African Programme for Oiichocerciasis Control (Apoc)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

Living Through Nigeria's Six-Year
“When We Can’t See the Enemy, Civilians Become the Enemy” Living Through Nigeria’s Six-Year Insurgency About the Report This report explores the experiences of civilians and armed actors living through the conflict in northeastern Nigeria. The ultimate goal is to better understand the gaps in protection from all sides, how civilians perceive security actors, and what communities expect from those who are supposed to protect them from harm. With this understanding, we analyze the structural impediments to protecting civilians, and propose practical—and locally informed—solutions to improve civilian protection and response to the harm caused by all armed actors in this conflict. About Center for Civilians in Conflict Center for Civilians in Conflict (CIVIC) works to improve protection for civil- ians caught in conflicts around the world. We call on and advise international organizations, governments, militaries, and armed non-state actors to adopt and implement policies to prevent civilian harm. When civilians are harmed we advocate the provision of amends and post-harm assistance. We bring the voices of civilians themselves to those making decisions affecting their lives. The organization was founded as Campaign for Innocent Victims in Conflict in 2003 by Marla Ruzicka, a courageous humanitarian killed by a suicide bomber in 2005 while advocating for Iraqi families. T +1 202 558 6958 E [email protected] www.civiliansinconflict.org © 2015 Center for Civilians in Conflict “When We Can’t See the Enemy, Civilians Become the Enemy” Living Through Nigeria’s Six-Year Insurgency This report was authored by Kyle Dietrich, Senior Program Manager for Africa and Peacekeeping at CIVIC. -

YOBE STATE MINISTRY of HEALTH Situation Report
YOBE STATE MINISTRY OF HEALTH Situation Report TITLE COVID-19 Pandemic Situation Report SERIAL NUMBER 24 EPID-WEEK 21 DATE 23 May 2020 HIGHLIGHTS: Two (2) newly confirmed case(s) have been reported from Potiskum LGA Two (2) new case(s) have been admitted in the state isolation center Twenty-eight (28) contacts of the newly confirmed cases have been identified and line-listed by the contact tracing teams in Bade, Bursari, and Nguru LGAs No new discharge from the isolation centers Three (3) new alerts have been received and investigated in Potiskum, Damaturu, and Bade LGAs. EPIDEMIOLOGICAL SUMMARY: The total number of confirmed COVID-19 case(s) is forty-seven (47): Nineteen (19) cases from Damaturu, ten (10) cases from Nguru, nine (9) cases from Bade, three (3) cases from Potiskum, and one (1) case each from Geidam, Tarmuwa, Bursari, Fika, Gulani and Gujba LGAs Total confirmed case(s) of COVID-19 amongst Health Care Workers (HCWs) in the state is thirteen (13): Seven (7) nurses, four (4) doctors, one (1) physiotherapist, and one (1) laboratory scientist The total number of deaths due to COVID-19 in the state is six (6) Total number of case(s) who recovered and have been discharged from the state isolation centers is eight (8) The total number of contacts who completed the 14-days follow-up without symptoms as of today is one hundred and fifty-three (153) Thirty-two (32) confirmed cases in the isolation center are in stable condition The total number of samples taken for testing is ninety-one (91). -
ETT Report-No.32.V2
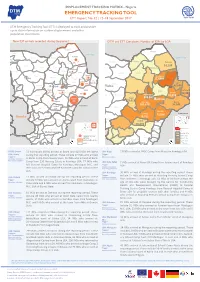
DISPLACEMENT TRACKING MATRIX - Nigeria DTM Nigeria EMERGENCY TRACKING TOOL ETT Report: No. 32 | 12–18 September 2017 IOM OIM DTM Emergency Tracking Tool (ETT) is deployed to track and provide up-to-date information on sudden displacement and other population movements New IDP arrivals recorded during the period DTM and ETT Cumulative Number of IDPs by LGA Abadam Abadam Yusufari Lake Chad Kukawa Yusufari Yunusari Mobbar Lake Chad± Nguru Karasuwa Niger Machina Yunusari Mobbar Abadam Kukawa Lake Chad Bade Guzamala 79 Nguru Karasuwa Kukawa Bursari 14,105 Geidam Gubio Bade Bade Guzamala Monguno Mobbar Nganzai Jakusko Bursari 6240 Marte Geidam Gubio Bade Guzamala Ngala Tarmua Monguno Magumeri Nganzai Jakusko Yobe 122,844 Marte 43 Gubio Monguno Jere Dikwa 7 Mafa Kala/BalgeYobe Ngala Maiduguri M.C. 122 Tarmua Nganzai Nangere Fune Damaturu Jigawa Magumeri 42,686 Borno 18 Yobe Marte Potiskum Ngala Kaga Konduga Bama Jere Mafa Kala/Balge Magumeri Dikwa 17 30 73 Yobe 49,480 Fika Gujba Nangere Fune Damaturu Maiduguri Mafa 74,858 Jere Dikwa Gwoza Potiskum Kaga Borno308,807 Kala-Balge MaiduBornoguri Damboa 799 19,619 KondugaKonduga Bama Gulani Cameroon Kag1a05,678 56,748 Chibok Konduga Fika Gujba Bama Biu 11 Madagali Askira/Uba Gwoza Michika Damboa Cameroon Kwaya Kusar 73,966Gwoza Hawul Damboa Bauchi Gombe Bayo Mubi North 76,795 Hong Gulani Shani Chibok Gombi Mubi South Madagali Biu Biu 16,378Chibok Maiha Askira/Uba Askira-Uba Inaccessible area Guyuk Song Michika Shelleng IDP severity Kwaya KusarKwaya Kusar Hawul Adamawa Hawul Less t han 10,788 Bauchi Gombe Bayo Mubi North Lamurde Number of new Bayo 10,788 - 25,813 HongAdamawa Numan Girei arrivals Shani Cameroon 25,813 - 56,749 Demsa Inaccessible area Shani Gombi Mubi South Yola South 56,749 - 122,770 Yola North Gombe 0 15 30 60 Km 122,770 Above Fufore LGAChad Adamawa Plateau Mayo-Belwa Shelleng Maiha Guyuk Song STATE: Borno 73 individuals (INDs) arrived at Bama and 129 INDs le� Bama LGA: Kaga 17 INDs arrived at NYSC Camp from Musari in Konduga LGA. -

Climate-Smart Agriculture in Yobe State of Nigeria
Climate-Smart Agriculture in Yobe state of Nigeria Climate-smart agriculture (CSA) considerations A• Agriculture is the mainstay for Yobe state economy P adaptation. There is the need to also integrate mitigation employing over 80 percent of the population. P M into the state’s climate-smart agriculture development Agricultural practices in the state are mainly rain-fed efforts. In addition, off-farm services related to CSA need with majority of the farmers engaged in small scale to be enhanced, including weather-smart and market- subsistence farming with millet, sorghum, cowpea and smart services. maize as major food crops and gum arabic, groundnut, sesame seed and cotton as cash crops. I• The Yobe state government places high priority on A significant proportion of the population are the development of the agricultural sector in the state. pastoralists rearing livestock such as cattle, sheep, The state ministry of agriculture is saddled with the goats, donkeys and horses at commercial level. responsibility of implementing agricultural policies that enables CSA. The broad strategic goals include A• The agricultural sector in the state is struggling to meet creating an operating environment that supports rapid the increasing food demand for its growing population modernization of agricultural production, processing, P as it battles with low productivity arising limited storage and distribution through supportive government investments, low farm input use, land tenure and climate policies. variability. In addition, the problem of flash floods, high temperature and incidences of pests and diseases have $• Funding for CSA is limited in the state and Nigeria in also aggravated the irrigation and upland farmers’ losses general, however there are opportunities to access and which consequently increase the incidence of poverty and utilize international climate finance from sources such as malnutrition in the state. -

Borno State, Nearly Tarmuwa Magumeri Kala/ Fune Jere Mafa 60 000 People Face the Threat of Famine Balge Nangere Dikwa (Phase 5)
N°32 SAHEL AND MAPSMARCH & FACTS 2016 WEST AFRICA Club No 44, November 2016 ONE OUT OF THREE PEOPLE IN NORTHEASTERN NIGERIA FACED WITH ACUTE FOOD INSECURITY August-September 2016 ccording to the fi ndings of the 1 Lake A Cadre harmonisé analysis of Abadam Yusufari Chad August 2016, some 4.4 million people in Yunusari Machina Mobbar Kukawa northeastern Nigeria were facing acute Nguru Karasuwa Guzamala food insecurity (phases 3-5) requiring Bade Borsari Mobbar urgent humanitarian assistance. In Bade Geidam Nganzai Monguro the worst affected and less acces- Jakusko Marte Yobe Ngala sible pockets of Borno state, nearly Tarmuwa Magumeri Kala/ Fune Jere Mafa 60 000 people face the threat of famine Balge Nangere Dikwa (phase 5). Boko Haram attacks and Damaturu Kaga Maiduguru Potiskum Konduga Bama suicide bombings continue to cause Fika Gujba fatalities and large-scale population Borno Gwoza displacement. This has had a negative Damboa Gulani impact on food consumption and Biu Chibok Madagali livelihood activities within both Askira/Uba Kwaya Michika displaced and host community house- Kusar Hawul Hong Bayo Mubi North holds. The situation continues to Shani Girie be particularly alarming in Borno, Mubi South Shelleng Maina Adamawa and Yobe which host large Song Adamawa numbers of internally displaced Lamurde people (IDPs). According to the Inter- Numan Gombi Demsa Yola North national Organization for Migration’s Yola South (IOM) June 2016 report, there are over Fufore Mayo- 1.4 million IDPs in Borno, 159 445 in Lake Abadam Bel Yusufari Chad Jada Yunusari Machina Mobbar Kukawa Adamawa and 111 671 in Yobe. New Phases of food insecurity Nguru Karasuwa Guzamala Bade Borsari Mobbar Bade Geidam Nganzai Monguro Jakusko Marte Yobe Ngala Tarmuwa Magumeri Kala/ Fune Jere Mafa Balge Nangere Dikwa Damaturu Kaga Maiduguru Potiskum Konduga Bama Fika arrivals of IDPs put additional stress Gujba Borno Gwoza Phase 1: Minimal Gulani Damboa Ganye Biu Chibok Madagali Askira/Uba Kwaya Michika Kusar Hawul Hong Bayo Mubi North Shani Girie Mubi South Shelleng Maina on host communities. -

GENDER ASSESSMENT January 2020
GENDER ASSESSMENT January 2020 Table of Contents List of graphs ....................................................................................................................................... ii List of table .......................................................................................................................................... ii Context .................................................................................................................................................... iii Objective .................................................................................................................................................. iii Methodology ........................................................................................................................................... iv Sampling .................................................................................................................................................. v Findings .................................................................................................................................................. vi Gender assessment analysis ................................................................................................................... 1 1. Socioeconomic activities and dynamics in the communities ........................................................ 2 1.1 Current daily activities of women compared to men ................................................................ 2 1.2 Type of livelihood -

Drought Occurrences and Its Implications on the Households in Yobe State, Nigeria Jude Nwafor Eze
Eze Geoenvironmental Disasters (2018) 5:18 Geoenvironmental Disasters https://doi.org/10.1186/s40677-018-0111-7 RESEARCH Open Access Drought occurrences and its implications on the households in Yobe state, Nigeria Jude Nwafor Eze Abstract The study assesses the extent of droughts and its implications on the households in the study area. This is to highlight the need to integrate drought adaptation options into the government development plans. Strategies for drought adaptation options in the study area have often been made without experimental foundations placed on the extent of drought and its implications on the households. To achieve this, the study employed Normalized Rainfall Index (NRI) to determine the extent of droughts and its implications on the households, which has much to offer in terms of policy decisions. The study also utilized questionnaire administrated to 400 households to determine the annual income from different occupations that yielded more income to the people in the study area using one-way analysis of variance (ANOVA). The NRI shows that the study area was characterized by mild to severe drought events. The first (1986–1995) and third (2006–2017) decades experienced high incidences of droughts, while the second decade (1996–2005), witnessed the least incidences of droughts. The result of the economic activities of the households reveals that 65% of the total household respondents were involved in farming, while 35% were involved in non-farming activities as their major source of livelihood. The analysis of variance on the economic activities that generated more income to the households in Yobe State shows that farming activities provided more opportunities for income generation. -

Power Grid Corridor Modelling for Efficient Electricity Distribution in Communities of Damaturu Nigeria Using GIS
International Journal of Advances in Scientific Research and Engineering (ijasre) E-ISSN : 2454-8006 DOI: 10.31695/IJASRE.2019.33154 Volume 5, Issue 4 April - 2019 Power Grid Corridor Modelling for Efficient Electricity Distribution in Communities of Damaturu Nigeria Using GIS Bala-Geidam M.1, Badema A.2 and Shuaibu, M. A.3 1Dept. of Basic Science, Yobe State College of Agriculture Gujba, Yobe State Nigeria 2Dept. of Geography, Yobe State University Damaturu, Yobe State, Nigeria 3Dept. of Surveying and Geoinformatics, Abubakar TafawaBalewa University Bauchi Nigeria _______________________________________________________________________________________ ABSTRACT This study focused on modelling of power grid corridor using geographic information system (GIS). The objectives are to map and evaluate the communities and existing Substations on national Grid with the aim of modelling new substations source for effective power distribution in the study area. The mapping of positions of the substations and communities around the grid was achieved using Etrex 10 handheld GPS receiver and the evaluation was carried out using the Location allocation analysis of ArcGIS 10.3. The result of the model reveals that ten (10) out of the thirty-two (32) communities found were on the national grid while eight (8) distribution substations out of the ten (10) communities were discovered during location-allocation analysis. Consequently, the pattern of distribution of the substations was found to be random but optimal and least cost. Hence, the result of this study will certainly make electricity distribution efficient in the study area and hence recommended for use by all stakeholders. KEY WORDS: Modelling, Location Allocation Analysis, GIS, Power Grid. ______________________________________________________________________________________________________ 1. -

Yobe State Multisectoral Crisis Recovery Project (Mcrp)
YOBE STATE MULTISECTORAL CRISIS RECOVERY PROJECT (MCRP) Environmental & Social Impact Assessment (ESIA) For Rehabilitation of 40km Gujba-Ngalda Road INFRASTRUCTURE PROJECTS UNDER COMPONENT 2 OF MCRP DRAFT REPORT MARCH, 2020 Yobe MCRP – Environmental & Social Impact Assessment (ESIA) for 40km Gujba-Ngalda Road Table of Contents List of Figures .................................................................................................. v List of Tables .................................................................................................. vi Acronyms and Abbreviations ............................................................................ vii Executive Summary ......................................................................................... ix CHAPTER ONE: INTRODUCTION ......................................................................... 2 1.1 Background ........................................................................................ 2 1.1.1 Technical Approach and Methodology to the ESIA ................................. 3 1.1.2 Desktop Research ......................................................................... 3 1.1.3 Reconnaissance Survey and Field Visits ........................................... 3 1.2 Applicable Laws and International Regulatory Framework ........................ 4 1.3 International Treaties and Conventions on Environment ........................... 6 1.5 Gender-Based Violence ........................................................................ 7 1.5.1 International -

Impacts of Boko Haram Insurgency on Agricultural Activities in Gujba Local Government Area, Yobe State, Nigeria
Research Publisher: Manuscript central Available Online at www.ijcrr.info International Journal of Contemporary Research and Review ISSN 0976 – 4852 https://doi.org/10.15520/ijcrr.v9i12.628 December, 2018|Volume 09|Issue 12| Section: Agriculture Impacts of Boko Haram Insurgency on Agricultural Activities in Gujba Local Government Area, Yobe State, Nigeria. M. Babagana1, M. Ismail2, B. G. Mohammed3, M. A. Dilala4, Hussaini I5, I M. Zangoma6 1Department of Animal Health and Production Technology College of Agriculture Gujba Yobe State, Nigeria 2Department of Agricultural Technology College of Agriculture Gujba Yobe State, Nigeria 3Department of Agricultural Technology College of Agriculture Gujba Yobe State, Nigeria 4Department of Animal Health and Production Technology College of Agriculture Gujba Yobe State, Nigeria 5Department of Agricultural Technology College of Agriculture Gujba Yobe State, Nigeria 6Department of Agricultural Technology College of Agriculture Gujba Yobe State, Nigeria Corresponding Author: M. Babagana Received: 2018-11-14; Accepted 2018-12-06, Abstract: The study was conducted between the months of November-December 2018 to assess the impacts of Boko Haram insurgency on agricultural activities in Gujba Local Government Area of Yobe state, Nigeria. Six towns namely Buni Yadi, Gujba, Goniri, Katarko, Mutai and Wagir formed the study locations. These towns were the major agricultural strongholds of the Local Government. The study considered impacts of the insurgency on farming after the return of residents to these towns after almost two years of exile in other places as a result of displacement by the militants’ activities (2016-2018). Descriptive Survey design involving mixed methods was used in which a total of 394 respondents participated. -

YOBE STATE MINISTRY of HEALTH Situation Report
YOBE STATE MINISTRY OF HEALTH Situation Report TITLE COVID-19 Pandemic Situation Report SERIAL NUMBER 17 EPID-WEEK 20 DATE 16 May 2020 HIGHLIGHTS: No new confirmed case(s) reported today Fifty-one (51) new contacts of the confirmed cases have been identified and line-listed by the contact tracing teams SMOH and WHO recruited, trained and deployed six (6) additional contact tracing teams in Gujba, Nguru, and Tarmuwa LGAs Seven (7) new alerts have been received and investigated in Nguru, Potiskum and Gujba LGAs Conducted high-level advocacy, led by the Hon Commissioner for Health (Vice-Chairman of State Task Force) and other members of State Rapid Response Team (SRRT), to Bade LGA emirate council to sensitize traditional leaders and community members on prevention of COVID-19 in their communities. EPIDEMIOLOGICAL SUMMARY: The total number of confirmed COVID-19 cases remains thirty-two (32): Sixteen (16) cases from Damaturu, eight (8) cases from Bade, five (5) cases from Nguru, and one (1) case each from Geidam, Tarmuwa, and Gujba LGAs Total confirmed cases of COVID-19 amongst Health Care Workers (HCWs) in the state remain nine (9): Six (6) nurses, two (2) doctors, and one (1) laboratory scientist Twenty-four (24) confirmed cases are on admission in isolation centers. All are in stable condition Three (3) cases have recovered and discharged from the isolation center two days ago The total number of contacts who completed the 14-days follow-up as of today is one hundred and twenty-four (124). None of them developed any symptoms The total number of deaths due to COVID-19 in the state is five (5) The total number of samples taken for testing remains sixty-three (63).