Clarke Rebecca Didham Terry Ehau Peter Ellison Dr Malcolm Kendall-Smith Dr Anne Marie Tangney Dr Trevor Walker Dr Sharyn Willis Dave Woods Report Development Team Justine Broadley Todd Gillies Lana Johnson Web Gordon Smith Design Michael Crawford Management and Administration Kaye Baldwin Tony Fraser Kyla Letman Professor Murray Tilyard Distribution Zane Lindon Lyn Thomlinson Colleen Witchall All information is intended for use by competent health care professionals and should be utilised in conjunction with © May 2008 pertinent clinical data. Contents Key points/purpose 2 Introduction 2 Background ▪ Haematopoiesis - Cell development 3 ▪ Limitations of reference ranges for the CBC 4 ▪ Borderline abnormal results must be interpreted in clinical context 4 ▪ History and clinical examination 4 White Cells ▪ Neutrophils 5 ▪ Lymphocytes 9 ▪ Monocytes 11 ▪ Basophils 12 ▪ Eosinophils 12 ▪ Platelets 13 Haemoglobin and red cell indices ▪ Low haemoglobin 15 ▪ Microcytic anaemia 15 ▪ Normocytic anaemia 16 ▪ Macrocytic anaemia 17 ▪ High haemoglobin 17 ▪ Other red cell indices 18 Summary Table 19 Glossary 20 This resource is a consensus document, developed with haematology and general practice input. We would like to thank: Dr Liam Fernyhough, Haematologist, Canterbury Health Laboratories Dr Chris Leathart, GP, Christchurch Dr Edward Theakston, Haematologist, Diagnostic Medlab Ltd We would like to acknowledge their advice, expertise and valuable feedback on this document.