Assistive Mobility Devices Focusing on Smart Walkers: Classification and Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Tips for Communicating with People with Disabilities
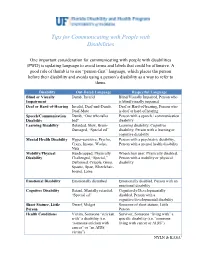
Tips for Communicating with People with Disabilities One important consideration for communicating with people with disabilities (PWD) is updating language to avoid terms and labels that could be offensive. A good rule of thumb is to use “person-first” language, which places the person before their disability and avoids using a person’s disability as a way to refer to them. Disability Out-Dated Language Respectful Language Blind or Visually Dumb, Invalid Blind/Visually Impaired, Person who Impairment is blind/visually impaired Deaf or Hard-of-Hearing Invalid, Deaf-and-Dumb, Deaf or Hard-of-hearing, Person who Deaf-Mute is deaf or hard of hearing Speech/Communication Dumb, “One who talks Person with a speech / communication Disability bad" disability Learning Disability Retarded, Slow, Brain- Learning disability, Cognitive Damaged, “Special ed” disability, Person with a learning or cognitive disability Mental Health Disability Hyper-sensitive, Psycho, Person with a psychiatric disability, Crazy, Insane, Wacko, Person with a mental health disability Nuts Mobility/Physical Handicapped, Physically Wheelchair user, Physically disabled, Disability Challenged, “Special,” Person with a mobility or physical Deformed, Cripple, Gimp, disability Spastic, Spaz, Wheelchair- bound, Lame Emotional Disability Emotionally disturbed Emotionally disabled, Person with an emotional disability Cognitive Disability Retard, Mentally retarded, Cognitively/Developmentally “Special ed” disabled, Person with a cognitive/developmental disability Short Stature, Little Dwarf, Midget Someone of short stature, Little Person Person Health Conditions Victim, Someone “stricken Survivor, Someone “living with” a with” a disability (i.e. specific disability (i.e. “someone “someone stricken with living with cancer or AIDS”) cancer” or “an AIDS victim”) NYLN & KASA1 General Tips Use a normal volume and tone when speaking to persons with disabilities. -

Hospice Care Network Hospice Care Network Northwell Health at Home Northwell Health Post-Acute Services 1 “None of Us, Including Me, Ever Do Great Things
Hospice Care Network Hospice Care Network 2019 Annual Report MANAGEMENT TEAM ADMINISTRATIVE LEADERSHIP MEDICAL LEADERSHIP Executive Director – Maureen Hinkelman, RN, MA Medical Director – Lori Ann Attivissimo, MD, FACP, FAAHPM, HMDC Associate Executive Director of Clinical Operations – Orael Keenan, RN, MSN Hospice Physician – Edward Halbridge, MD ABOUT US Medical Director – Lori Ann Attivissimo, MD, FACP, FAAHPM, HMDC Hospice Physician – Joi Marszalek, DO Our Mission Assistant Vice President of Counseling & Pediatric Services – Mary Gravina, LCSW Hospice Physician – Eirene Milano, MD Our mission is to enable people to live in peace and with dignity in a caring environment during the final stages of life by Assistant Vice President of Hospice Operations – Marie Zanotelli Hospice Physician – Sonia Tercero Moreno, MD offering care and comfort both to them and to those with whom they share their lives. Assistant Vice President of Inpatient Hospice Services – Darrin London, ANP Hospice Physician - Dimitris Platis, MD Hospice Physician - Tarek Zetoune, MD We develop and provide individualized programs of care and supportive services during dying, death and bereavement that enhance quality of life by addressing physical, emotional, spiritual and social needs. Nurse Practitioner – Carmen Bassaragh, ANP-C PATIENT CARE AND BUSINESS LEADERSHIP Nurse Practitioner – Lori Finkel, ANP-BC, CHPN Director of Admissions – Linda Rossi, RN, CHPN Background Nurse Practitioner – Tara Lauria, ANP-C Director of Financial and Operations Management - Letizia Cinelli Hospice Care Network is a not for profit healthcare organization serving patients and families in Nassau, Suffolk and Queens Nurse Practitioner – Darrin London, ANP counties. Hospice Care Network has been helping patients since 1988 and is a proud member of Northwell Health. -

A Study of the Use of Clinician I Personnel to Perform Intravenous Therapy
Old Dominion University ODU Digital Commons OTS Master's Level Projects & Papers STEM Education & Professional Studies 1996 A Study of the Use of Clinician I Personnel to Perform Intravenous Therapy Laura L. Walker Old Dominion University Follow this and additional works at: https://digitalcommons.odu.edu/ots_masters_projects Part of the Education Commons Recommended Citation Walker, Laura L., "A Study of the Use of Clinician I Personnel to Perform Intravenous Therapy" (1996). OTS Master's Level Projects & Papers. 334. https://digitalcommons.odu.edu/ots_masters_projects/334 This Master's Project is brought to you for free and open access by the STEM Education & Professional Studies at ODU Digital Commons. It has been accepted for inclusion in OTS Master's Level Projects & Papers by an authorized administrator of ODU Digital Commons. For more information, please contact [email protected]. A STUDY OF THE USE CLINICIAN I PERSONNEL TO PERFORM INTRAVENOUS THERAPY A Research Paper Presented to the Graduate Faculty of the Department of Occupational and Technical Studies at Old Dominion University In Partial Fulfillment Of the Requirements for the Degree Master of Science in Education by Laura L. Walker August 1996 APPROVAL PAGE This research paper was prepared under the direction of Dr. John M. Ritz, Graduate Advisor. It was submitted to the Graduate Program Director of Occupational and Technical Studies as partial fulfillment of the requirements for the Degree of Master of Science in Education. "-""' Date: !s -I4- - 7b · Graduate Advisor and Graduate Program Director ACKNOWLEDGMENTS This study on the use of unlicensed assistive personnel in health care would have been difficult to prepare without the assistance of the staff members of the Progressive Care Unit of Children's Hospital of the King's Daughters, Norfolk, Virginia. -

Posted on May 5, 2021 Sites with Asterisks (**) Are Able to Vaccinate 16-17 Year Olds
Posted on May 5, 2021 Sites with asterisks (**) are able to vaccinate 16-17 year olds. Updated at 4:00 PM All sites are able to vaccinate adults 18 and older. Visit www.vaccinefinder.org for a map of vaccine sites near you. Parish Facility Street Address City Website Phone Acadia ** Acadia St. Landry Hospital 810 S Broadway Street Church Point (337) 684-4262 Acadia Church Point Community Pharmacy 731 S Main Street Church Point http://www.communitypharmacyrx.com/ (337) 684-1911 Acadia Thrifty Way Pharmacy of Church Point 209 S Main Street Church Point (337) 684-5401 Acadia ** Dennis G. Walker Family Clinic 421 North Avenue F Crowley http://www.dgwfamilyclinic.com (337) 514-5065 Acadia ** Walgreens #10399 806 Odd Fellows Road Crowley https://www.walgreens.com/covid19vac Acadia ** Walmart Pharmacy #310 - Crowley 729 Odd Fellows Road Crowley https://www.walmart.com/covidvaccine Acadia Biers Pharmacy 410 N Parkerson Avenue Crowley (337) 783-3023 Acadia Carmichael's Cashway Pharmacy - Crowley 1002 N Parkerson Avenue Crowley (337) 783-7200 Acadia Crowley Primary Care 1325 Wright Avenue Crowley (337) 783-4043 Acadia Gremillion's Drugstore 401 N Parkerson Crowley https://www.gremillionsdrugstore.com/ (337) 783-5755 Acadia SWLA CHS - Crowley 526 Crowley Rayne Highway Crowley https://www.swlahealth.org/crowley-la (337) 783-5519 Acadia Miller's Family Pharmacy 119 S 5th Street, Suite B Iota (337) 779-2214 Acadia ** Walgreens #09862 1204 The Boulevard Rayne https://www.walgreens.com/covid19vac Acadia Rayne Medicine Shoppe 913 The Boulevard Rayne https://rayne.medicineshoppe.com/contact -

The Allied Health Care Professional's Role in Assisting Medical Decision
LWW/TLD TLD200107 April 20, 2012 16:4 Top Lang Disorders Vol. 32, No. 2, pp. 119–136 Copyright c 2012 Wolters Kluwer Health | Lippincott Williams & Wilkins The Allied Health Care Professional’s Role in Assisting Medical Decision Making at the End of Life Heather Lambert As a patient approaches the end of life, he or she faces a number of very difficult medical decisions. Allied health care professionals, including speech–language pathologists (SLPs) and occupational therapists (OTs), can be instrumental in assisting their patients to make advance care plans, al- though their traditional job descriptions do not include this role. The allied health care professional is often in a trusted position, permitting insight into the values and beliefs of the patient and fa- cilitating the depth of communication necessary when making difficult decisions. Professionals who work with clients at the end of life need to be aware of the many issues surrounding end- of-life decision making and the preparation of advance directives for care. This article provides an overview of the complex issues the practicing clinician needs to keep in mind when assisting clients with advance care planning. This service requires that clinicians step outside their roles as rehabilitation experts, a move that is supported by professional associations. The concepts of medical decision making and informed consent are discussed in the context of decisions made in advance of illness at the end of life. The professional needs also to be aware of the legali- ties of advance decision making, as laws and statutes differ between states/provinces. There are overarching pieces of legislation that inform local legal and policy issues; the impact of these is briefly addressed. -

Walker-Hackensack-Akeley School District (0113-01)
Special Education Program Compliance Review Final Report June 29, 2018 Walker-Hackensack-Akeley School District (0113-01) Eric Pingrey, Superintendent Eva M Pohl, Director of Special Education Table of Contents Introduction and Authority .................................................................................................................. 3 Scope of Monitoring ........................................................................................................................ 3 Resulting Findings and Corrective Action ....................................................................................... 3 District Overview ............................................................................................................................. 4 Monitoring Findings by Area ............................................................................................................... 4 Area 1: Governance ........................................................................................................................ 4 Area 2: Facilities, Equipment and Materials .................................................................................... 8 Area 3: Child Find and Evaluation ................................................................................................. 10 Area 4: IEP and IFSP Process and Implementation ...................................................................... 14 Summary of Corrective Action Required .......................................................................................... -

Vehicle Acquisition
VEHICLE ACQUISITION F ederal Transit Administration Americans with Disabilities Act Circular C 4710.1 Draft Chapter for Public Comment October 2012 TABLE OF CONTENTS 1 INTRODUCTION 1 1.1 THE DOT ADA REGULATIONS 1 1.2 PROVIDING SERVICE ON BEHALF OF ANOTHER ENTITY: “STAND IN THE SHOES” 1 2 ACQUISITION REQUIREMENTS FOR PUBLIC ENTITIES 3 2.1 BUSES AND VANS 4 2.2 RAPID RAIL AND LIGHT RAIL 5 2.3 COMMUTER RAIL 6 2.4 OTHER CONSIDERATIONS 7 2.5 DEMAND RESPONSIVE SERVICE 8 3 THE MAIN ELEMENTS OF ACCESSIBLE VEHICLES 10 3.1 BUSES AND VANS 13 3.2 RAPID RAIL VEHICLES 17 3.3 LIGHT RAIL VEHICLES 18 3.4 COMMUTER RAIL CARS 21 3.5 OTHER CONSIDERATIONS 23 4 ENSURING THAT VEHICLES ARE COMPLIANT 24 4.1 UNDERSTANDING THE SPECIFICATIONS 24 4.2 OBTAINING PUBLIC INPUT 24 4.3 ADDITIONAL SPECIFICATIONS 25 4.4 INSPECTIONS 25 5 DEFINITIONS 26 6 AUTHORITIES 28 7 REFERENCES 29 APPENDICES APPENDIX 1 SAMPLE BUS AND VAN SPECIFICATION CHECKLIST !"#$#%#$&'()*+,($$ -./')+.$#)0*'1'2'34$&/,52.($6$%(,72$ 8)239.($:;<:$ =,>.$<$37$:? ! 1 INTRODUCTION This Circular chapter on vehicle acquisition serves as a reference document for public transportation providers acquiring vehicles to ensure that these vehicles meet the requirements of the U.S. Department of Transportation (DOT) Americans with Disabilities Act (ADA) regulations. It is the goal of the Federal Transit Administration (FTA) to help transportation providers meet their obligations under the ADA by outlining the regulations, describing effective practices, and presenting the information in an easy-to-use format. Please note that this Circular does not alter, amend, or otherwise affect the DOT ADA regulations themselves; transportation providers are advised to use this Circular in addition to (not in lieu of) the DOT ADA regulations. -

Interpretative Statement: Delegation of Health Services in Iowa Schools Melissa Walker, School Nurse Consultant, Iowa Department of Education 2016-2017
Iowa Department of Education Interpretative Statement: Delegation of Health Services in Iowa Schools Melissa Walker, School Nurse Consultant, Iowa Department of Education 2016-2017 Interpretative Statement: Delegation of Health Services in Iowa Schools Purpose: Iowa students, as healthcare consumers, have the right to nursing care that meets the legal standards of health care regardless of the setting (National Council of State Boards of Nursing [NCSBN], 2005) (IAC 655 Chapter 6). School nurses are accountable for their practice of nursing in the educational setting and are also an integral member of the interdisciplinary education team to provide student’s access to quality instruction in the least restrictive, safe school environment. School nurses ensure that students receive health services for physical or mental health conditions that permit school attendance so they may equally access education as their peers and also assist parents or legal guardians to reasonably meet compulsory attendance regulations for their child pursuant to Iowa Code 299. All health services provided to students that constitute nursing or any activity representing nursing in the school setting is a regulatory responsibility of the state licensing board of Nursing (NCSBN, 2005). The purpose of this statement is to provide a resource for Iowa school nurses to maintain accountability in safe, effective nursing practice by working with and through others when using professional judgment in the delegation of nursing tasks for students who require health services to attend school (NCSBN, 2005). Background: Delegation is used in many professional arenas of employment, to include education and healthcare. Nursing delegation in schools is the process conducted by a nurse to transfer to a competent individual the authority to perform selected nursing tasks or activities in selected situations for a student (NCSBN, 2005). -

Battery Powered Wheelchair and Mobility Aid Guidance Document
Battery Powered Wheelchair and SafetyMobility requirements applicableAid toGuidance the carriage of battery powered Document wheelchairs and mobility aids when carried by passengers travelling by air Based on the 2019 Regulation compliance with the IATA Dangerous Goods Introduction Regulations. This document is based on the provisions set out in Passengers may only travel with a battery-powered the 2019-2020 Edition of the International Civil mobility aid with the airline’s approval. Proper pre- Aviation Organization (ICAO) Technical Instruction notification by the user helps to ensure that: for the Safe Transport of Dangerous Goods by Air (Technical Instructions) and the 60th Edition of the ▪ all in the transportation chain know what IATA Dangerous Goods Regulations (DGR). device(s) and battery type(s) they are transporting; Information on the DGR can be found here: ▪ how to properly load and handle them; and https://www.iata.org/publications/dgr/Pages/index. ▪ what to do if an incident or accident occurs aspx either in-flight or on the ground. The batteries that power wheelchairs and mobility The pilot-in-command must be informed of the aids are considered dangerous goods when carried location of the mobility aid with installed batteries, by air. These and some other dangerous goods that removed batteries and spare batteries, to best deal are permitted for carriage by passengers can be with any emergencies that may occur. transported safely by air provided certain safety requirements are met. The requirements are Inadvertent operation of battery powered mobility detailed in the IATA Dangerous Goods Regulations, aids can cause friction or electrical load which which are based on the ICAO Technical could lead to a fire. -
2017 Ada Update on Service Animal Rules
2017 ADA UPDATE ON SERVICE ANIMAL RULES The California Hotel & Lodging Association receives many questions regarding the rights and obligations of lodging establishments with respect to service animals. This document contains CHLA’s updated discussion of this topic. First, there has been a significant change regarding California law related to service animals. This change, which is discussed below, will make it easier for lodging operators to deal with guests who claim that their pets are service animals. Here are the basics of California law as it relates to service animals: • There was a time when the California Department of Fair Employment and Housing, which administers California’s Fair Employment and Housing Act (Act), took the position that the Act applied to the lodging industry. At that time, there was concern that lodging operators would have to comply with the more stringent requirements of the Act: (1) it is not limited to dogs— depending on the circumstances, the FEHA protects other types of animals and treats them as service animals; and (2) it provides protections for people who use “comfort” and “companion” animals. Contrary to the Department’s earlier position, however, CHLA was recently advised that the Act only applies to homes, condos, and apartments, and that it does not apply to hotels! • It is important for lodging operators to bear in mind that although the 2011 revisions to the ADA rules regarding service animals expressly state that (1) only dogs qualify as service animals,1 and that (2) “comfort” and “companion” dogs are not service animals,2 if a local jurisdiction in California has broader, more stringent rules than the ADA, the local rules must be complied with. -

Relationship Between Body Image and Physical Functioning Following Rehabilitation for Lower-Limb Amputation
Western University Scholarship@Western Physical Therapy Publications Physical Therapy School 2019 Relationship between body image and physical functioning following rehabilitation for lower-limb amputation Jessica Desrochers Courtney Frengopoulos Michael W.C. Payne Ricardo Viana Susan W. Hunter Follow this and additional works at: https://ir.lib.uwo.ca/ptpub Part of the Physical Therapy Commons Relationship between body image and physical functioning following rehabilitation for lower limb amputation Jessica Desrochers BHSc1; Courtney Frengopoulos MSc2; Michael WC Payne MD3; Ricardo Viana MD3; Susan W Hunter PhD3,4 1. School of Health Studies, University of Western Ontario, London, ON; 2. Faculty of Health & Rehabilitation Sciences, University of Western Ontario, London, ON; 3. Department of Physical Medicine & Rehabilitation, Schulich School of Medicine and Dentistry, University of Western Ontario, London, ON; 4. School of Physical Therapy, University of Western Ontario, London, ON. Running title: Body image and mobility in lower extremity amputees Corresponding author: Dr. Susan W Hunter University of Western Ontario School of Physical Therapy Room 1588, Elborn College 1201 Western Road, London, Ontario Email: [email protected] Telephone: 519-661-2111 ext88845 Funding: This work was supported by the St. Joseph’s Foundation Cognitive Vitality and Brain Health Seed Funding Opportunity. The funding body had no involvement in the conduct of the study. Conflict of interest: None to report. Relationship between body image and physical functioning following rehabilitation for lower limb amputation ABSTRACT Objectives: To evaluate change in body image and the association between body image at discharge and mobility 4 months post rehabilitation. Methods: Prospective cohort of consecutive admissions to inpatient prosthetic rehabilitation. -

The Economics of Enhancing Accessibility Estimating the Benefits and Costs of Participation
The Economics of Enhancing Accessibility Estimating the Benefits and Costs of Participation Discussion01 Paper 2017 • 01 Bridget R.D. Burdett TDG Ltd, Hamilton, New Zealand Stuart M. Locke University of Waikato Management School, Hamilton, New Zealand Frank Scrimgeour Institute for Business Research, University of Waikato, Hamilton, New Zealand The Economics of Enhancing Accessibility Estimating the Benefits and Costs of Participation Discussion Paper No. 2017-01 Prepared for the Roundtable on Economics of Accessible Transport 3-4 March 2016, Paris Bridget R.D. Burdett TDG Ltd, Hamilton, New Zealand Stuart M. Locke Department of Finance, University of Waikato Management School, Hamilton, New Zealand Frank Scrimgeour Institute for Business Research, University of Waikato, Hamilton, New Zealand February 2017 The International Transport Forum The International Transport Forum is an intergovernmental organisation with 57 member countries. It acts as a think tank for transport policy and organises the Annual Summit of transport ministers. ITF is the only global body that covers all transport modes. The ITF is politically autonomous and administratively integrated with the OECD. The ITF works for transport policies that improve peoples’ lives. Our mission is to foster a deeper understanding of the role of transport in economic growth, environmental sustainability and social inclusion and to raise the public profile of transport policy. The ITF organises global dialogue for better transport. We act as a platform for discussion and pre- negotiation of policy issues across all transport modes. We analyse trends, share knowledge and promote exchange among transport decision-makers and civil society. The ITF’s Annual Summit is the world’s largest gathering of transport ministers and the leading global platform for dialogue on transport policy.