Psychiatry and Narcology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
LINKING INFECTIOUS and NARCOLOGY CARE) Evidence-Based for Engagement in HIV Care
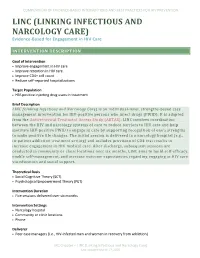
COMPENDIUM OF EVIDENCE-BASED INTERVENTIONS AND BEST PRACTICES FOR HIV PREVENTION LINC (LINKING INFECTIOUS AND NARCOLOGY CARE) Evidence-Based for Engagement in HIV Care INTERVENTION DESCRIPTION Goal of Intervention • Improve engagement in HIV care • Improve retention in HIV care • Improve CD4+ cell count • Reduce self-reported hospitalizations Target Population • HIV-positive injecting drug users in treatment Brief Description LINC (Linking Infectious and Narcology Care) is an individual-level, strengths-based case management intervention for HIV-positive persons who inject drugs (PWID). It is adapted from the Antiretroviral Treatment Access Study (ARTAS). LINC involves coordination between the HIV and narcology systems of care to reduce barriers to HIV care and help motivate HIV-positive PWID to engage in care by supporting recognition of one’s strengths to make positive life changes. The initial session is delivered in a narcology hospital (e.g., in-patient addiction treatment setting) and includes provision of CD4 test results to increase engagement in HIV medical care. After discharge, subsequent sessions are conducted in community or clinic locations over six months. LINC aims to build self-efficacy, enable self-management, and increase outcome expectancies regarding engaging in HIV care via education and social support. Theoretical Basis • Social Cognitive Theory (SCT) • Psychological Empowerment Theory (PET) Intervention Duration • Five sessions delivered over six months Intervention Settings • Narcology hospital • Community or clinic locations • Phone Deliverer • Peer case managers (i.e., HIV-infected men and women in recovery from addiction) LRC Chapter – LINC (Linking Infectious and Narcology Care) Last updated March 17, 2020 COMPENDIUM OF EVIDENCE-BASED INTERVENTIONS AND BEST PRACTICES FOR HIV PREVENTION Delivery Methods • Case management • Printed materials • Discussion • Video • Goal setting Structural Components There are no reported structural components reported for this study. -

Autism Practice Parameters
American Academy of Child and Adolescent Psychiatry AACAP is pleased to offer Practice Parameters as soon as they are approved by the AACAP Council, but prior to their publication in the Journal of the American Academy of Child and Adolescent Psychiatry (JAACAP). This article may be revised during the JAACAP copyediting, author query, and proof reading processes. Any final changes in the document will be made at the time of print publication and will be reflected in the final electronic version of the Practice Parameter. AACAP and JAACAP, and its respective employees, are not responsible or liable for the use of any such inaccurate or misleading data, opinion, or information contained in this iteration of this Practice Parameter. PRACTICE PARAMETER FOR THE ASSESSMENT AND TREATMENT OF CHILDREN AND ADOLESCENTS WITH AUTISM SPECTRUM DISORDER ABSTRACT Autism spectrum disorder (ASD) is characterized by patterns of delay and deviance in the development of social, communicative, and cognitive skills which arise in the first years of life. Although frequently associated with intellectual disability, this condition is distinctive in terms of its course, impact, and treatment. ASD has a wide range of syndrome expression and its management presents particular challenges for clinicians. Individuals with an ASD can present for clinical care at any point in development. The multiple developmental and behavioral problems associated with this condition necessitate multidisciplinary care, coordination of services, and advocacy for individuals and their families. Early, sustained intervention and the use of multiple treatment modalities are indicated. Key Words: autism, practice parameters, guidelines, developmental disorders, pervasive developmental disorders. ATTRIBUTION This parameter was developed by Fred Volkmar, M.D., Matthew Siegel, M.D., Marc Woodbury-Smith, M.D., Bryan King, M.D., James McCracken, M.D., Matthew State, M.D., Ph.D. -
Handbook for Parents/Guardians and Students in North Carolina Public Schools
Know Your Rights, Remedies, & Resources A Handbook for Parents/Guardians and Students in North Carolina Public Schools a publication of Advocates for Children's Services a statewide project of Legal Aid of North Carolina 1 Know Your Rights, Remedies, and Resources ADVOCATES FOR CHILDREN’S SERVICES Advocates for Children's Services (ACS) is a statewide project of Legal Aid of North Carolina. The focus of ACS' work is dismantling the school-to-prison pipeline through: High-quality legal advice and representation for children from low-income families who are being pushed out of public school systems through suspensions, expulsions, school-based court referrals, mistreatment by school resource officers, discrimination, unmet educational needs, including special education, and other factors; Community education in the form of trainings, presentations, publications, and media outreach; and Collaboration with and technical assistance for individuals and organizations working for education justice. For more information about ACS, visit www.legalaidnc.org/acs, call 919-226-0052, or email [email protected]. A Handbook for Parents/Guardians and Students in North Carolina Public Schools 2 Produced By: Jason Langberg Equal Justice Works Fellow/Attorney Advocates for Children’s Services Date of Publication: April 2012 Thank you to the following individuals for their contributions to this booklet: Katherine Asaro, Intern, Advocates for Children's Services Brenda Berlin, Supervising Attorney, Duke Children's Law Clinic Christine Bischoff, Staff -

Trojan Terrorism: Revenge Colonists Or Condition of Evolution? (To the Problem “Your/Alien”)
Philosophy Study, April 2018, Vol. 8, No. 4, 191-208 doi: 10.17265/2159-5313/2018.04.005 D DAVID PUBLISHING Trojan Terrorism: Revenge Colonists or Condition of Evolution? (To the Problem “Your/Alien”) Menshikova Elena Rudolfovna Expert New Institute for Cultural Research Thinking about the problem of terrorism, the author finds its origins in the myth of the Trojan War, treating it as a battle for space, which was the primary basis for the civilizational leap—the expansion of the Greek world to the east, which led to the flourishing of Greek culture, creating a precedent of justified colonialism, provided strategy and tactics—the causal apology of violence—all subsequent wars, colonial campaigns, which was no exception for the migratory flows of the XX century, as a result of which the word “terrorism” sounded with by force of the song of B. Brecht. The theme of “space”—chucked away, lost, taken away, destroyed, compressed, anarchic, empty, boundless, virtual—remains vital in our time, when the limitless possibilities lead to the limitation of man himself, his emptiness, and “complete shortness” (Platonov), when the treaty as the basis of human existence is rejected, and when you become the Other yourself. The metaphysics of “violence” is buried in anthropology—in ignorance of one’s limits by man, in denying the boundaries of “another’s,” in unwillingness to ask a question and find the answer, in laziness and, in fact, in the loss of oneself. Keywords: myth, space, terrorism, Own/Alien’s, treaty, another, happiness The subtitle to the topic could be played cinematically: “Good, bad, evil: What is happiness, brother?”—then an allusion to the Scorsese’s western (“Il Buono, il brutto, il cattivo,” 1966) and Balabanov’s film (“Brother,” 1997), that became cultic at different times of the revolutionary 20th century, and as a result of social transformations experienced by a society divided by the ocean, history, and culture to different social formations. -

Boletin De Documentación Nº 37, Marzo De 2009
Su elaboración en formato electrónico, iniciada en julio de 2002, ha supuesto importantes ventajas de cara a ampliar y agilizar su difusión entre los profesionales del sector, permitiendo asimismo la localización de documentación relevante por parte de cualquier ciudadano interesado en el campo de las drogodependencias. Como en los números anteriores, en el boletín de marzo se recogen las principales novedades bibliográficas que, sobre los distintos aspectos relacionados con las adicciones, han tenido entrada en el Centro de Documentación e Información de la Delegación del Gobierno para el Plan Nacional sobre Drogas en los tres últimos meses. El contenido del Boletín está estructurado en tres grandes epígrafes: Novedades bibliográficas (clasificadas por su temática y con indicación de su ruta en el caso de que estén disponibles a texto completo en Internet), Legislación y Sumarios de revistas. Esperamos que el Boletín, cuya difusión se realiza a través de listas de distribución de correo electrónico y de su presencia permanente en la página web de la Delegación del Gobierno para el Plan Nacional sobre Drogas, sea de interés y quedamos a la espera de cualquier sugerencia y/o consulta que sobre el mismo queráis formular. Ministerio de Sanidad y Consumo. Delegación del Gobierno para el Plan Nacional sobre Drogas José del Val – E-correo: [email protected] Jefe de Servicio del Centro de Documentación e Información 1 Aspectos Generales ........................................................................ 4 Aspectos Sociales ............................................................................ -

Specificity of Psychosis, Mania and Major Depression in A
Molecular Psychiatry (2014) 19, 209–213 & 2014 Macmillan Publishers Limited All rights reserved 1359-4184/14 www.nature.com/mp ORIGINAL ARTICLE Specificity of psychosis, mania and major depression in a contemporary family study CL Vandeleur1, KR Merikangas2, M-PF Strippoli1, E Castelao1 and M Preisig1 There has been increasing attention to the subgroups of mood disorders and their boundaries with other mental disorders, particularly psychoses. The goals of the present paper were (1) to assess the familial aggregation and co-aggregation patterns of the full spectrum of mood disorders (that is, bipolar, schizoaffective (SAF), major depression) based on contemporary diagnostic criteria; and (2) to evaluate the familial specificity of the major subgroups of mood disorders, including psychotic, manic and major depressive episodes (MDEs). The sample included 293 patients with a lifetime diagnosis of SAF disorder, bipolar disorder and major depressive disorder (MDD), 110 orthopedic controls, and 1734 adult first-degree relatives. The diagnostic assignment was based on all available information, including direct diagnostic interviews, family history reports and medical records. Our findings revealed specificity of the familial aggregation of psychosis (odds ratio (OR) ¼ 2.9, confidence interval (CI): 1.1–7.7), mania (OR ¼ 6.4, CI: 2.2–18.7) and MDEs (OR ¼ 2.0, CI: 1.5–2.7) but not hypomania (OR ¼ 1.3, CI: 0.5–3.6). There was no evidence for cross-transmission of mania and MDEs (OR ¼ .7, CI:.5–1.1), psychosis and mania (OR ¼ 1.0, CI:.4–2.7) or psychosis and MDEs (OR ¼ 1.0, CI:.7–1.4). -

2021 Psychiatry CERT Content Specifications
CERTIFICATION EXAMINATION IN PSYCHIATRY Beginning in 2017, the American Board of Psychiatry and Neurology, Inc. (ABPN) issued two- dimensional content specifications for the psychiatry, neurology and child neurology certification examinations. Questions for the September 2021 psychiatry, neurology and child neurology certification examinations will conform to these content specifications. Within the two-dimensional format, one dimension is comprised of disorders and topics while the other is comprised of competencies and mechanisms that cut across the various disorders of the first dimension. By design, the two dimensions are interrelated and not independent of each other. All of the questions on the examination will fall into one of the disorders/topics and will be aligned with a competency/mechanism. For example, an item on substance use could focus on treatment, or it could focus on systems-based practice. The psychiatry, neurology and child neurology content specifications can be accessed from the specialty certification section of our website. Candidates should use the detailed content specifications as a guide to prepare for a certification examination. Scores for these examinations will be reported in a standardized format rather than the previous percent correct format. Starting in 2018, all future examinations given by the ABPN will gradually conform to the two- dimensional content specification. The American Board of Psychiatry and Neurology, Inc. is a not-for-profit corporation dedicated to serving the public interest and the professions of psychiatry and neurology by promoting excellence in practice through certification and continuing certification processes. For more information, please contact us at [email protected] or visit our website at www.abpn.com. -
Reasonable Accommodations: a Faculty Guide to Teaching College Students with Disabilities
CUNY Council on Student Disability Issues (COSDI) City University of New York Central Office of Student Affairs 555 West 57th Street, Suite 1401 New York, NY. 10019 Published October 2014 Reasonable Accommodations II Table of Contents Foreword ......................................................................................... 5 Introduction ..................................................................................... 7 The Law .......................................................................................... 9 Disability Categories ..................................................................... 11 Teaching Students with Disabilities.............................................. 12 Universal Design in Learning ....................................................... 15 University-Wide Accessibility Projects ........................................ 18 Technology in the Classroom and for Online Courses ................. 23 Alternative Text for Students with Disabilities ............................ 27 Learning Disabilities ..................................................................... 28 Attention Deficit/Hyperactivity Disorders (AD/HD) ................... 32 Neurological Disabilities .............................................................. 36 Traumatic Brain Injury (TBI) ....................................................... 38 Autism Spectrum Disorder/ Asperger’s Syndrome ...................... 40 Psychological Disorders................................................................ 43 Mobility -

Songs from the Second Floor 179 Chapter 9: Sin: Werckmeister Harmonies 193 Chapter 10: Guilt: Dog Days; You the Living; Import Export 205
University of Bath PHD A 'Post-Historical' Cinema of Suspense: Jean-Luc Nancy and the Limits of Redemption Callow, James Award date: 2010 Awarding institution: University of Bath Link to publication Alternative formats If you require this document in an alternative format, please contact: [email protected] General rights Copyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright owners and it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights. • Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ? Take down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Download date: 24. Sep. 2021 A „Post-Historical‟ Cinema of Suspense Jean-Luc Nancy and the Limits of Redemption James Callow A thesis submitted for the degree of Doctor of Philosophy University of Bath Department of European Studies and Modern Languages November 2010 COPYRIGHT Attention is drawn to the fact that copyright of this thesis rests with the author. This copy of the thesis has been supplied on condition that anyone who consults it is understood to recognise that its copyright rests with its author and that no quotation from the thesis and no information derived from it may be published without the prior written consent of the author. -

Why Do We Need a Social Psychiatry? Antonio Ventriglio, Susham Gupta and Dinesh Bhugra
The British Journal of Psychiatry (2016) 209, 1–2. doi: 10.1192/bjp.bp.115.175349 Editorial Why do we need a social psychiatry? Antonio Ventriglio, Susham Gupta and Dinesh Bhugra Summary interventions in psychiatry should be considered in the Human beings are social animals, and familial or social framework of social context where patients live and factors relationships can cause a variety of difficulties as well as they face on a daily basis. providing support in our social functioning. The traditional way of looking at mental illness has focused on abnormal Declaration of interest thoughts, actions and behaviours in response to internal D.B. is President of the World Psychiatric Association. causes (such as biological factors) as well as external ones such as social determinants and social stressors. We Copyright and usage contend that psychiatry is social. Mental illness and B The Royal College of Psychiatrists 2016. and difficulties at these levels can lead to psychopathological Antonio Ventriglio (pictured) is an honorary researcher at the Department of and behavioural dysfunctions. Social stressors can lead to changes Clinical and Experimental Medicine at the University of Foggia, Italy. Susham 5 Gupta is a consultant psychiatrist at the East London Mental Health in the cerebral structure and affect neuro-hormonal pathways. Foundation NHS Trust. Dinesh Bhugra is Emeritus Professor of Mental Health Even organic conditions such as dementia are said to be related to & Cultural Diversity at the Institute of Psychiatry, Psychology & Neuroscience, life events and social factors such as economic and educational status.5 King’s College London and is President of the World Psychiatric Association. -

NEW RESEARCH BOOK I a I 2011 H AW Photo By: Hawaii Tourism Authority Tourism By:Photo Hawaii
NEW RESEARCH BOOK I I A AW 2011 H Photo By: Hawaii Tourism Authority Tourism By:Photo Hawaii American Psychiatric Association Transforming Mental Health Through Leadership, Discovery and Collaboration WWW.PSYCH.ORG NEW RESEARCH BOOK NEW RESEARCH RESIDENT POSTER SESSION 01 Chp.: Michel Burger M.D., Centre Hospitalier Erstein, May 14, 2011 13 route de Krafft BP 30063, Erstein, 67152 France, 10 – 11:30 AM Co-Author(s): Christelle Nithart, Ph.D., Luisa Weiner, Hawaii Convention Center, Exhibit Hall, Level 1 M.Sc., Jean-Philippe Lang, M.D. NR01‑01 PROMOTING HEALTH THROUGH THE SUMMARY: BEAUTIFUL GAME: ENGAGING WITH Introduction We present the psychiatric AND ADVOCATING FOR RESIDENTS OF rehabilitation program we are developing in VANCOUVER’S DOWNTOWN EASTSIDE Erstein, France, since September 2008. This THROUGH STREET SOCCER program is based on a residential facility located in the community, which is conceived as an Chp.:Alan Bates M.D., Psychiatry Dept., 11th Floor, interface between inpatient care and psychosocial Gordon & Leslie Diamond Health Care Centre, 2775 rehabilitation. Objective To evaluate the viability Laurel St., Vancouver, V5L 2V8 Canada, Co-Author(s): of the Courlis residential facility in facilitating Fidel Vila-Rodriguez, M.D., Siavash Jafari, M.D., patients’ psychiatric rehabilitation. Method Lurdes Tse, B.Sc., Rachel Ilg, R.N., William Honer, M.D. A comprehensive psychosocial and medical evaluation is undertaken at admission. Criteria for SUMMARY: admission are the following: functional disability Vancouver’s Downtown Eastside is one of the due to chronic psychiatric illness in symptomatic poorest neighbourhoods in North America. remission, and very low socioeconomic status. A Mental illness and addictions are prevalent and socio‑educative and a psychiatric team act together contribute significantly to marginalization and to improve independent social functioning, social disadvantage.Street Soccer for people affected symptomatic remission, and quality of life, according by homelessness re‑engages marginalized people to individual profiles and aims. -

Pharmacology on Your Palms CLASSIFICATION of the DRUGS
Pharmacology on your palms CLASSIFICATION OF THE DRUGS DRUGS FROM DRUGS AFFECTING THE ORGANS CHEMOTHERAPEUTIC DIFFERENT DRUGS AFFECTING THE NERVOUS SYSTEM AND TISSUES DRUGS PHARMACOLOGICAL GROUPS Drugs affecting peripheral Antitumor drugs Drugs affecting the cardiovascular Antimicrobial, antiviral, Drugs affecting the nervous system Antiallergic drugs system antiparasitic drugs central nervous system Drugs affecting the sensory Antidotes nerve endings Cardiac glycosides Antibiotics CNS DEPRESSANTS (AFFECTING THE Antihypertensive drugs Sulfonamides Analgesics (opioid, AFFERENT INNERVATION) Antianginal drugs Antituberculous drugs analgesics-antipyretics, Antiarrhythmic drugs Antihelminthic drugs NSAIDs) Local anaesthetics Antihyperlipidemic drugs Antifungal drugs Sedative and hypnotic Coating drugs Spasmolytics Antiviral drugs drugs Adsorbents Drugs affecting the excretory system Antimalarial drugs Tranquilizers Astringents Diuretics Antisyphilitic drugs Neuroleptics Expectorants Drugs affecting the hemopoietic system Antiseptics Anticonvulsants Irritant drugs Drugs affecting blood coagulation Disinfectants Antiparkinsonian drugs Drugs affecting peripheral Drugs affecting erythro- and leukopoiesis General anaesthetics neurotransmitter processes Drugs affecting the digestive system CNS STIMULANTS (AFFECTING THE Anorectic drugs Psychomotor stimulants EFFERENT PART OF THE Bitter stuffs. Drugs for replacement therapy Analeptics NERVOUS SYSTEM) Antiacid drugs Antidepressants Direct-acting-cholinomimetics Antiulcer drugs Nootropics (Cognitive