Assistive Technologies for People with Disabilities Part II: Current and Emerging Technologies
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Tips for Communicating with People with Disabilities
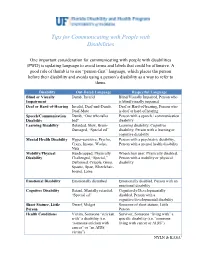
Tips for Communicating with People with Disabilities One important consideration for communicating with people with disabilities (PWD) is updating language to avoid terms and labels that could be offensive. A good rule of thumb is to use “person-first” language, which places the person before their disability and avoids using a person’s disability as a way to refer to them. Disability Out-Dated Language Respectful Language Blind or Visually Dumb, Invalid Blind/Visually Impaired, Person who Impairment is blind/visually impaired Deaf or Hard-of-Hearing Invalid, Deaf-and-Dumb, Deaf or Hard-of-hearing, Person who Deaf-Mute is deaf or hard of hearing Speech/Communication Dumb, “One who talks Person with a speech / communication Disability bad" disability Learning Disability Retarded, Slow, Brain- Learning disability, Cognitive Damaged, “Special ed” disability, Person with a learning or cognitive disability Mental Health Disability Hyper-sensitive, Psycho, Person with a psychiatric disability, Crazy, Insane, Wacko, Person with a mental health disability Nuts Mobility/Physical Handicapped, Physically Wheelchair user, Physically disabled, Disability Challenged, “Special,” Person with a mobility or physical Deformed, Cripple, Gimp, disability Spastic, Spaz, Wheelchair- bound, Lame Emotional Disability Emotionally disturbed Emotionally disabled, Person with an emotional disability Cognitive Disability Retard, Mentally retarded, Cognitively/Developmentally “Special ed” disabled, Person with a cognitive/developmental disability Short Stature, Little Dwarf, Midget Someone of short stature, Little Person Person Health Conditions Victim, Someone “stricken Survivor, Someone “living with” a with” a disability (i.e. specific disability (i.e. “someone “someone stricken with living with cancer or AIDS”) cancer” or “an AIDS victim”) NYLN & KASA1 General Tips Use a normal volume and tone when speaking to persons with disabilities. -

On the Mystery of Human Consciousness
On the mystery of human consciousness Egon Gál 23 August 2007 Philosophers and natural scientists regularly dismiss consciousness as irrelevant. However, even its critics agree that consciousness is less a problem than a mystery. One way into the mystery is through an understanding of autism. It started with a letter from Michaela Martinková: Dear Egon Gál, Our eldest son, aged almost eight, has Asperger’s Syndrome (AS). It is a diagnosis that falls into the autistic spectrum, but his IQ is very much above average. In an effort to find out how he thinks, I decided that I must find out how we think, and so I read into the cognitive sciences and epistemology. I found what I needed there, although I have an intense feeling that precisely the way of thinking of such people as our son is missing from the mosaic of these sciences. And I think that this missing piece could rearrange the whole mosaic. In the book Philosophy and the Cognitive Sciences, [1] you write, among other things: “Actually the only handicap so far observed in these children (with autism and AS) is that they cannot use human psychology. They cannot postulate intentional states in their own minds and in the minds of other people.” I think that deeper knowledge of autism, and especially of Asperger’s Syndrome as its version found in people with higher IQ in the framework of autism, could be immensely enriching for the cognitive sciences. I am convinced that these people think in an entirely different way from us. [2] Why the present interest in autism? It is generally known that some people whose diagnosis falls under Asperger’s Syndrome, namely people with Asperger’s Syndrome and high-functional autism, show a remarkable combination of highly above-average intelligence and well below-average social ability. -

Becoming Autistic: How Do Late Diagnosed Autistic People
Becoming Autistic: How do Late Diagnosed Autistic People Assigned Female at Birth Understand, Discuss and Create their Gender Identity through the Discourses of Autism? Emily Violet Maddox Submitted in accordance with the requirements for the degree of Master of Philosophy The University of Leeds School of Sociology and Social Policy September 2019 1 Table of Contents ACKNOWLEDGEMENTS ................................................................................................................................... 5 ABSTRACT ....................................................................................................................................................... 6 ABBREVIATIONS ............................................................................................................................................. 7 CHAPTER ONE ................................................................................................................................................. 8 INTRODUCTION .............................................................................................................................................. 8 1.1 RESEARCH OBJECTIVES ........................................................................................................................................ 8 1.2 TERMINOLOGY ................................................................................................................................................ 14 1.3 OUTLINE OF CHAPTERS .................................................................................................................................... -

Constructing Narratives and Identities in Auto/Biography About Autism
RELATIONAL REPRESENTATION: CONSTRUCTING NARRATIVES AND IDENTITIES IN AUTO/BIOGRAPHY ABOUT AUTISM by MONICA L. ORLANDO Submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy Department of English CASE WESTERN RESERVE UNIVERSITY May 2015 2 CASE WESTERN RESERVE UNIVERSITY SCHOOL OF GRADUATE STUDIES We hereby approve the dissertation of Monica Orlando candidate for the degree of Doctor of Philosophy.* Committee Chair Kimberly Emmons Committee Member Michael Clune Committee Member William Siebenschuh Committee Member Jonathan Sadowsky Committee Member Joseph Valente Date of Defense March 3, 2015 * We also certify that written approval has been obtained for any proprietary material contained therein. 3 Dedications and Thanks To my husband Joe, for his patience and support throughout this graduate school journey. To my family, especially my father, who is not here to see me finish, but has always been so proud of me. To Kim Emmons, my dissertation advisor and mentor, who has been a true joy to work with over the past several years. I am very fortunate to have been guided through this project by such a supportive and encouraging person. To the graduate students and faculty of the English department, who have made my experience at Case both educational and enjoyable. I am grateful for having shared the past five years with all of them. 4 Table of Contents Abstract ............................................................................................................................... 5 Chapter 1: Introduction Relationality and the Construction of Identity in Autism Life Writing ........................ 6 Chapter 2 Clara Claiborne Park’s The Siege and Exiting Nirvana: Shifting Conceptions of Autism and Authority ................................................................................................. 53 Chapter 3 Transformative Narratives: Double Voicing and Personhood in Collaborative Life Writing about Autism .............................................................................................. -

A Memoir of Brain Change and Emotional Awakening by John Elder Robison
Discussion Guide Switched On: A Memoir of Brain Change and Emotional Awakening By John Elder Robison 1. Robison was diagnosed with Asperger’s at age forty. He claims that his “diagnosis was a huge relief and a source of empowerment” What does he mean? 2. In Chapter 6, Robison tells the story of being the first responder at the scene of a car accident. He is not emotionally affected by the situation. “Before TMS, all I knew was that I was a good guy in a crisis because my logical mind took charge.” He continues, “Even without feeling the expected emotions, I did the right thing… My sense of right and wrong was quite well developed, and I did the best I could for other people. It’s just that my senses and abilities were limited, so I didn’t always do what they expected.” Did you find this surprising? Have you known people whose facial expressions struck you as odd or overly blank? How did it make you feel, and how did you interpret their behavior? 3. Why did Transcranial Magnetic Stimulation (TMS) appeal to the author? How is the title relevant to the story? 4. In Chapter 14, Robison describes his reaction to his first TMS treatment after leaving the research hospital and driving home in his car listening to music. Describe the significance of this episode. 5. Robison often says that before TMS, he could relate better to machines than to people, yet, he wasn’t void of feelings, and he felt socially isolated. Discuss Robison’s relationships before and after TMS. -

Vehicle Acquisition
VEHICLE ACQUISITION F ederal Transit Administration Americans with Disabilities Act Circular C 4710.1 Draft Chapter for Public Comment October 2012 TABLE OF CONTENTS 1 INTRODUCTION 1 1.1 THE DOT ADA REGULATIONS 1 1.2 PROVIDING SERVICE ON BEHALF OF ANOTHER ENTITY: “STAND IN THE SHOES” 1 2 ACQUISITION REQUIREMENTS FOR PUBLIC ENTITIES 3 2.1 BUSES AND VANS 4 2.2 RAPID RAIL AND LIGHT RAIL 5 2.3 COMMUTER RAIL 6 2.4 OTHER CONSIDERATIONS 7 2.5 DEMAND RESPONSIVE SERVICE 8 3 THE MAIN ELEMENTS OF ACCESSIBLE VEHICLES 10 3.1 BUSES AND VANS 13 3.2 RAPID RAIL VEHICLES 17 3.3 LIGHT RAIL VEHICLES 18 3.4 COMMUTER RAIL CARS 21 3.5 OTHER CONSIDERATIONS 23 4 ENSURING THAT VEHICLES ARE COMPLIANT 24 4.1 UNDERSTANDING THE SPECIFICATIONS 24 4.2 OBTAINING PUBLIC INPUT 24 4.3 ADDITIONAL SPECIFICATIONS 25 4.4 INSPECTIONS 25 5 DEFINITIONS 26 6 AUTHORITIES 28 7 REFERENCES 29 APPENDICES APPENDIX 1 SAMPLE BUS AND VAN SPECIFICATION CHECKLIST !"#$#%#$&'()*+,($$ -./')+.$#)0*'1'2'34$&/,52.($6$%(,72$ 8)239.($:;<:$ =,>.$<$37$:? ! 1 INTRODUCTION This Circular chapter on vehicle acquisition serves as a reference document for public transportation providers acquiring vehicles to ensure that these vehicles meet the requirements of the U.S. Department of Transportation (DOT) Americans with Disabilities Act (ADA) regulations. It is the goal of the Federal Transit Administration (FTA) to help transportation providers meet their obligations under the ADA by outlining the regulations, describing effective practices, and presenting the information in an easy-to-use format. Please note that this Circular does not alter, amend, or otherwise affect the DOT ADA regulations themselves; transportation providers are advised to use this Circular in addition to (not in lieu of) the DOT ADA regulations. -

Praise for Switched On
Praise for Switched On ‘Astonishing, brave…reads like a medical thriller and keeps you wonder- ing what will happen next…[Robison] takes readers for a ride through the thorny thickets of neuroscience and leaves us wanting more. He is deft at explaining difficult concepts and doesn’t shy from asking hard questions. This is a truly unusual memoir—both poignant and scientifically important.’ Washington Post ‘Robison’s writings are…logical, restrained, lacking in self-pity… Like Awakenings, this book raises deep philosophical problems.’ The Times ‘Fascinating for its insights into Asperger’s and research, this engrossing record will make readers reexamine their preconceptions about this syn- drome and the future of brain manipulation.’ Booklist ‘Like books by Andrew Solomon and Oliver Sacks, Switched On offers an opportunity to consider mental processes through a combination of powerful narrative and informative medical context.’ BookPage ‘A fascinating companion to the previous memoirs by this masterful storyteller.’ Kirkus ‘John Elder Robison is an extraordinary guide, carefully elucidating the cutting-edge science behind this revolutionary new brain therapy, TMS, alongside the compelling story of the impact it has on his relationships, his thinking and emotions, and indeed his very identity. At the heart of Switched On are fundamental questions of who we are, where our identity resides, of difference and disability and free will, that are brought into sharp focus by Robison’s lived experience.’ Graeme Simsion, author of The Rosie Project -

DM a Talent: ADHD Employer Guide
Supported by DMA Talent: ADHD Employer Guide DMA Talent: DMA Talent: ADHD Employer Guide Copyright / DMA (2021) 01 DMA Talent: ADHD Employer Guide Contents DMA Talent’s Employer Guide Series .............................................................................................. 03 Definitions and Terminology ........................................................................................................................04 What is Neurodiversity? .........................................................................................................................................04 What is ADHD? ...............................................................................................................................................................04 Seeking a Diagnosis for ADHD ..................................................................................................................08 What are the Employer’s Responsibilities? ..............................................................................................09 Qualities Associated with ADHD ................................................................................................................11 Simple Ways to Modify the Recruitment Process ............................................................. 12 Job Advertisements .................................................................................................................................................... 12 Work Trials and Skills Testing .............................................................................................................................. -

Battery Powered Wheelchair and Mobility Aid Guidance Document
Battery Powered Wheelchair and SafetyMobility requirements applicableAid toGuidance the carriage of battery powered Document wheelchairs and mobility aids when carried by passengers travelling by air Based on the 2019 Regulation compliance with the IATA Dangerous Goods Introduction Regulations. This document is based on the provisions set out in Passengers may only travel with a battery-powered the 2019-2020 Edition of the International Civil mobility aid with the airline’s approval. Proper pre- Aviation Organization (ICAO) Technical Instruction notification by the user helps to ensure that: for the Safe Transport of Dangerous Goods by Air (Technical Instructions) and the 60th Edition of the ▪ all in the transportation chain know what IATA Dangerous Goods Regulations (DGR). device(s) and battery type(s) they are transporting; Information on the DGR can be found here: ▪ how to properly load and handle them; and https://www.iata.org/publications/dgr/Pages/index. ▪ what to do if an incident or accident occurs aspx either in-flight or on the ground. The batteries that power wheelchairs and mobility The pilot-in-command must be informed of the aids are considered dangerous goods when carried location of the mobility aid with installed batteries, by air. These and some other dangerous goods that removed batteries and spare batteries, to best deal are permitted for carriage by passengers can be with any emergencies that may occur. transported safely by air provided certain safety requirements are met. The requirements are Inadvertent operation of battery powered mobility detailed in the IATA Dangerous Goods Regulations, aids can cause friction or electrical load which which are based on the ICAO Technical could lead to a fire. -
2017 Ada Update on Service Animal Rules
2017 ADA UPDATE ON SERVICE ANIMAL RULES The California Hotel & Lodging Association receives many questions regarding the rights and obligations of lodging establishments with respect to service animals. This document contains CHLA’s updated discussion of this topic. First, there has been a significant change regarding California law related to service animals. This change, which is discussed below, will make it easier for lodging operators to deal with guests who claim that their pets are service animals. Here are the basics of California law as it relates to service animals: • There was a time when the California Department of Fair Employment and Housing, which administers California’s Fair Employment and Housing Act (Act), took the position that the Act applied to the lodging industry. At that time, there was concern that lodging operators would have to comply with the more stringent requirements of the Act: (1) it is not limited to dogs— depending on the circumstances, the FEHA protects other types of animals and treats them as service animals; and (2) it provides protections for people who use “comfort” and “companion” animals. Contrary to the Department’s earlier position, however, CHLA was recently advised that the Act only applies to homes, condos, and apartments, and that it does not apply to hotels! • It is important for lodging operators to bear in mind that although the 2011 revisions to the ADA rules regarding service animals expressly state that (1) only dogs qualify as service animals,1 and that (2) “comfort” and “companion” dogs are not service animals,2 if a local jurisdiction in California has broader, more stringent rules than the ADA, the local rules must be complied with. -

Theory of Mind and Communication in Autism Francesca Gabrielle
Theory of Mind and Communication in Autism Francesca Gabrielle Elizabeth Happe, MRC Cognitive Development Unit, and Department of Psychology, University College, London. Thesis submitted for the degree of Ph.D. in Psychology, University of London. October, 1991. 1 Acknowledgements My greatest thanks must go to Uta Frith, who made writing this thesis not only possible but pleasurable. I have benefitted enormously from her unstinting encouragement, her insightful criticisms, and her great kindness. I would also like to thank all my colleagues at the MRC Cognitive Development Unit, particularly Annette Kanniloff-Smith, Alan Leslie and John Morton, for teaching me so much which I hadn't realised I didn't know. Thanks also go to Fran Siddons, James Blair and other friends, who have been invaluable in the discussion of fledgling ideas. I am also extremely grateful to the autistic children and adults who took part in the studies reported here. They, along with their teachers and parents, have taught me a great deal about autism, and shown me how much more there is still to discover. Lastly, my thanks go to my family for their unfailing support and enthusiasm. A.M.D.G. 2 Abstract Recent work investigating the biological and cognitive nature of autism is reviewed. The hypothesis that autistic individuals suffer from a specific impairment in theory of mind, and the relevance of this notion to the diagnosis of Asperger's syndrome, is discussed. Theory of mind explanations of autism must account for the minority of autistic subjects who pass false belief tasks. Two possible accounts are considered; delay versus "hacking". -

Office of Diversity & Equal Opportunity April/May, 2016
Office of Diversity & Equal Opportunity April/May, 2016 VOICES William & Mary is committed to inclusive excellence. our focus. This work is not aligned with a single office, Building on our core value of diversity, we strive to be a but the shared responsibility of all. We define diversity place where equity and inclusion are integral parts of all in its broadest terms and celebrate how this makes that we do. We work to create a community that is William & Mary a better institution. representative of individuals with different backgrounds, ___________________________________________ talents and skills. We work to ensure that William & VOICES is the monthly e-newsletter, and provides an Mary is a place where all faculty, staff, students and update on the university's diversity efforts in facilitating alumni feel supported and affirmed. From classroom and supporting diversity and inclusion. Each issue shares discussions and study abroad experiences, to equitable the good work of academic and administrative departments, students, affinity groups and more. Past and transparent recruitment, hiring and promotion issues are available at the Diversity & Equal Opportunity processes, inclusive excellence is website: www.wm.edu/offices/diversity/voices/index. Neurodiversity Innovative Initiative at W&M Founded in 2012, William & Mary’s neurodiversity initiative is a unique effort to support students on our campus, to advocate for appreciating the value of neurodiversity, and to offer a model to other colleges and universities. Neurodiversity is an emerging philosophy and civil rights movement that seeks to acknowledge and appreciate the wide variety of human neurologies including Autism, ADHD, and others on par with gender, ethnicity or sexual orientation instead of seeing them at pathologies.