Raja / SOUTH SUDAN (M/F)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Map of South Sudan
UNITED NATIONS SOUTH SUDAN Geospatial 25°E 30°E 35°E Nyala Ed Renk Damazin Al-Fula Ed Da'ein Kadugli SUDAN Umm Barbit Kaka Paloich Ba 10°N h Junguls r Kodok Āsosa 10°N a Radom l-A Riangnom UPPER NILEBoing rab Abyei Fagwir Malakal Mayom Bentiu Abwong ^! War-Awar Daga Post Malek Kan S Wang ob Wun Rog Fangak at o Gossinga NORTHERN Aweil Kai Kigille Gogrial Nasser Raga BAHR-EL-GHAZAL WARRAP Gumbiel f a r a Waat Leer Z Kuacjok Akop Fathai z e Gambēla Adok r Madeir h UNITY a B Duk Fadiat Deim Zubeir Bisellia Bir Di Akobo WESTERN Wau ETHIOPIA Tonj Atum W JONGLEI BAHR-EL-GHAZAL Wakela h i te LAKES N Kongor CENTRAL Rafili ile Peper Bo River Post Jonglei Pibor Akelo Rumbek mo Akot Yirol Ukwaa O AFRICAN P i Lol b o Bor r Towot REPUBLIC Khogali Pap Boli Malek Mvolo Lowelli Jerbar ^! National capital Obo Tambura Amadi WESTERN Terakeka Administrative capital Li Yubu Lanya EASTERN Town, village EQUATORIAMadreggi o Airport Ezo EQUATORIA 5°N Maridi International boundary ^! Juba Lafon Kapoeta 5°N Undetermined boundary Yambio CENTRAL State (wilayah) boundary EQUATORIA Torit Abyei region Nagishot DEMOCRATIC Roue L. Turkana Main road (L. Rudolf) Railway REPUBLIC OF THE Kajo Yei Opari Lofusa 0 100 200km Keji KENYA o o o o o o o o o o o o o o o o o o o o o o o o o 0 50 100mi CONGO o e The boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. -
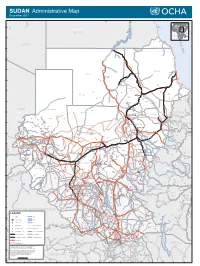
SUDAN Administrative Map December 2011
SUDAN Administrative Map December 2011 Faris IQLIT Ezbet Dush Ezbet Maks el-Qibli Ibrim DARAW KOM OMBO Al Hawwari Al-Kufrah Nagel-Gulab ASWAN At Tallab 24°N EGYPT 23°N R E LIBYA Halaib D S 22°N SUDAN ADMINISTRATED BY EGYPT Wadi Halfa E A b 'i Di d a i d a W 21°N 20°N Kho r A bu Sun t ut a RED SEA a b r A r o Porth Sudan NORTH Abu Hamad K Dongola Suakin ur Qirwid m i A ad 19°N W Bauda Karima Rauai Taris Tok ar e il Ehna N r e iv R RIVER NILE Ri ver Nile Desert De Bayouda Barbar Odwan 18°N Ed Debba K El Baraq Mib h o r Adara Wa B a r d a i Hashmet Atbara ka E Karora l Atateb Zalat Al Ma' M Idd Rakhami u Abu Tabari g a Balak d a Mahmimet m Ed Damer Barqa Gereis Mebaa Qawz Dar Al Humr Togar El Hosh Al Mahmia Alghiena Qalat Garatit Hishkib Afchewa Seilit Hasta Maya Diferaya Agra 17°N Anker alik M El Ishab El Hosh di El Madkurab Wa Mariet Umm Hishan Qalat Kwolala Shendi Nakfa a r a b t Maket A r a W w a o d H i i A d w a a Abdullah Islandti W b Kirteit m Afabet a NORTH DARFUR d CHAD a Zalat Wad Tandub ug M l E i W 16°N d Halhal Jimal Wad Bilal a a d W i A l H Aroma ERITREA Keren KHARTOUM a w a KASSALA d KHARTOUM Hagaz G Sebderat Bahia a Akordat s h Shegeg Karo Kassala Furawiya Wakhaim Surgi Bamina New Halfa Muzbat El Masid a m a g Barentu Kornoi u Malha Haikota F di Teseney Tina Um Baru El Mieiliq 15°N Wa Khashm El Girba Abu Quta Abu Ushar Tandubayah Miski Meheiriba EL GEZIRA Sigiba Rufa'ah Anka El Hasahisa Girgira NORTH KORDOFAN Ana Bagi Baashim/tina Dankud Lukka Kaidaba Falankei Abdel Shakur Um Sidir Wad Medani Sodiri Shuwak Badime Kulbus -

PRESS RELEASE Marina Modi Public &Media Relations Officer [email protected] 0955950026 #Defyhatenow: Mobilizing Civic A
PRESS RELEASE Marina Modi Public &Media relations Officer [email protected] 0955950026 #defyhatenow: Mobilizing Civic Action against Hate Speech and Directed Social Media Incitement to Violence in South Sudan. Juba, 03 November 2017 #DEFYHATENOW WIKIPEDIA WORKSHOP #defyhatenow initiative will be training students from the University of Juba on writing and feeding /editing information about South Sudan on Wikipedia,the online global encyclopedia from 6- 9 November 2017. Objectives; 1. Empowering South Sudanese to have a global voice in national narratives and knowledge in the quest for lasting peace. 2. Generating more knowledge about other people-to-people peace-building issues. 3. Initiate a sustainable movement of South Sudanese Wikipedia writers/editors. Why Wikipedia? South Sudan is underrepresented at Wikipedia, the world's largest online encyclopedia. There are hardly 1.500 articles about South Sudanese subjects and most of them are just stubs, since even entries about many major towns and states only feature a couple of lines. While Wikipedia is one of the most used and visited websites, next to no content about South Sudan has been generated inside the country itself. Instead, most information about South Sudan has been created by outsiders. With regard to internal peace-making, #defyhatenow will be working with the student run #kefkum initiative to collaboratively edit, starting with a critical review of Wunlit conference and then create a comprehensive article on Wikipedia. As a pilot example, #defyhatenow has already edited the Wikipedia article about Deim Zubeir from a one-line stub to a multi-facetted overview. Deim Zubeir has recently been included on South Sudan's first tentative list for UNESCO World Heritage sites. -

South Sudan - Crisis Fact Sheet #4, Fiscal Year (Fy) 2019 March 8, 2019
SOUTH SUDAN - CRISIS FACT SHEET #4, FISCAL YEAR (FY) 2019 MARCH 8, 2019 NUMBERS AT USAID/OFDA1 FUNDING HIGHLIGHTS A GLANCE BY SECTOR IN FY 2018 Insecurity in Yei results in unknown number of civilian deaths, prevents 15,000 5% 7% 20% people from receiving aid 7.1 million 7% Estimated People in South Health actors continue EVD awareness Sudan Requiring Humanitarian 10% and screening activities Assistance 19% 2019 Humanitarian Response Plan – WFP conducts first road delivery to 15% December 2018 central Unity 17% Logistics Support & Relief Commodities (20%) Water, Sanitation & Hygiene (19%) HUMANITARIAN FUNDING Health (17%) 6.5 million FOR THE SOUTH SUDAN RESPONSE Nutrition (15%) Estimated People in Need of Protection (10%) Food Assistance in South Sudan Agriculture & Food Security (7%) USAID/OFDA $135,187,409 IPC Technical Working Group – Humanitarian Coordination & Info Management (7%) February 2019 Shelter & Settlements (5%) USAID/FFP $398,226,647 3 State/PRM $91,553,826 1.9 million USAID/FFP2 FUNDING $624,967,8824 Estimated IDPs in BY MODALITY IN FY 2018 1% TOTAL USG HUMANITARIAN FUNDING FOR THE South Sudan SOUTH SUDAN CRISIS IN FY 2018 UN – January 31, 2019 84% 9% 5% U.S. In-Kind Food Aid (84%) 1% $3,756,094,855 Local & Regional Food Procurement (9%) TOTAL USG HUMANITARIAN FUNDING FOR THE Complementary Services (5%) SOUTH SUDAN RESPONSE IN FY 2014–2018, Cash Transfers for Food (1%) INCLUDING FUNDING FOR SOUTH SUDANESE 191,238 Food Vouchers (1%) REFUGEES IN NEIGHBORING COUNTRIES Estimated Individuals Seeking Refuge at UNMISS Bases UNMISS – March 4, 2019 KEY DEVELOPMENTS Ongoing violence between Government of the Republic of South Sudan (GoRSS) and opposition forces near Central Equatoria State’s Yei area has displaced an estimated 2.3 million 7,400 people to Yei town since December and is preventing relief agencies from reaching Estimated Refugees and Asylum more than 15,000 additional people seeking safety outside of Yei, the UN reports. -

Utd^L. Dean of the Graduate School Ev .•^C>V
THE FASHODA CRISIS: A SURVEY OF ANGLO-FRENCH IMPERIAL POLICY ON THE UPPER NILE QUESTION, 1882-1899 APPROVED: Graduate ttee: Majdr Prbfessor ~y /• Minor Professor lttee Member Committee Member irman of the Department/6f History J (7-ZZyUtd^L. Dean of the Graduate School eV .•^C>v Goode, James Hubbard, The Fashoda Crisis: A Survey of Anglo-French Imperial Policy on the Upper Nile Question, 1882-1899. Doctor of Philosophy (History), December, 1971, 235 pp., bibliography, 161 titles. Early and recent interpretations of imperialism and long-range expansionist policies of Britain and France during the period of so-called "new imperialism" after 1870 are examined as factors in the causes of the Fashoda Crisis of 1898-1899. British, French, and German diplomatic docu- ments, memoirs, eye-witness accounts, journals, letters, newspaper and journal articles, and secondary works form the basis of the study. Anglo-French rivalry for overseas territories is traced from the Age of Discovery to the British occupation of Egypt in 1882, the event which, more than any other, triggered the opening up of Africa by Europeans. The British intention to build a railroad and an empire from Cairo to Capetown and the French dream of drawing a line of authority from the mouth of the Congo River to Djibouti, on the Red Sea, for Tied a huge cross of European imperialism over the African continent, The point of intersection was the mud-hut village of Fashoda on the left bank of the White Nile south of Khartoum. The. Fashoda meeting, on September 19, 1898, of Captain Jean-Baptiste Marchand, representing France, and General Sir Herbert Kitchener, representing Britain and Egypt, touched off an international crisis, almost resulting in global war. -

Everyone and Everything Is a Target
THE IMPACT ON CHILDREN OF ATTACKS ON HEALTH CARE AND DENIAL OF HUMANITARIAN ACCESS IN SOUTH SUDAN “Everyone and Everything Is a Target” About Watchlist Watchlist on Children and Armed Conflict (“Watchlist”) strives to end violations against children in armed conflicts and to guarantee their rights. As a global network, Watchlist builds partnerships among local, national, and international nongovernmental organizations (NGOs), enhancing mutual capacities and strengths. Working together, we collect and disseminate information on violations against children in conflicts in order to influence key decision-makers and implement programs and policies that effectively protect children. For further information about Watchlist, please contact: [email protected] or visit: www.watchlist.org This report was researched and written by Christine Monaghan, PhD, with support from Bonnie Berry, Adrianne Lapar, and Cara Antonaccio. Vesna Jaksic Lowe copyedited the report. Watchlist would also like to thank the many domestic and international NGOs, UN agencies, and individuals who participated in the research, generously shared their stories and experiences, and provided feedback on the report. “Everyone and Everything Is a Target” THE IMPACT ON CHILDREN OF ATTACKS ON HEALTH CARE AND DENIAL OF HUMANITARIAN ACCESS IN SOUTH SUDAN Table of Contents Map of South Sudan 2 Acronyms 3 Executive Summary and Recommendations 4 Methodology 10 Conflict Context 11 Pre-2016 Health Context 13 Health Context during the Reporting Period 14 Compounding Health Challenges due to Attacks and Denial of Humanitarian Access 16 Focus Regions 20 a. Greater Upper Nile 20 b. Bahr el Ghazal 25 c. Equatoria 27 Conclusion 32 Endnotes 33 D 24° 26° 28° 30° 32 34 in 36° ° ° de En Nahud r 12° Abu Zabad SOUTH 12° SOUTH SUDAN Ed Damazin SUDAN SUDAN Al Fula Renk Ed Da'ein Tullus Nuba Mts. -

E4220v2 Republic of South Sudan Ministry of Agriculture & Forestry
E4220v2 Republic of South Sudan Ministry of Agriculture & Forestry Public Disclosure Authorized EMERGENCY FOOD CRISIS RESPONSE PROJECT Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized ENVIRONMENTAL AND SOCIAL ASSESSMENT REPORT May 2013 Contents LIST OF ACRONYMS AND ABBREVIATIONS III EXECUTIVE SUMMARY 1 ACKNOWLEDGEMENTS 4 1. BACKGROUND INFORMATION ON THE PROJECT AND THE STUDY 5 2. AN OVERVIEW OF THE AGRICULTURE SECTOR IN SOUTH SUDAN 14 3. REVIEW OF THE RELEVANT POLICIES, LAWS AND REGULATIONS 19 4. DESCRIPTION OF THE PROJECT ACTIVITIES AND IMPLEMENTATION APPROACH 26 6. PUBLIC CONSULTATIONS AND DISCLOSURE 48 7. PEST MANAGEMENT 52 8. ENVIRONMENTAL AND SOCIAL ISSUES, IMPACTS AND MITIGATION 55 9. ENVIRONMENT AND SOCIAL MANAGEMENT AND MONITORING PLAN 60 10. SUMMARY OF THE STUDY 66 11. REFERENCES 69 ii LIST OF ACRONYMS AND ABBREVIATIONS AAHI Action Africa Help International CES Central Equatoria State CPA Comprehensive Peace Agreement EA Environmental Assessment EFCRP Emergency Food Crisis and Response Project ESA Environmental and Social Assessment ESAF Environment and Social Assessment Framework ESIA Environmental and Social Impact Assessment ESMF Environment and Social Management Framework ESMP Environment and Social Management Plan FAO Food and Agriculture Organization GDP Gross Domestic Product GFRP Global Food Crisis Response Program GNI Gross National Income GoSS Government of Southern Sudan IPM Integrated Pest Management IPMF Integrated Pest Management Framework IPMP Integrated Peoples Management -

Download (PDF, 1.15
South Sudan HUMANITARIAN-SUPPORTED IDP RETURNS June 2021 Since April 2016, internally displaced persons (IDP) have been approaching UNHCR’s protection desks in dierent internally displaced sites, in search for information in their places of origin or requesting assistance to return to their area of origin. Working through the area-based Solutions Working Groups, humanitarians and UNMISS, follow a comprehen- sive set of guidelines so that each IDP has the information needed to make a sound and informed decision, voluntarily. This begins a rigorous process of interviews, counselling, and protection assessments to ensure returns are in safe, digni- fied, and durable. After returning to their area of origin or habitual residence, the Solutions Working Groups continue monitoring their reintegration into the community June Highlights No supported returns in the month of May and June Final destinations (State) due to the onset of the rain season. Upper Nile 10,919 (58%) Unity 5,326 (28%) Top five final destinations (County) individuals Returnees by departure 18,690 point WBG 1,828 (10%) Baliet 7,859 (42%) 13 (0.1%) 6,169 households Jonglei 562 (4%) in PoCs BalietMaban 7,536 (40%) Western Equatoria 29 ( ~0.16%) Cumulative Supported Returns Wau 1,663 (9%) (September 2018 to June 2021) Central Equatoria 19 (~0.09%) Rubkona 724 (4%) 18,677 (99.9%) in Settlements Lakes 10 (~0 .05%) Akobo 280 (2%) Spontaneous and supported return movements (number of Individuals movements) From Maban IDP site to: Maban communities (7,536) individuals From Melut IDP site -
Sudan Country Report
SUDAN COUNTRY REPORT April 2004 Country Information & Policy Unit IMMIGRATION AND NATIONALITY DIRECTORATE HOME OFFICE, UNITED KINGDOM Sudan April 2004 CONTENTS 1. SCOPE OF DOCUMENT 1.1 - 1.7 2. GEOGRAPHY 2.1 - 2.3 3. ECONOMY 3.1 - 3.2 4. HISTORY 1989 - April 2004: The al-Bashir Regime 4.1 - 4.3 Events of 2002 - 2004 4.4 - 4.19 5. STATE STRUCTURES The Constitution 5.1 - 5.2 The Political System 5.3 - 5.5 Political Parties 5.6 - 5.7 The Judiciary 5.8 - 5.17 Military Service and the Popular Defence Force 5.18 - 5.26 Conscription 5.27 - 5.32 Exemptions, Pardons and Postponements 5.33 - 5.36 Internal Security 5.37 - 5.38 Legal Rights/Detention 5.39 - 5.43 Prisons and Prison Conditions 5.44 - 5.47 Medical Services 5.48 - 5.55 HIV/AIDS 5.56 - 5.60 Mental Health Care 5.61 - 5.62 The Education System 5.63 - 5.64 Sudanese Nationality Laws 5.65 - 5.68 6. HUMAN RIGHTS 6.A. HUMAN RIGHTS ISSUES Overview 6.1 - 6.12 Freedom of Speech and the Media 6.13 - 6.17 Newspapers 6.18 - 6.21 Television, Radio and the Internet 6.22 - 6.24 Freedom of Religion 6.25 - 6.37 Forced Religious Conversion 6.38 - 6.39 Freedom of Assembly and Association 6.40 - 6.46 Meetings and Demonstrations 6.47 - 6.49 Employment Rights 6.50 - 6.52 Trade Unions 6.53 - 6.58 Wages and Conditions 6.59 - 6.62 People Trafficking 6.63 - 6.66 Slavery 6.67 - 6.71 Freedom of Movement 6.72 - 6.75 Passports 6.76 - 6.77 Exit Visas 6.78 - 6.81 Airport Security 6.82 - 6.83 Returning Sudanese Nationals 6.84 - 6.87 Arbitrary Interference with Privacy 6.88 - 6.91 6.B. -

South Sudan: Hospitals and Cemonc Targeted for Scaling up of Blood Transfusion Services, 2017 South Sudan
South Sudan: Hospitals and CEmONC targeted for scaling up of blood transfusion services, 2017 South Sudan Map date: 29 May 2018 Sudan Chad Renk Northern Upper Nile Palog Fashoda Maban Ruweng Malakal Aweil East Bentui Malual Kop Central T MayenTwic AbunTuralei Upper Nile Lol Northern Maiwut Wanjok IAL Liech Latjor Gogrial Raga Aweil Aweil Center Fangak Deim Zubeir Southern Ethiopia Tonj Liech Bieh Akobo Cuei Cok Wau Wau Ngok Eastern Lake Aduel Jonglei Boma Eastern Lake Tambura Bor South Central African Republic Terekeka Maridi Mary Help Legend Gbudwe Amadxi Kapoeta National Blood Transfusion Service (NBTS) HQ Imatong I Kapoeta Mission Regional Blood Trasnfusion Service (RBTS) NBTS HQ Yambio Jubek Juba Hub Blood Transfusion Services (HBTS) Torit State Hospital Blood Trransfusion Centers (STBC) Democr a tic Yei River Republic of Kenya CEmOC/Hospital Blood Banks (HBB) the Congo 0 100 200 Uganda km The boundaries and names shown and the designations used on this map do not imply the expression The map reflects the currently available data and is subject to change according to further updates to the data. of any opinion whatsoever on the part of the World Health Organization concerning the legal status Data source: South Sudan Ministry of Health, World Health Organization (WHO), OpenStreetMap of any country, territory, city or area or of its authorities, or concerning the delimitation of its Map production: WHO Health Emergencies Programme frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.. -
Southern Sudan at Odds with Itself
Allen et al. Schomerus ‘I found the report fascinating and also disturbing in equal measure. …While state building efforts are rightly focused on building up structures from the ground they fail to address the primary need to ensure that such institutions are properly reformed to become independent and impartial institutions…To address these pressing issues and to maximise the positive momentum generated SOUTHERN ODD SUDAN AT from the elections and the international focus on Southern Sudan at this time, these issues needs to be discussed publicly with all key states, governments and civil society stakeholders who hold the future of Southern Sudan in their hands. I would urge action sooner rather than later.’ Akbar Khan, Director, Legal & Constitutional Affairs Division, Commonwealth Secretariat ‘The great strength of the report is the accuracy of its voicing of common concerns – it forms an excellent representation of people’s perceptions and experiences, making an important corollary to the current focus on high-level political negotiations and structures. As the report emphasises at the outset, the current focus of Sudanese governments and their international advisors on the technicalities and procedural aspects of planning for the referendum and its outcome needs to be countered by the more holistic approach advocated by this report.’ Cherry Leonardi, Durham University ‘A very important and timely contribution to the current debates…The report offers an invaluable S insight in some of the key issues and dilemma’s Southern Sudan and -

South Sudan's Bright Economic Prospects
Maximum The difference A South between Sudanese impact population movie from UK’s control and family star in the planning making? aid Page 8 Page 32 Page 44 The MarchPIONEER 19, 2011 - March 25, 2011Issue 11 Vol 002 5 SDG 2 USD South Sudan’s bright economic prospects- World Bank Otieno Ogeda ith less than four months to indepen- dence of SouthW Sudan, analysts fore- see speedy economic growth of a region that has been coupled with confl ict for many years. World Bank reveals that the region’s economic growth would surprise many people by the massive ex- pectations coated with hard work and willingness to set stronger institutions. “South Sudan is start- ing on a new page with enormous experiences from other States which if well placed would catalyse both socio-economic and political growth,” asserts Shantayan- an Devarajan, World Bank’s African Chief Economist. On his three day visit to South Sudan, Shantayanan says that the commitment the citizens have shown towards the Government of Southern Sudan should be turned into a reality following the tremendous referendum vote that saw Southerners vote a world referendum record of over 98 percent. South Sudan celebrates its fi rst independence on July 9 after voting over- Full story on page 2 Leading woman SPLM economic An interview with the The role of Southern Sudan journalist dies in blueprint ahead of Minister of Higher Human Rights Commission accident page 3 independence page 4 Education page 6 explained page 15 2 The Pioneer / March 19, 2011 - March 25, 2011 National News South Sudan’s bright economic prospects- World Bank Continued from page 1 izens had always anticipated.