The ICD-10 Classification of Mental and Behavioural Disorders Diagnostic Criteria for Research
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Paranoid – Suspicious; Argumentative; Paranoid; Continually on The
Disorder Gathering 34, 36, 49 Answer Keys A N S W E R K E Y, Disorder Gathering 34 1. Avital Agoraphobia – 2. Ewelina Alcoholism – 3. Martyna Anorexia – 4. Clarissa Bipolar Personality Disorder –. 5. Lysette Bulimia – 6. Kev, Annabelle Co-Dependant Relationship – 7. Archer Cognitive Distortions / all-of-nothing thinking (Splitting) – 8. Josephine Cognitive Distortions / Mental Filter – 9. Mendel Cognitive Distortions / Disqualifying the Positive – 10. Melvira Cognitive Disorder / Labeling and Mislabeling – 11. Liat Cognitive Disorder / Personalization – 12. Noa Cognitive Disorder / Narcissistic Rage – 13. Regev Delusional Disorder – 14. Connor Dependant Relationship – 15. Moira Dissociative Amnesia / Psychogenic Amnesia – (*Jason Bourne character) 16. Eylam Dissociative Fugue / Psychogenic Fugue – 17. Amit Dissociative Identity Disorder / Multiple Personality Disorder – 18. Liam Echolalia – 19. Dax Factitous Disorder – 20. Lorna Neurotic Fear of the Future – 21. Ciaran Ganser Syndrome – 22. Jean-Pierre Korsakoff’s Syndrome – 23. Ivor Neurotic Paranoia – 24. Tucker Persecutory Delusions / Querulant Delusions – 25. Lewis Post-Traumatic Stress Disorder – 26. Abdul Proprioception – 27. Alisa Repressed Memories – 28. Kirk Schizophrenia – 29. Trevor Self-Victimization – 30. Jerome Shame-based Personality – 31. Aimee Stockholm Syndrome – 32. Delphine Taijin kyofusho (Japanese culture-specific syndrome) – 33. Lyndon Tourette’s Syndrome – 34. Adar Social phobias – A N S W E R K E Y, Disorder Gathering 36 Adjustment Disorder – BERKELEY Apotemnophilia -

First Episode Psychosis an Information Guide Revised Edition
First episode psychosis An information guide revised edition Sarah Bromley, OT Reg (Ont) Monica Choi, MD, FRCPC Sabiha Faruqui, MSc (OT) i First episode psychosis An information guide Sarah Bromley, OT Reg (Ont) Monica Choi, MD, FRCPC Sabiha Faruqui, MSc (OT) A Pan American Health Organization / World Health Organization Collaborating Centre ii Library and Archives Canada Cataloguing in Publication Bromley, Sarah, 1969-, author First episode psychosis : an information guide : a guide for people with psychosis and their families / Sarah Bromley, OT Reg (Ont), Monica Choi, MD, Sabiha Faruqui, MSc (OT). -- Revised edition. Revised edition of: First episode psychosis / Donna Czuchta, Kathryn Ryan. 1999. Includes bibliographical references. Issued in print and electronic formats. ISBN 978-1-77052-595-5 (PRINT).--ISBN 978-1-77052-596-2 (PDF).-- ISBN 978-1-77052-597-9 (HTML).--ISBN 978-1-77052-598-6 (ePUB).-- ISBN 978-1-77114-224-3 (Kindle) 1. Psychoses--Popular works. I. Choi, Monica Arrina, 1978-, author II. Faruqui, Sabiha, 1983-, author III. Centre for Addiction and Mental Health, issuing body IV. Title. RC512.B76 2015 616.89 C2015-901241-4 C2015-901242-2 Printed in Canada Copyright © 1999, 2007, 2015 Centre for Addiction and Mental Health No part of this work may be reproduced or transmitted in any form or by any means electronic or mechanical, including photocopying and recording, or by any information storage and retrieval system without written permission from the publisher—except for a brief quotation (not to exceed 200 words) in a review or professional work. This publication may be available in other formats. For information about alterna- tive formats or other CAMH publications, or to place an order, please contact Sales and Distribution: Toll-free: 1 800 661-1111 Toronto: 416 595-6059 E-mail: [email protected] Online store: http://store.camh.ca Website: www.camh.ca Disponible en français sous le titre : Le premier épisode psychotique : Guide pour les personnes atteintes de psychose et leur famille This guide was produced by CAMH Publications. -

DCF Pamphlet 155-2: Appendix 3
DCF Pamphlet 155-2: Appendix 3 Appendix 3: The table below shows the ICD9 codes that are acceptable in the Substance Abuse and Mental Health Information System (SAMHIS). This replaces all previous versions of allowable ICD9 codes used in the Substance Abuse and Mental Health Information System. The following are the codes and their meaning. STATUS: 0 = Inactive, code is not usable, 1 = Active, this will show in SAMHIS. PROGRAM CODE: N = Not Active, M = Mental Health Code, S = Substance Abuse Code B = Behavioral Health (can be used for either a mental health or substance abuse diagnosis) NOTE: Codes with ‘N’ (Not Active) in the Program Code are for historical purposes only. ICD9 PROGRAM Code STATUS DESCRIPTION CODE 095.7 0 SYPHILIS OF TENDON/BURSA N 196.8 0 MAL NEO LYMPH NODE-MULT N 259.9 0 ENDOCRINE DISORDER NOS N 269.0 0 DEFICIENCY OF VITAMIN K N 289.9 0 BLOOD DISEASE NOS N 290 0 Senile and presenile organic psychotic conditions N 290.0 0 SENILE DEMENTIA UNCOMP N 290.1 0 Presenile dementia N 290.10 0 PRESENILE DEMENTIA N 290.11 0 PRESENILE DELIRIUM N 290.12 0 PRESENILE DELUSION M 290.13 0 PRESENILE DEPRESSION M 290.2 0 Senile dementia with delusional or depressive feat M 290.20 0 SENILE DELUSION M 290.21 0 SENILE DEPRESSIVE M 290.3 0 SENILE DELIRIUM N 290.4 0 Arteriosclerotic dementia N 290.40 0 ARTERIOSCLER DEMENT NOS N 290.41 0 ARTERIOSCLER DELIRIUM N 290.42 0 ARTERIOSCLER DELUSION M 290.43 0 ARTERIOSCLER DEPRESSIVE M 290.8 0 SENILE PSYCHOSIS NEC N 290.9 0 SENILE PSYCHOT COND NOS N 291 1 Alcohol psychoses S 291.0 1 DELIRIUM TREMENS -

Types of Bipolar Disorder Toms Are Evident
MOOD DISORDERS ASSOCIATION OF BRITISH COLUmbIA T Y P E S O F b i p o l a r d i s o r d e r Bipolar disorder is a class of mood disorders that is marked by dramatic changes in mood, energy and behaviour. The key characteristic is that people with bipolar disorder alternate be- tween episodes of mania (extreme elevated mood) and depression (extreme sadness). These episodes can last from hours to months. The mood distur- bances are severe enough to cause marked impairment in the person’s func- tioning. The experience of mania is not pleasant and can be very frightening to The Diagnotistic Statisti- the person. It can lead to impulsive behaviour that has serious consequences cal Manual (DSM- IV-TR) is a for the person and their family. A depressive episode makes it difficult or -im manual used by doctors to possible for a person to function in their daily life. determine the specific type of bipolar disorder. People with bipolar disorder vary in how often they experience an episode of either mania or depression. Mood changes with bipolar disorder typically occur gradually. For some individuals there may be periods of wellness between the different mood episodes. Some people may also experience multiple episodes within a 12 month period, a week, or even a single day (referred to as “rapid cycling”). The severity of the mood can also range from mild to severe. Establishing the particular type of bipolar disorder can greatly aid in determin- ing the best type of treatment to manage the symptoms. -

ICD-10 Mental Health Billable Diagnosis Codes in Alphabetical
ICD-10 Mental Health Billable Diagnosis Codes in Alphabetical Order by Description IICD-10 Mental Health Billable Diagnosis Codes in Alphabetic Order by Description Note: SSIS stores ICD-10 code descriptions up to 100 characters. Actual code description can be longer than 100 characters. ICD-10 Diagnosis Code ICD-10 Diagnosis Description F40.241 Acrophobia F41.0 Panic Disorder (episodic paroxysmal anxiety) F43.0 Acute stress reaction F43.22 Adjustment disorder with anxiety F43.21 Adjustment disorder with depressed mood F43.24 Adjustment disorder with disturbance of conduct F43.23 Adjustment disorder with mixed anxiety and depressed mood F43.25 Adjustment disorder with mixed disturbance of emotions and conduct F43.29 Adjustment disorder with other symptoms F43.20 Adjustment disorder, unspecified F50.82 Avoidant/restrictive food intake disorder F51.02 Adjustment insomnia F98.5 Adult onset fluency disorder F40.01 Agoraphobia with panic disorder F40.02 Agoraphobia without panic disorder F40.00 Agoraphobia, unspecified F10.180 Alcohol abuse with alcohol-induced anxiety disorder F10.14 Alcohol abuse with alcohol-induced mood disorder F10.150 Alcohol abuse with alcohol-induced psychotic disorder with delusions F10.151 Alcohol abuse with alcohol-induced psychotic disorder with hallucinations F10.159 Alcohol abuse with alcohol-induced psychotic disorder, unspecified F10.181 Alcohol abuse with alcohol-induced sexual dysfunction F10.182 Alcohol abuse with alcohol-induced sleep disorder F10.121 Alcohol abuse with intoxication delirium F10.188 Alcohol -

Inflated Praise Leads Socially Anxious Children to Blush
UvA-DARE (Digital Academic Repository) When gushing leads to blushing: Inflated praise leads socially anxious children to blush Nikolić , M.; Brummelman, E.; Colonnesi, C.; de Vente, W.; Bögels, S.M. DOI 10.1016/j.brat.2018.04.003 Publication date 2018 Document Version Final published version Published in Behaviour Research and Therapy Link to publication Citation for published version (APA): Nikolić , M., Brummelman, E., Colonnesi, C., de Vente, W., & Bögels, S. M. (2018). When gushing leads to blushing: Inflated praise leads socially anxious children to blush. Behaviour Research and Therapy, 106, 1-7. https://doi.org/10.1016/j.brat.2018.04.003 General rights It is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons). Disclaimer/Complaints regulations If you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, stating your reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Ask the Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam, The Netherlands. You will be contacted as soon as possible. UvA-DARE is a service provided by the library of the University of Amsterdam (https://dare.uva.nl) Download date:24 Sep 2021 Behaviour Research and Therapy 106 (2018) 1–7 Contents lists available at ScienceDirect Behaviour Research and Therapy journal homepage: www.elsevier.com/locate/brat When gushing leads to blushing: Inflated praise leads socially anxious T children to blush ∗ Milica Nikolića, , Eddie Brummelmana,b, Cristina Colonnesia, Wieke de Ventea, Susan M. -

Behavorial Health Department – Primary Care Center and Fireweed Treatment Guidelines for Cognitive Disorders
BEHAVORIAL HEALTH DEPARTMENT – PRIMARY CARE CENTER AND FIREWEED TREATMENT GUIDELINES FOR COGNITIVE DISORDERS EXECUTIVE SUMMARY .................................................................................................... 2 INTRODUCTION AND STATEMENT OF INTENT .................................................................................2 DEFINITION OF DISORDER......................................................................................................2 GENERAL GOALS OF TREATMENT ..............................................................................................3 SUMMARY OF 1ST, 2ND AND 3RD LINE TREATMENT ............................................................................3 CLINICAL AND DEMOGRAPHIC ISSUES THAT INFLUENCE TREATMENT PLANNING..........................................3 FLOW DIAGRAM ............................................................................................................. 4 ASSESSMENT.................................................................................................................. 5 PSYCHIATRIC ASSESSMENT ....................................................................................................5 PSYCHOLOGICAL TESTING ......................................................................................................5 SCREENING/SCALES ............................................................................................................5 MODALITIES & TREATMENT MODELS............................................................................. -

Guidelines for Treating Dissociative Identity Disorder in Adults, Third
This article was downloaded by: [208.78.151.82] On: 21 October 2011, At: 09:20 Publisher: Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Journal of Trauma & Dissociation Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/wjtd20 Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision International Society for the Study of Trauma and Dissociation Available online: 03 Mar 2011 To cite this article: International Society for the Study of Trauma and Dissociation (2011): Guidelines for Treating Dissociative Identity Disorder in Adults, Third Revision, Journal of Trauma & Dissociation, 12:2, 115-187 To link to this article: http://dx.doi.org/10.1080/15299732.2011.537247 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material. -
DSM III and ICD 9 Codes 11-2004
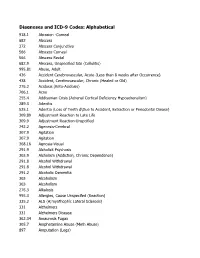
Diagnoses and ICD-9 Codes: Alphabetical 918.1 Abrasion -Corneal 682 Abscess 372 Abscess Conjunctiva 566 Abscess Corneal 566 Abscess Rectal 682.9 Abscess, Unspecified Site (Cellulitis) 995.81 Abuse, Adult 436 Accident Cerebrovascular, Acute (Less than 8 weeks after Occurrence) 438 Accident, Cerebrovascular, Chronic (Healed or Old) 276.2 Acidosis (Keto-Acidosis) 706.1 Acne 255.4 Addisonian Crisis (Adrenal Cortical Deficiency Hypoadrenalism) 289.3 Adenitis 525.1 Adentia (Loss of Teeth d\Due to Accident, Extraction or Periodontal Diease) 309.89 Adjustment Reaction to Late Life 309.9 Adjustment Reaction-Unspcified 742.2 Agenesis-Cerebral 307.9 Agitation 307.9 Agitation 368.16 Agnosia-Visual 291.9 Alcholick Psychosis 303.9 Alcholism (Addiction, Chronic Dependence) 291.8 Alcohol Withdrawal 291.8 Alcohol Withdrawal 291.2 Alcoholic Dementia 303 Alcoholism 303 Alcoholism 276.3 Alkalosis 995.3 Allergies, Cause Unspecifed (Reaction) 335.2 ALS (A;myothophic Lateral Sclerosis) 331 Alzheimers 331 Alzheimers Disease 362.34 Amaurosis Fugax 305.7 Amphetamine Abuse (Meth Abuse) 897 Amputation (Legs) 736.89 Amputation, Leg, Status Post (Above Knee, Below Knee) 736.9 Amputee, Site Unspecified (Acquired Deformity) 285.9 Anemia 284.9 Anemia Aplastic (Hypoplastic Bone Morrow) 280 Anemia Due to loss of Blood 281 Anemia Pernicious 280.9 Anemia, Iron Deficiency, Unspecified 285.9 Anemia, Unspecified (Normocytic, Not due to blood loss) 281.9 Anemia, Unspecified Deficiency (Macrocytic, Nutritional 441.5 Aneurysm Aortic, Ruptured 441.1 Aneurysm, Abdominal 441.3 Aneurysm, -

Research on Child Mental Issues in the Field of Prevention 1. Mental
Research on child mental issues in the field of prevention Helmut Remschmidt* 1. Mental disorders / Classification, developmental aspects 2. Epidemiology and time trends 3. Types and goals of preventive interventions: risk factors and protective factors 4. Prevention programs * Prof. Helmut Remschmidt, MD, PhD, Dept. Child and Adolescent Psychiatry and Psychotherapy, Philipps-University, D-35033 Marburg (Germany) email: [email protected] A Concept of Disease/Disorder "A psychopathological disorder can be described as a state of involuntarily disturbed functions characterized by a more or less clearly defined begin, course and end preventing a child or an adolescent from taking an active part in his age-appropriate life and developmental tasks" (Remschmidt, 1988) Multiaxial System According to ICD-10 Axis 1: Clinical psychiatric syndromes Axis 2: Specific disorders of psychological development Axis 3: Intellectual level Axis 4: Medical conditions Axis 5: Associated abnormal psychosocial situations Axis 6: Global assessment of psychosocial disability Potential Relationship Between Psychopathology and Developmental Tasks (Garber, 1984) Psychopathological Developmental tasks disorder Separation anxiety Object permanence, attachment Depression Differentiation of self, self esteem, social comparison Suicide Concept of death, time perspective (future) Conduct disorder, Moral development Undersocialized Aggressive Perspective-taking, empathy Impulsivity Delay of gratification Oppositional disorder Autonomy, individuation Schizoid disorder Peer relation, friendship patterns Natural History of Tics and Associated Behaviors A Critique of Existing Classifications From a Developmental Perspective (Graham & Skuse, 1992) 1. Exclusion of causal processes 2. Disregard of the longitudinal course (example: Gilles de la Tourette-syndrome) 3. Insufficient consideration of age at onset (phases of life) 4. Insufficient judgement of developmental appropriateness of possibly abnormal behaviour (e.g. -

Reactive Attachment Disorder of Infancy Or Early Childhood
CASE STUDY Reactive Attachment Disorder of Infancy or Early Childhood MARGOT MOSER RICHTERS, PH.D., AND FRED R. VOLKMAR, M.D. ABSTRACT Since its introduction into DSM-Ill, reactive attachment disorder has stood curiously apart from other diagnoses for two reasons: it remains the only diagnosis designed for infants, and it requires the presence of a specific etiology. This paper describes the pattern of disturbances demonstrated by some children who meet DSM-Ill-R criteria for reactive attachment disorder. Three suggestions are made: (1) the sensitivity and specificity of the diagnostic concept may be enhanced by including criteria detailing the developmental problems exhibited by these children; (2) the etiological requirement should be discarded given the difficulties inherent in obtaining complete histories for these children, as well as its inconsistency with ICD-10; and (3) the diagnosis arguably is not a disorder of attachment but rather a syndrome of atypical development. J. Am. Acad. Child Adolesc. Psychiatry,1994, 33, 3: 328-332. Key Words: reactive attachment disorder, maltreatment, DSM-Ill-R Reactive attachment disorder (RAD) was included in social responsiveness, apathy, and onset before 8 DSM-III in 1980 (American Psychiatric Association, months. Only one criterion addressed the quality of 1980), reflecting an awareness of a body of literature mother-infant attachment. on the effects of deprivation and institutionalization Several aspects of the definition were unsatisfactory on infants and young children (Bakwin, 1949; Bowlby, (Rutter and Shaffer, 1980), and substantial modifica- tions were made in DSM-III-R (American Psychiatric 1944; Provence and Lipton, 1962; Rutter, 1972; Skeels Association, 1987): the age of onset was raised to age and Dye, 1939; Skuse, 1984; Spitz, 1945; Tizard and 5 years, consistent with data on the development of Rees, 1975). -

Department of Veterans Affairs § 4.130
Department of Veterans Affairs § 4.130 than 50 percent and schedule an exam- upon the Diagnostic and Statistical ination within the six month period Manual of Mental Disorders, Fourth following the veteran’s discharge to de- Edition, of the American Psychiatric termine whether a change in evalua- Association (DSM-IV). Rating agencies tion is warranted. must be thoroughly familiar with this (Authority: 38 U.S.C. 1155) manual to properly implement the di- rectives in § 4.125 through § 4.129 and to [61 FR 52700, Oct. 8, 1996] apply the general rating formula for § 4.130 Schedule of ratings—mental mental disorders in § 4.130. The sched- disorders. ule for rating for mental disorders is The nomenclature employed in this set forth as follows: portion of the rating schedule is based Rating Schizophrenia and Other Psychotic Disorders 9201 Schizophrenia, disorganized type 9202 Schizophrenia, catatonic type 9203 Schizophrenia, paranoid type 9204 Schizophrenia, undifferentiated type 9205 Schizophrenia, residual type; other and unspecified types 9208 Delusional disorder 9210 Psychotic disorder, not otherwise specified (atypical psychosis) 9211 Schizoaffective disorder Delirium, Dementia, and Amnestic and Other Cognitive Disorders 9300 Delirium 9301 Dementia due to infection (HIV infection, syphilis, or other systemic or intracranial infections) 9304 Dementia due to head trauma 9305 Vascular dementia 9310 Dementia of unknown etiology 9312 Dementia of the Alzheimer’s type 9326 Dementia due to other neurologic or general medical conditions (endocrine