Sengamala Thayaar Educational Trust Women's College
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Characterization of Murine Macrophages from Bone Marrow
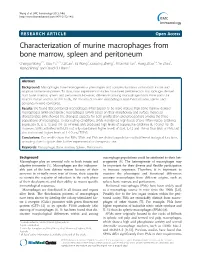
Wang et al. BMC Immunology 2013, 14:6 http://www.biomedcentral.com/1471-2172/14/6 RESEARCH ARTICLE Open Access Characterization of murine macrophages from bone marrow, spleen and peritoneum Changqi Wang1*†, Xiao Yu1,2†, Qi Cao1, Ya Wang1, Guoping Zheng1, Thian Kui Tan1, Hong Zhao1,3, Ye Zhao1, Yiping Wang1 and David CH Harris1 Abstract Background: Macrophages have heterogeneous phenotypes and complex functions within both innate and adaptive immune responses. To date, most experimental studies have been performed on macrophages derived from bone marrow, spleen and peritoneum. However, differences among macrophages from these particular sources remain unclear. In this study, the features of murine macrophages from bone marrow, spleen and peritoneum were compared. Results: We found that peritoneal macrophages (PMs) appear to be more mature than bone marrow derived macrophages (BMs) and splenic macrophages (SPMs) based on their morphology and surface molecular characteristics. BMs showed the strongest capacity for both proliferation and phagocytosis among the three populations of macrophage. Under resting conditions, SPMs maintained high levels of pro-inflammatory cytokines expression (IL-6, IL-12 and TNF-α), whereas BMs produced high levels of suppressive cytokines (IL-10 and TGF-β). However, SPMs activated with LPS not only maintained higher levels of (IL-6, IL-12 and TNF-α) than BMs or PMs, but also maintained higher levels of IL-10 and TGF-β. Conclusions: Our results show that BMs, SPMs and PMs are distinct populations with different biological functions, providing clues to guide their further experimental or therapeutic use. Keywords: Macrophage, Bone marrow, Spleen, Peritoneum Background macrophage populations could be attributed to their het- Macrophages play an essential role in both innate and erogeneity [4]. -

1 | Page: Immune Cells and Tissues Swailes Cells and Tissues of The
Cells and Tissues of the Immune System N. Swailes, Ph.D. Department of Anatomy and Cell Biology Rm: B046A ML Tel: 5-7726 E-mail: [email protected] Required reading Mescher AL, Junqueira’s Basic Histology Text and Atlas, 12th Edition, Chapter 20: pp226-2480 Ross MH and Pawlina W, Histology: A text and Atlas, 6th Edition, Chapter 21: pp396-429 Learning objectives 1) Identify the major cells of the immune system and briefly outline their function 2) Describe the general structure of lymphoid tissue 3) Differentiate between primary and secondary immune organs 4) Identify the thymus and discuss the role of its cells in ‘educating’ immature T-cells 5) Identify a lymph node and outline how an immune response is triggered here 6) Identify the spleen and describe the role of red and white pulp in filtering the blood and reacting to blood borne antigens 7) Differentiate between MALT in the oral cavity (tonsils) 8) Know where to find and how to identify examples of BALT and GALT Major Take Home Points A. Lymphoid tissues are composed of different types of lymphocytes and supporting cells within a scaffold of Type III collagen/reticular fibers B. The major primary lymphoid organs are encapsulated organs where immature lymphocytes are born (bone marrow) and become immunocompetent (thymus) C. The major secondary lymphoid organs are encapsulated organs where immunocompetent lymphocytes differentiate into effector cells after exposure to antigen in the blood (spleen) or lymph (nodes) D. Mucosa Associated Lymphoid Tissues (MALT) are un-encapsulated areas of lymphoid tissue within the mucosa of organs that can be identified by their lining epithelium (tonsils, GALT: ileum and appendix, BALT) 1 | Page: Immune Cells and Tissues Swailes A1: Organization of the immune system 5a A. -

The Spleen ABOLARIN A.T BUTH, OGBOMOSO Outline
The Spleen ABOLARIN A.T BUTH, OGBOMOSO Outline Structure and physiology Functions Diseases associated with the spleen The major functions of the spleen are (i) filtration and ‘quality control’ of red cells within the circulation (ii) capture and destruction of blood-borne pathogens (iii) generation of adaptive immune responses. In order to achieve these aims the Spleen has evolved a unique anatomical structure that is based on the filtering of blood through two main systems. These consist of a white pulp, which is concerned mainly with immunological function, and a red pulp, which regulates the selection of red cells for re-entry into the circulation. Structure of the spleen The normal spleen weighsabout 150–250 g, but there is considerable variation between normal individuals and at various ages in the same individual. At puberty it weighs about 200–300 g but after the age of 65 years this decreases to 100–150 g or less. In the adult its length is 8–13cm, width 4.5–7.0 cm, surface area 45– 80 cm2 and volume less than 275 cm3. A spleen greater than 14 cm long is usually palpable. Blood flow It is enclosed by a connective tissue framework that extends inwards to form a fibrous network. Blood enters at the pelvis and the majority of vessels open into these open networks(the red pulp) before re-entering the closed venous system. There is no afferent lymphatic to the spleen and the efferent lymphatic system leaves along the route of the splenic vein. The spleen contains a large amount of lymphatic tissue that is mostly concentrated in concentric rings around the arterioles (white pulp). -

Other Useful Books
Other Useful Books Dictionaries: Leeson TS, Leeson CR: Histology, 4th ed. Philadel phia: Saunders, 1981. Dorland's Illustrated Medical Dictionary, 26th ed. Lentz, TL: Cell Fine Structure. Philadelphia: Saun Philadelphia: Saunders, 1981. ders, 1971. Melloni's Illustrated Medical Dictionary. Balti Rhodin JAG: Histology, A Text and Atlas. New more: Williams and Wilkins, 1979. York: Oxford University Press, 1974. Stedman's Illustrated Medical Dictionary, 24th ed. Williams PL, Warwick R: Gray's Anatomy, 36th Baltimore: Williams and Wilkins, 1982. English edition. Philadelphia: Saunders, 1980. Weiss L, Greep ROO: Histology, 4th ed. New York: McGraw-Hill, 1977. Textbooks: Histology and Cytology Wheater PR, Burkitt HG, Daniels VG: Functional Arey LB: Human Histology, 4th ed. Philadelphia: Histology. Edinburgh: Churchill Livingstone, 1979. Saunders, 1974. Bloom W, Fawcett DW: A Textbook of Histology, Textbooks: Pathology 10th ed. Philadelphia: Saunders, 1974. Anderson WAD, Kissane JM: Pathology, 7th ed. Borysenko M, Borysenko J, Beringer T, Gustafson St. Louis: Mosby, 1977. A: Functional Histology. A Core Text. Boston: Lit tle, Brown, 1979. Anderson WAD, Scotti TM: Synopsis of Pathology, 10th ed. St. Louis: Mosby, 1980. Copenhaver WM, Kelly DE, Wood RL: Bailey's Golden A: Pathology. Understanding Human Dis Textbook of Histology, 17th ed. Baltimore: Wil ease. Baltimore: Williams and Wilkins, 1982. liams and Wilkins, 1978. King D, Geller LM, Krieger P, Silva F, Lefkowitch Cowdry EV: A Textbook of Histology, 4th ed. Phila JH: A Survey of Pathology. New York: Oxford delphia: Lea and Febiger, 1950. University Press, 1976. Dyson RD: Cell Biology. A Molecular Approach, Robbins SL, Cotran RS: Pathologic Basis of Dis 2nd ed. Boston: Allyn and Bacon, 1978. -

Lymphatic Organs the Lymphatic Organs Are Classified in To: 1
Lymphatic organs The lymphatic organs are classified in to: 1. Primary (central) lymphoid organs: responsible for development and maturation of lymphocytes. It consists of bone marrow and thymus gland. 2. Secondary (peripheral) lymphoid organs: Site where mature lymphocytes react with antigen. It consists of lymph node, spleen, lymphatic tonsil and diffuse lymphatic nodules. Thymus gland A primary lymphatic organ responsible for maturation of T lymphocytes to become immuno-competent (functional). Size of the thymus varies with age: - In infants, it is found in the inferior neck and extends into the mediastinum where it partially overlies the heart. It increases in size and is most active during childhood. - It stops growing during adolescence and then gradually atrophies. Structure: 1. Stroma: - Capsule: Thin CT capsule surrounding the gland - Septa: extend from the inner surface of the capsule into the gland tissue dividing it into lobules. - Epithelial-reticular cells (not reticular connective tissue): ñ don´t form reticular fibers. ñ joined together with desmosome forming the stromal background of the thymus. ñ Important for blood thymic barrier (will be mentioned later). Parenchyma: Thymic lobes contain an outer cortex and inner medulla Cortex: It is the outer dark part of the thymus lobule and contains • Lymphocytes: Most thymic cells are immature T-lymphocytes. They are rapidly dividing and densely packed. • Few macrophages. Medulla: It appears lighter than the cortex: • Few number of mature T lymphocytes • Thymic (Hassall’s) corpuscles: Consisting of concentric whorls of keratinized epithelial cells, which are thought to be degenerate epithelial cells. Recently it is evidenced that Hassall’s corpuscles are involved in the development of a class of T lymphocytes called regulatory T cells, which are important for preventing autoimmune responses. -

Lymphoid Tissue
Lymphoid Tissue Dr Punita manik Professor Department of Anatomy K G’s Medical University U P Lucknow Classification • Diffuse Lymphoid tissue: diffuse arrangement of lymphocytes and plasma cells deep to epithelium in Lamina propria of digestive, respiratory and urogenital tracts forming an immunological barrier against invasion of microorganisms. • Dense Lymphoid tissue: presence of lymphocytes in the form of nodules Classification Dense Lymphoid Tissue: Nodules are found either in association with mucous membranes of viscera or as discrete encapsulated organs. 2 Types 1. MALT(Mucosa associated Lymphoid Tissue; Nonencapsulated) 2. Discrete Lymphoid organs (Encapsulated) • MALT: Solitary Nodules Aggregated Nodules(Peyer’s patches) Lymphoid nodules in vermiform appendix Waldeyer’s ring at the entrance of pharynx • Discrete Lymphoid Organs: Thymus Lymph Node Spleen Tonsil Lymph Node • Connective tissue framework Capsule Trabecula Reticular Stroma (fibres) Components of Lymph Node • Parenchyma 1.Cortex 2.Paracortex (Inner Cortex) 3.Medulla Lymph node Lymph Node Reticulum • Reticular stroma- reticular fibres and phagocytic reticular cells • Gives structural support to the lymphoid cells Lymph Node Reticulum Cortex Subcapsular Sinus Lymphatc Nodules Primary Nodule Secondary Nodule Germinal Centre • Paracotex: Inner cortical Zone Thymus dependent zone Lymph Node • Medulla: • Medullary Cords -Darkly stained, branching anastomosing – B Lymphocytes, plasma cells& macrophages • Medullary Sinuses- Lightly stained Lymph Node Lymph Node Lymph Node Thymus • Central Lymphoid organ • Dual Origin- Lymphoctes- Mesoderm • Reticular epithelial cells- Endoderm • Formed only by T lymphocytes • No B lymphocytes • Divided into lobules of lymphoid tissue( No lymphatic nodule) • Has hassall’s corpuscles • Produces thymic hormones • Fully dev at birth, involutes at puberty. Thymus • COMPONENTS 1. Supporting Framework Capsule Interlobular septa Cellular cytoplasmic reticulum 2. -
![Lymphoid Tissue [PDF]](https://docslib.b-cdn.net/cover/5414/lymphoid-tissue-pdf-3935414.webp)
Lymphoid Tissue [PDF]
10.03.2015 Lymphoid Tissue Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, Lucknow What is lymphoid tissue? • Specialized form of connective tissue • Supporting framework: reticular cells & reticular fibres • Large number of lymphocytes • Other cells: Plasma cells & macrophages Consists of……. • Lymphatic vessels • Specific lymphoid organs (lymph node, spleen, thymus) • Lymphatic tissue found within the tissues of other organs (in bone marrow, GI tract, urinary tract, respiratory tract) Functions • Defense of body • Phagocytosis of foreign cells • Involved in production of lymphocytes and plasma cells Lymphatic Vessels – Originate as lymph capillaries – Capillaries unite to form larger lymph vessels • Resemble veins in structure • Connect to lymph nodes at various intervals Lymphatic Capillaries Lymphatic capillary & Vessel Lymphatic Vessels Channels of Lymphatics – Lymphatics ultimately deliver lymph into 2 main channels • Right lymphatic duct –Drains right side of head & neck, right arm, right thorax –Empties into the right subclavian vein • Thoracic duct –Drains the rest of the body –Empties into the left subclavian vein Channels of Lymphatics Major Lymphatic Vessel of the Trunk Lymphatic Tissue – 3 types • Diffuse lymphatic tissue – No capsule present – Found in connective tissue of almost all organs • Lymphatic nodules – No capsule present – Oval-shaped masses – Found singly or in clusters • Lymphatic organs – Capsule present – Lymph nodes, spleen, thymus Diffuse lymphatic tissue • Called as mucosa associated lymphatic tissue (MALT). • Accumulation of lymphatic tissue in the mucous membrane of gastrointestinal, respiratory, urinary and reproductive tracts. • Located where they come in direct contact with antigens. Lymphatic Nodule • Circumscribed concentration of lymphatic tissue (lymphocytes and related cells). • Not surrounded by capsule. Lymphatic Nodule Lymphatic Organs Lymph Node – Consists of connective tissue framework & numerous lymphocytes. -

Spleen (Lec.3 )
Spleen (Lec.3 ) Spleen is largest lymphatic organ located in abdominal cavity , beneath the diaphragm. It is covered by the visceral layer of mesothelial cells (peritoneum) below it thick capsule of dense irregular connective tissue contains some smooth muscle fibers are found. Trabeculae (septa) are extended from capsule into splenic tissue. Spleen is composed of: White pulp , red pulp and marginal zone - White Pulp Is composed of: 1- branches of arteries as (central arterioles) 2- Diffused lymphatic tissue, as irregular masses around central arterioles this area is called periarterial lymphatic sheath( PALS) its lymphocytes are T- lymphocytes, so it is called (thymus-dependent area) . 3-White pulp is also composed of (dense aggregation of lymphocytes) as lymphatic nodules some with germinal center. marginal zone: The white pulp is enclosed within a layer called marginal zone. Which is an area between the red and white pulp. The periphery of the lymphatic sheath and nodules is surrounded by a marginal zone. It contains mainly B lymphocytes, plasma cells macrophages and Interdigitating, dendritic cells, marginal blood sinuses . This area plays role in (immune response & filter the blood). • Red pulp Is located between white pulp and trabeculae. • The red pulp is composed of two components : 1• Splenic cords of Billroth, and 2• Venous sinuses. Splenic cords: Are composed of a spongy cellular mass supported by reticular fibers. The collage trabeculae are continuous with the reticular fibers of the pulp. The lymphatic tissue is organized as cords or strands, contains large No. of RBC ; lymphocytes; granular leukocytes, macrophages Embedded in meshwork of reticular tissue. Venous sinuses Have large wide irregular lumen, 12-40μm wide. -
Parenchyma: Outer Cortex and Inner Medulla
Lymphatic system The lymphatic system is a drainage system it includes: 1. Lymph vessel. 2. Lymphatic tissue. Lymphatic organs Primary lymphoid Secondary lymphoid organs eg thymus organs eg spleen tonsil lymph node Lymphatic nodule • There are two types of lymphatic nodules: 1. Primary lymphatic nodules: they are aggregation of small lymphocytes without germinal centers. 2. Secondary lymphatic nodules: each consists of outer dark part and central pale part called “Germinal center”. The germinal center is the site of active lymphocyte production that appears only after birth in response to antigen exposure. The germinal center contains large lymphocytes, plasmablasts, plasma cells and macrophage cells. Capsule Trabeculae Reticular net work Lymph nodes • Lymph nodes are ovoid or kidney-shaped. • They are distributed throughout the body along the course of the lymphatic vessels. • Lymph nodes have a convex side and concave depression, the hilum, through which arteries and nerves enter and veins and lymphatic vessels leave the node. Structure: Stroma: 1. - Capsule: each lymph node is surrounded by a dense connective capsule pierced by branches of afferent lymphatic vessels. 2. - Trabeculae: they arise from the capsule and extend for variable distances into the substance of the node. 3. - Fine network of reticular fibers and reticular cells: that extends throughout the node providing a loose, supporting framework for the huge mass of lymphocytes within the lymph node. Parenchyma: outer cortex and inner medulla. 1. Cortex The cortex is formed of lymphatic tissue. It is divided by the trabeculae into regular compartments. It contains: 1. Lymphatic nodules: They are of secondary nodules and formed mainly of B lymphocytes. -

Cell Distribution Striking but Temporary Changes in Splenic
Plasmodium chabaudi chabaudi Infection in Mice Induces Strong B Cell Responses and Striking But Temporary Changes in Splenic Cell Distribution This information is current as of September 25, 2021. Ariel H. Achtman, Mahmood Khan, Ian C. M. MacLennan and Jean Langhorne J Immunol 2003; 171:317-324; ; doi: 10.4049/jimmunol.171.1.317 http://www.jimmunol.org/content/171/1/317 Downloaded from References This article cites 52 articles, 20 of which you can access for free at: http://www.jimmunol.org/content/171/1/317.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 25, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2003 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Plasmodium chabaudi chabaudi Infection in Mice Induces Strong B Cell Responses and Striking But Temporary Changes in Splenic Cell Distribution1 Ariel H. Achtman,* Mahmood Khan,† Ian C. M. MacLennan,† and Jean Langhorne2* B cells and Abs play a key role in controlling the erythrocytic stage of malaria. -
Hematolymphoid-System.Pdf
Toxicologic Pathology 2019, Vol. 47(6) 665-783 ª The Author(s) 2019 Nonproliferative and Proliferative Article reuse guidelines: sagepub.com/journals-permissions Lesions of the Rat and Mouse DOI: 10.1177/0192623319867053 journals.sagepub.com/home/tpx Hematolymphoid System 1 2,c Cynthia L. Willard-Mack, (Chair) , Susan A. Elmore , 3 4,e,g 5,f William C. Hall , Johannes Harleman , C. Frieke Kuper , 6,a 7,d,g 8,g Patricia Losco , Jerold E. Rehg , Christine Ru¨ hl-Fehlert , 9,d,g 10,b 11 Jerrold M. Ward , Daniel Weinstock , Alys Bradley , 12 13 14 Satoru Hosokawa , Gail Pearse , Beth W. Mahler , 2 15 Ronald A. Herbert , and Charlotte M. Keenan Abstract The INHAND Project (International Harmonization of Nomenclature and Diagnostic Criteria for Lesions in Rats and Mice) is a joint initiative of the Societies of Toxicologic Pathology from Europe (ESTP), Great Britain (BSTP), Japan (JSTP), and North America (STP) to develop an internationally accepted nomenclature for proliferative and nonproliferative changes in rats and mice. The purpose of this publication is to provide a standardized nomenclature for classifying changes observed in the hematolymphoid organs, including the bone marrow, thymus, spleen, lymph nodes, mucosa-associated lymphoid tissues, and other lymphoid tissues (serosa-associated lymphoid clusters and tertiary lymphoid structures) with color photomicrographs illustrating examples of the lesions. Sources of material included histopathology databases from government, academia, and industrial laboratories throughout the world. Content includes spontaneous lesions as well as lesions induced by exposure to test materials. The nomenclature for these organs is divided into 3 terminologies: descriptive, conventional, and enhanced. -
Atraumatic Splenic Rupture: Dreaded Complication of Splenomegaly
dicine & Me S l u Shiber et al., Trop Med Surg 2014, 2:1 a r ic g e p r y DOI: 10.4172/2329-9088.1000162 o r T Tropical Medicine & Surgery ISSN: 2329-9088 ReviewResearch Article Article OpenOpen Access Access ATraumatic Splenic Rupture: Dreaded Complication of Splenomegaly Joseph Shiber1*, Emily Fontane2 and David Prisk2 1Department of Medicine, Emergency Medicine and Surgical Critical Care, College of Medicine, University of Florida, USA 2Departments of Pediatrics and Emergency Medicine, College of Medicine, University of Florida, USA Abstract We discuss the causes of splenomegaly and the underlying abnormalities leading to the most feared complication of a traumatic splenic rupture. A case discussion is included. Keywords: Splenomegaly; Traumatic splenic rupture rupture since it almost always occurs in a diseased spleen due to an underlying pathologic process. A true spontaneous rupture that Case Presentation would occur without trauma and in a normal spleen is considered A 21 year-old man presented to the Emergency Department (ED) to be exceptionally rare and is still debated if it indeed occurs [2-4]. with the chief complaint of abdominal pain that radiated to his left upper Even with splenic injuries from blunt trauma there has been found back and worsened with deep inspiration. The patient was nauseous abnormal lymphocyte populations that may have contributed to the and had vomited twice. He had a sore throat for approximately one risk of rupture requiring splenectomy [2]. The definition of a truly month and had had a negative rapid streptococcal test at his student spontaneous rupture of the spleen in 1958 included: no antecedent health center.