An Overview on Non Epileptic Seizures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Abuse-Proof Solid Pharmaceutical Composition
(19) TZZ¥¥ ¥_T (11) EP 3 329 939 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 06.06.2018 Bulletin 2018/23 A61K 47/02 (2006.01) A61K 47/36 (2006.01) A61K 9/16 (2006.01) A61K 31/485 (2006.01) (2006.01) (21) Application number: 17204525.4 A61K 31/192 (22) Date of filing: 29.11.2017 (84) Designated Contracting States: (72) Inventors: AL AT BE BG CH CY CZ DE DK EE ES FI FR GB • BOSCHETTI, Silvia GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO I-38060 Aldeno (TN) (IT) PL PT RO RS SE SI SK SM TR • ROSSI, Massimiliano Designated Extension States: I-38121 Trento (IT) BA ME • BENFENATI, Diego Designated Validation States: I-38052 Caldonazzo (TN) (IT) MA MD • POJER, Alessandro I-38092 Altavalle (TN) (IT) (30) Priority: 02.12.2016 IT 201600122469 (74) Representative: Allaix, Roberto (71) Applicant: E-Pharma Trento S.p.A. PGA S.p.A. 38123 Trento (IT) Via Mascheroni, 31 20145 Milano (IT) (54) ABUSE-PROOF SOLID PHARMACEUTICAL COMPOSITION (57) The present invention relates to an abuse-proof solid pharmaceutical composition comprising an active ingre- dient with potential for abuse, silica in an amount of from 10 mg to 1000 mg, guar flour in an amount of from 100 mg to 300 mg, and a water soluble diluent in an amount of from 500 mg to 5000 mg. EP 3 329 939 A1 Printed by Jouve, 75001 PARIS (FR) EP 3 329 939 A1 Description FIELD OF THE INVENTION 5 [0001] The present invention relates to an abuse-proof solid pharmaceutical composition, in particular a solid phar- maceutical composition, such as, for example a granulate or a tablet, capable of solubilizing in a glass of water (about 100 ml), but of forming a not injectable gel and/or viscous solution if added to the amount of water contained in a hypodermic syringe (about 10 ml). -

Pharmacology on Your Palms CLASSIFICATION of the DRUGS
Pharmacology on your palms CLASSIFICATION OF THE DRUGS DRUGS FROM DRUGS AFFECTING THE ORGANS CHEMOTHERAPEUTIC DIFFERENT DRUGS AFFECTING THE NERVOUS SYSTEM AND TISSUES DRUGS PHARMACOLOGICAL GROUPS Drugs affecting peripheral Antitumor drugs Drugs affecting the cardiovascular Antimicrobial, antiviral, Drugs affecting the nervous system Antiallergic drugs system antiparasitic drugs central nervous system Drugs affecting the sensory Antidotes nerve endings Cardiac glycosides Antibiotics CNS DEPRESSANTS (AFFECTING THE Antihypertensive drugs Sulfonamides Analgesics (opioid, AFFERENT INNERVATION) Antianginal drugs Antituberculous drugs analgesics-antipyretics, Antiarrhythmic drugs Antihelminthic drugs NSAIDs) Local anaesthetics Antihyperlipidemic drugs Antifungal drugs Sedative and hypnotic Coating drugs Spasmolytics Antiviral drugs drugs Adsorbents Drugs affecting the excretory system Antimalarial drugs Tranquilizers Astringents Diuretics Antisyphilitic drugs Neuroleptics Expectorants Drugs affecting the hemopoietic system Antiseptics Anticonvulsants Irritant drugs Drugs affecting blood coagulation Disinfectants Antiparkinsonian drugs Drugs affecting peripheral Drugs affecting erythro- and leukopoiesis General anaesthetics neurotransmitter processes Drugs affecting the digestive system CNS STIMULANTS (AFFECTING THE Anorectic drugs Psychomotor stimulants EFFERENT PART OF THE Bitter stuffs. Drugs for replacement therapy Analeptics NERVOUS SYSTEM) Antiacid drugs Antidepressants Direct-acting-cholinomimetics Antiulcer drugs Nootropics (Cognitive -

Workbook Psychiatry and Narcology
Kharkiv National Medical University Department of Psychiatry, Narcology and Medical Psychology WORKBOOK MANUAL FOR INDIVIDUAL WORK FOR MEDICAL STUDENTS PSYCHIATRY AND NARCOLOGY (Part 2) Student ___________________________________________________________ Faculty _________________________________________________________ Course _________________ Group _____________________________________ Kharkiv 2019 Затверджено вченою радою ХНМУ Протокол №5 від 23.05.2019 р. Psychiatry (Part 2) : workbook manual for individual work of students / I. Strelnikova, G. Samardacova, К. Zelenska – Kharkiv, 2019. – 103 p. Копіювання для розповсюдження в будь-якому вигляді частин або повністю можливо тільки з дозволу авторів навчального посібника. CLASS 7. NEUROTIC DISORDERS. CLINICAL FORMS. TREATMENT AND REHABILITATION. POSTTRAUMATIC STRESS DISORDER. TREATMENT AND REHABILITATION. Psychogenic diseases are a large and clinically varied group of diseases resulting from an effect of acute or long-term psychic traumas, which manifest themselves by both mental and somatoneurological disorders and, as a rule, are reversible. Psychogenic diseases are caused by a psychic trauma, i.e. some events which affect significant aspects of existence of the human being and result in deep psychological feelings. These may be subjectively significant events, i.e. those which are pathogenic for the majority of people. Besides, the psyche may be traumatized by conventionally pathogenic events, which cause feelings in an individual because of his peculiar hierarchy of values. Unfavorable psychogenic effects on the human being cause stress in him, i.e. a nonspecific reaction at the physiological, psychological and behavioural levels. Stress may exert some positive, mobilizing influence, but may result in disorganization of the organism activity. The stress, which exerts a negative influence and causes various disturbances and even diseases, is termed distress. Classification of neurotic disorders I. -
![Ehealth DSI [Ehdsi V2.2.2-OR] Ehealth DSI – Master Value Set](https://docslib.b-cdn.net/cover/8870/ehealth-dsi-ehdsi-v2-2-2-or-ehealth-dsi-master-value-set-1028870.webp)
Ehealth DSI [Ehdsi V2.2.2-OR] Ehealth DSI – Master Value Set
MTC eHealth DSI [eHDSI v2.2.2-OR] eHealth DSI – Master Value Set Catalogue Responsible : eHDSI Solution Provider PublishDate : Wed Nov 08 16:16:10 CET 2017 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 1 of 490 MTC Table of Contents epSOSActiveIngredient 4 epSOSAdministrativeGender 148 epSOSAdverseEventType 149 epSOSAllergenNoDrugs 150 epSOSBloodGroup 155 epSOSBloodPressure 156 epSOSCodeNoMedication 157 epSOSCodeProb 158 epSOSConfidentiality 159 epSOSCountry 160 epSOSDisplayLabel 167 epSOSDocumentCode 170 epSOSDoseForm 171 epSOSHealthcareProfessionalRoles 184 epSOSIllnessesandDisorders 186 epSOSLanguage 448 epSOSMedicalDevices 458 epSOSNullFavor 461 epSOSPackage 462 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 2 of 490 MTC epSOSPersonalRelationship 464 epSOSPregnancyInformation 466 epSOSProcedures 467 epSOSReactionAllergy 470 epSOSResolutionOutcome 472 epSOSRoleClass 473 epSOSRouteofAdministration 474 epSOSSections 477 epSOSSeverity 478 epSOSSocialHistory 479 epSOSStatusCode 480 epSOSSubstitutionCode 481 epSOSTelecomAddress 482 epSOSTimingEvent 483 epSOSUnits 484 epSOSUnknownInformation 487 epSOSVaccine 488 © eHealth DSI eHDSI Solution Provider v2.2.2-OR Wed Nov 08 16:16:10 CET 2017 Page 3 of 490 MTC epSOSActiveIngredient epSOSActiveIngredient Value Set ID 1.3.6.1.4.1.12559.11.10.1.3.1.42.24 TRANSLATIONS Code System ID Code System Version Concept Code Description (FSN) 2.16.840.1.113883.6.73 2017-01 A ALIMENTARY TRACT AND METABOLISM 2.16.840.1.113883.6.73 2017-01 -

WHO Drug Information Vol
WHO Drug Information Vol. 26, No. 4, 2012 WHO Drug Information Contents International Regulatory Regulatory Action and News Harmonization New task force for antibacterial International Conference of Drug drug development 383 Regulatory Authorities 339 NIBSC: new MHRA centre 383 Quality of medicines in a globalized New Pakistan drug regulatory world: focus on active pharma- authority 384 ceutical ingredients. Pre-ICDRA EU clinical trial regulation: public meeting 352 consultation 384 Pegloticase approved for chronic tophaceous gout 385 WHO Programme on Tofacitinib: approved for rheumatoid International Drug Monitoring arthritis 385 Global challenges in medicines Rivaroxaban: extended indication safety 362 approved for blood clotting 385 Omacetaxine mepesuccinate: Safety and Efficacy Issues approved for chronic myelo- Dalfampridine: risk of seizure 371 genous leukaemia 386 Sildenafil: not for pulmonary hyper- Perampanel: approved for partial tension in children 371 onset seizures 386 Interaction: proton pump inhibitors Regorafenib: approved for colorectal and methotrexate 371 cancer 386 Fingolimod: cardiovascular Teriflunomide: approved for multiple monitoring 372 sclerosis 387 Pramipexole: risk of heart failure 372 Ocriplasmin: approved for vitreo- Lyme disease test kits: limitations 373 macular adhesion 387 Anti-androgens: hepatotoxicity 374 Florbetapir 18F: approved for Agomelatine: hepatotoxicity and neuritic plaque density imaging 387 liver failure 375 Insulin degludec: approved for Hypotonic saline in children: fatal diabetes mellitus -

BMJ Open Is Committed to Open Peer Review. As Part of This Commitment We Make the Peer Review History of Every Article We Publish Publicly Available
BMJ Open is committed to open peer review. As part of this commitment we make the peer review history of every article we publish publicly available. When an article is published we post the peer reviewers’ comments and the authors’ responses online. We also post the versions of the paper that were used during peer review. These are the versions that the peer review comments apply to. The versions of the paper that follow are the versions that were submitted during the peer review process. They are not the versions of record or the final published versions. They should not be cited or distributed as the published version of this manuscript. BMJ Open is an open access journal and the full, final, typeset and author-corrected version of record of the manuscript is available on our site with no access controls, subscription charges or pay-per-view fees (http://bmjopen.bmj.com). If you have any questions on BMJ Open’s open peer review process please email [email protected] BMJ Open Pediatric drug utilization in the Western Pacific region: Australia, Japan, South Korea, Hong Kong and Taiwan Journal: BMJ Open ManuscriptFor ID peerbmjopen-2019-032426 review only Article Type: Research Date Submitted by the 27-Jun-2019 Author: Complete List of Authors: Brauer, Ruth; University College London, Research Department of Practice and Policy, School of Pharmacy Wong, Ian; University College London, Research Department of Practice and Policy, School of Pharmacy; University of Hong Kong, Centre for Safe Medication Practice and Research, Department -

Farmaatsia- Terminoloogia Teine, Täiendatud Trükk
Farmaatsia- terminoloogia Teine, täiendatud trükk Graanulid Suspensioon Lahus Emulsioon Pillid Pulber Salv Kreem Aerosool Plaaster Sprei Pastill Tampoon Oblaat Emulsioon Kontsentraat Silmageel Tablett Haavapulk Ninatilgad Kapsel Lakukivi Inhalaator Farmaatsia- terminoloogia Teine, täiendatud trükk Tartu 2019 Koostajad: Toivo Hinrikus, Karin Kogermann, Ott Laius, Signe Leito, Ain Raal, Andres Soosaar, Triin Teppor, Daisy Volmer Keeletoimetaja: Tiina Kuusk Kirjastanud: Ravimiamet Nooruse 1, 50411 Tartu Telefon: +372 737 4140 Faks: +372 737 4142 E-post: [email protected] Esimene trükk 2010 Teine, täiendatud trükk 2019 Raamat on leitav Ravimiameti veebilehelt: www.ravimiamet.ee/farmaatsiaterminoloogia Väljaande refereerimisel või tsiteerimisel palume viidata allikale. ISBN 978-9949-9697-3-9 Sisukord Farmaatsiaterminoloogia Eestis..........................................................................................5 Üldised farmaatsiaalased terminid ...................................................................................10 Euroopa farmakopöa ......................................................................................................... 21 Euroopa farmakopöa sõnastik ..........................................................................................24 Standardterminid ..............................................................................................................29 Ravimvormid .....................................................................................................................29 -
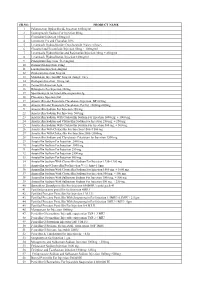
SR.NO. PRODUCT NAME 1 Palonosetron Hydrochloride
SR.NO. PRODUCT NAME 1 Palonosetron Hydrochloride Injection 0.05mg/ml 2 Esomeprazole Sodium For Injection 40mg 3 Cimetidine Injection 100mg/ml 4 Ivermectin 1% and Clorsulon 10% 5 Levamisole Hydrochloride+Oxyclozanide 3%w/v+6%w/v 6 Closantel and Levamisole Injection 50mg + 100mg/ml 7 Levamisole Hydrochloride and Rafoxanide Injection 30mg + 45mg/ml 8 Levamisole Hydrochloride Injection 100mg/ml 9 Praziquantel Injection 56.8 mg/ml 10 Doramectin Injection 10mg 11 Lorazepam Injection 4mg/ml 12 Diazepam Injection 5mg/ml 13 Midazolam Injection BP 5mg/ml (Single Use) 14 Diazepam Injection 10 mg./ml. 15 Temocillin Injection 1gm 16 Rifampicin For Injection 300mg 17 Spectinomycin for Injectable suspension 2g 18 Placentrex Injection 2ml 19 Amoxicillin and Potassium Clavulanate Injection BP 625mg 20 Amoxicillin and Potassium Clavulanate For Inj. 1000mg+200mg 21 Amoxicillin Sodium For Injection 250 mg. 22 Amoxicillin Sodium For Injection 500 mg. 23 Amoxicillin Sodium With Cloxacillin Sodium For Injection 1000 mg. + 1000 mg. 24 Amoxicillin Sodium and Cloxacillin Sodium For Injection 250 mg. + 250 mg. 25 Amoxicillin Sodium With Cloxacillin Sodium For Injection 500 mg. + 500 mg. 26 Amoxicillin With Cloxacillin For Injection 1500+1500 mg 27 Amoxicillin With Cloxacillin For Injection 2000+2000mg 28 Amoxicillin Sodium and Clavulanate Potassium for Injection 1200 mg 29 Ampicillin Sodium For Injection 2000 mg. 30 Ampicillin Sodium For Injection 3000 mg. 31 Ampicillin Sodium For Injection 250 mg. 32 Ampicillin Sodium For Injection 2500 mg. 33 Ampicillin Sodium For Injection 500 mg. 34 Ampicillin Sodium With Cloxacillin Sodium For Injection 1250+1250 mg 35 Ampicillin and Cloxacillin For Injection Vet 1.5gm+1.5gm 36 Ampicillin Sodium With Cloxacillin Sodium For Injection 1000 mg. -

Mexidol® Action
Mexidol has antioxidant, antihypoxic and membrane-protective Mexidol® action. It inhibits lipid peroxidation, increases the activity of superoxide dismutase, increases the lipid-protein ratio, reduces International Non-Proprietary Name (INN): Mexidol the viscosity of the membrane and increases its fluidity. The drug (Emoxypine) modulates the activity of membrane-bound enzymes (calcium of independent phosphodiesterase, adenylate cyclase and Dosage Form: pills (125 mg) acetylcholinesterase) and receptor complexes (benzodiazepine, Structure: 1 capsule contains: GABA and acetylcholine): it enhances their ability to bind to Active ingredient: ethylmethylhydroxypyridine succinate (2-ethyl- ligands, helps to preserve the structural and functional 6-methyl-3-hydroxypyridine) – 125 mg. organization of biomembranes and neurotransmitter transport, Excipients: lactose monohydrate – 97.5 mg, povidone – 25 mg, and facilitates synaptic transmission improvement. magnesium stearate – 2.5 mg. Mexidol causes an increase of dopamine in the brain. It Film coat: opadrai II white 33G28435 – 7.5 mg (hypromellose 3 enhances compensatory activation of aerobic glycolysis and mg, titanium dioxide – 1.875 mg, lactose monohydrate – 1.575 weakens the inhibition of oxidative processes in the Krebs cycle mg, polyethylene glycol (macrogol) – 0.6 mg, triacetin – 0.45 mg) under conditions of hypoxia with an increased ATP and creatine phosphate. The drug activates the energy-synthesizing functions Description: of mitochondria and stabilization of cell membranes. The double radius pills are covered with a film coat in white or Mexidol improves the metabolism and blood supply of the brain, light creamy colour. On the cross-section there are two layers: improves microcirculation and rheological properties of blood, the inner one (the core) is gray or gray-creamy and the outer one and reduces platelet aggregation. -

Zāļu Patēriņa Statistika 2018
fa ZĀĻU PATĒRIŅA STATISTIKA STATISTICS ON MEDICINES CONSUMPTION 2018 ZĀĻU VALSTS AĢENTŪRA STATE AGENCY OF MEDICINES 2019 Autors/ Author: Zāļu valsts aģentūra Sagatavoja/ Prepared by: A. Seilis, E. Gailīte Izdevējs/ Publisher: Zāļu valsts aģentūra/ State Agency of Medicines© 2019 Izmantojot šajā grāmatā publicētos datus, jānorāda datu avots When using or quoting the data included in this issue, please indicate the source SATURS Ievads .................................................................................................................................................................................................. 6 Metode ............................................................................................................................................................................................... 7 Rezultāti .............................................................................................................................................................................................. 9 1. Iedzīvotāju skaits Latvijā no 2014. līdz 2018. gadam ................................................................................................................... 9 2. Licencēto zāļu lieltirgotavu skaits ................................................................................................................................................ 9 3. Reģistrēto zāļu kopējais apgrozījums pēdējos 5 gados .............................................................................................................. -

ADAPTOL Summary of Product Characteristics
TRANSLATION FROM LATVIAN State Agency of Medicines, Director I.Adovi ča __ /signature/__ Registered No. 10843-300708 Summary of Product Characteristics 1. NAME OF THE MEDICINAL PRODUCT ADAPTOL ® 300 mg Tablets ADAPTOL ® 500 mg Tabletes ADAPTOL ® 300 mg Capsules 2. QUALITATIVE AND QUANTITATIVE COMPOSITION OF THE PRODUCT Active substance : mebicar (Mebicarum) – well known name. Each ADAPTOL ® 300 mg tablet contains 300 mg mebicar. Each ADAPTOL ® 500 mg tablet contains 500 mg mebicar. Each ADAPTOL ® 300 mg capsule contains 300 mg mebicar Excipients : the complete list of excipients see in p. 6.1 3. PHARMACEUTICAL FORM Tablets. Description : White or almost white, round flat tablets with bevelled edge and break line on one side of the tablet. Capsules. Description : gelatine capsules No. 0 filled with white or almost white granules. 4. CLINICAL DESCRIPTION 4.1. Indications Neuroses and neurotic disturbances (irritability, emotional excitability, anxiety, fear). Cardialgias of different genesis, which are not connected with ischemic heart disease. To improve tolerability of neuroleptics and tranquilizers. Complex therapy to decrease addiction to smoking. 4.2 Administration and dosage The drugs are administered orally independently of meals. Adults use 300-500 mg 2-3 times a day. The highest single dose is 3 g, the highest daily dose - 10 g. The course of treatment - from a few days up to 2-3 months. Complex therapy to decrease the addiction to smoking – 600-1000 mg a day for 5-6 weeks. Elderly should not adjust the dose. Patients with liver impairment should not diminish the dose. Dose adjustment is not studied in patients with kidneys deficiency . -

WO 2017/120012 Al 13 July 20 17 (13.07.2017) W P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2017/120012 Al 13 July 20 17 (13.07.2017) W P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/185 (2006.01) A61K 31/336 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DJ, DK, DM, PCT/US20 16/067024 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KH, KN, 15 December 2016 (15. 12.2016) KP, KR, KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, (25) Filing Language: English NI, NO, NZ, OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, (26) Publication Language: English RU, RW, SA, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, (30) Priority Data: ZA, ZM, ZW. 62/275,182 5 January 2016 (05.01 .2016) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: THE REGENTS OF THE UNIVERSITY kind of regional protection available): ARIPO (BW, GH, OF CALIFORNIA [US/US]; 1111 Franklin Street, 12th GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, Floor, Oakland, California 94607-5200 (US).