Jordan: a Need Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
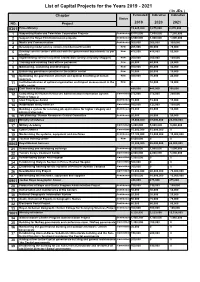
List of Capital Projects for the Years 2019 - 2021 ( in Jds ) Chapter Estimated Indicative Indicative Status NO
List of Capital Projects for the Years 2019 - 2021 ( In JDs ) Chapter Estimated Indicative Indicative Status NO. Project 2019 2020 2021 0301 Prime Ministry 13,625,000 9,875,000 8,870,000 1 Supporting Radio and Television Corporation Projects Continuous 8,515,000 7,650,000 7,250,000 2 Support the Royal Film Commission projects Continuous 3,500,000 1,000,000 1,000,000 3 Media and Communication Continuous 300,000 300,000 300,000 4 Developing model service centers (middle/nourth/south) New 205,000 90,000 70,000 5 Develop service centers affiliated with the government departments as per New 475,000 415,000 50,000 priorities 6 Implementing service recipients satisfaction surveys (mystery shopper) New 200,000 200,000 100,000 7 Training and enabling front offices personnel New 20,000 40,000 20,000 8 Maintaining, sustaining and developing New 100,000 80,000 40,000 9 Enhancing governance practice in the publuc sector New 10,000 20,000 10,000 10 Optimizing the government structure and optimal benefiting of human New 300,000 70,000 20,000 resources 11 Institutionalization of optimal organization and impact measurement in the New 0 10,000 10,000 public sector 0601 Civil Service Bureau 485,000 445,000 395,000 12 Completing the Human Resources Administration Information System Committed 275,000 275,000 250,000 Project/ Stage 2 13 Ideal Employee Award Continuous 15,000 15,000 15,000 14 Automation and E-services Committed 160,000 125,000 100,000 15 Building a system for receiving job applications for higher category and Continuous 15,000 10,000 10,000 administrative jobs. -

Jordan Middle East DISCUSSION PAPER and North Africa Transition Fund September 2017 Middle East and North Africa Transition Fund
Towards a new partnership between government and youth in Jordan Middle East DISCUSSION PAPER and North Africa Transition Fund September 2017 Middle East and North Africa Transition Fund ABOUT THE OECD MENA TRANSITION FUND OF THE DEAUVILLE PARTNERSHIP The Organisation for Economic Co-operation and Development (OECD) is an international body that promotes In May 2011, the Deauville Partnership was launched as a policies to improve the economic and social well-being long-term global initiative that provides Arab countries in of people around the world. It is made up of 35 member transition with a framework based on technical support countries, a secretariat in Paris, and a committee, drawn to strengthen governance for transparent, accountable from experts from government and other fields, for each governments and to provide an economic framework for work area covered by the organisation. The OECD provides sustainable and inclusive growth. a forum in which governments can work together to share experiences and seek solutions to common problems. We The Deauville Partnership has committed to support collaborate with governments to understand what drives Egypt, Jordan, Libya, Morocco, Tunisia and Yemen and the economic, social and environmental change. We measure Transition Fund is one of the levers to implement this productivity and global flows of trade and investment. commitment. The Transition Fund demonstrates a joint commitment by G7 members, Gulf and regional partners, For more information, please visit www.oecd.org. and international and regional financial institutions to support the efforts of the people and governments of the Partnership countries as they overhaul their economic systems to promote more accountable governance, broad- based, sustainable growth, and greater employment opportunities for youth and women. -

Women's Political Participation in Jordan
MENA - OECD Governance Programme WOMEN’S Political Participation in JORDAN © OECD 2018 | Women’s Political Participation in Jordan | Page 2 WOMEN’S POLITICAL PARTICIPATION IN JORDAN: BARRIERS, OPPORTUNITIES AND GENDER SENSITIVITY OF SELECT POLITICAL INSTITUTIONS MENA - OECD Governance Programme © OECD 2018 | Women’s Political Participation in Jordan | Page 3 OECD The mission of the Organisation for Economic Co-operation and Development (OECD) is to promote policies that will improve the economic and social well-being of people around the world. It is an international organization made up of 37 member countries, headquartered in Paris. The OECD provides a forum in which governments can work together to share experiences and seek solutions to common problems within regular policy dialogue and through 250+ specialized committees, working groups and expert forums. The OECD collaborates with governments to understand what drives economic, social and environmental change and sets international standards on a wide range of things, from corruption to environment to gender equality. Drawing on facts and real-life experience, the OECD recommend policies designed to improve the quality of people’s. MENA - OECD MENA-OCED Governance Programme The MENA-OECD Governance Programme is a strategic partnership between MENA and OECD countries to share knowledge and expertise, with a view of disseminating standards and principles of good governance that support the ongoing process of reform in the MENA region. The Programme strengthens collaboration with the most relevant multilateral initiatives currently underway in the region. In particular, the Programme supports the implementation of the G7 Deauville Partnership and assists governments in meeting the eligibility criteria to become a member of the Open Government Partnership. -

THE STARTUP GUIDE Business in Jordan
Your complete guide to registering and licensing a small THE STARTUP GUIDE business in Jordan Find out what to do, where to go and what fees are required to formalize your small business in this simple, step-by-step guide Contents WHY SHOULD I REGISTER AND LICENSE MY BUSINESS? ........................................................................................ 2 WHAT ARE THE STEPS I NEED TO TAKE IN ORDER TO FORMALIZE MY BUSINESS? ............................................... 3 HOW DO I KNOW WHAT TYPE OF BUSINESS TO REGISTER? ................................................................................. 4 HOW DO I CHOOSE A BUSINESS STRUCTURE THAT’S RIGHT FOR ME? ................................................................. 6 I’VE CHOSEN MY BUSINESS STRUCTURE… WHAT NEXT? ...................................................................................... 8 I’VE GOTTEN MY PRE-APPROVALS. HOW DO I REGISTER MY BUSINESS? ............................................................. 9 A) REGISTERING AN INDIVIDUAL ESTABLISHMENT ........................................................................................ 10 B) REGISTERING A GENERAL PARTNERSHIP OR LIMITED PARTNERSHIP COMPANY ...................................... 13 C) REGISTERING A LIMITED LIABILITY COMPANY ........................................................................................... 16 D) REGISTERING A PRIVATE SHAREHOLDING COMPANY................................................................................ 20 I’VE REGISTERED MY BUSINESS. HOW CAN I SET -

Intention to Use Contraceptives in Jordan
Intention to Use Contraceptives in Jordan: Further Analysis of the Jordan Population and Family Health Survey 2017-18 DHS Further Analysis Reports No. 141 December 2020 This publication was produced for review by the United States Agency for International Development. It was prepared by Sara Riese. Further Analysis Reports No. 141 Intention to Use Contraceptives in Jordan: Further Analysis of the Jordan Population and Family Health Survey 2017-18 Sara Riese1,2 ICF Rockville, Maryland, USA December 2020 1 ICF 2 The DHS Program Corresponding author: Sara Riese, International Health and Development, ICF, 530 Gaither Road, Suite 500, Rockville, MD 20850, USA; phone: +1 301-572-0546; fax: +1 301-407-6501; email: [email protected] Acknowledgments: This study was supported by the USAID/Jordan. The USAID Mission in Jordan provided support and funding under the DHS-8 contract. Many thanks to my colleague, Christina Juan, for brainstorming and discussions during the Jordan Further Analysis report development process. Gratitude is extended to Shireen Assaf and Yodit Bekele for their thoughtful review and comments, as well as to our external reviewers, Hana Banat, John Callanta, and Samah Al-Quran. Editor: Diane Stoy Document Production: Natalie Shattuck This report presents findings from a further analysis of the 2017-18 Jordan Population and Family Health Survey (JPFHS). This report is a publication of The DHS Program which collects, analyzes, and disseminates data on fertility, family planning, maternal and child health, nutrition, and HIV/AIDS. Funding was provided by the U.S. Agency for International Development (USAID) through the DHS Program (#720-0AA-18C-00083). -
Distrubition System Plan
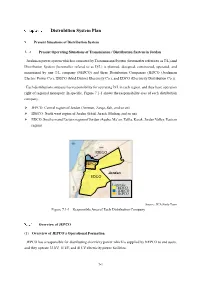
Distrubition System Plan Present Situations of Distribution System Present Operating Situations of Transmission / Distribution System in Jordan Jordanian power system which is consisted by Transmission System (hereinafter refered to as T/L) and Distribution System (hereinafter refered to as D/L) is planned, designed, constructed, operated, and maintained by one T/L company (NEPCO) and three Distribution Companies (JEPCO (Jordanian Electric Power Co.), IDECO (Irbid District Electricity Co.), and EDCO (Electricity Distribution Co.)). Each distribution company has responsibility for operating D/L in each region, and they have operation right of regional monopoly. In specific, Figure 7.1-1 shows the responsibility area of each distribution company. JEPCO: Central region of Jordan (Amman, Zarqa, Salt, and so on) IDECO: North west region of Jordan (Irbid, Jarash, Mufraq, and so on) EDCO: Southern and Eastern region of Jordan (Aqaba, Ma’an, Tafila, Karak, Jordan Valley, Eastern region) IDECO JEPCO Jordan EDCO Legends: ■:EDCO ■:IDECO ■:JEPCO Source: JICA Study Team Figure 7.1-1 Responsible Area of Each Distribution Company Overview of JEPCO (1) Overview of JEPCO’s Operational Formation JEPCO has a responsible for distributing electricity power which is supplied by NEPCO to end users, and they operate 33 kV, 11 kV, and 415 V electricity power facilities. 7-1 Headquarters of JEPCO is located in Amman, and they operate the distribution facilities from secondary side bus of each BSP to terminals of end user. Organization chart of JEPCO is shown in Figure 7.1-2. JEPCO buys the electricity power from NEPCO, and the boundary point of trading is secondary side of BSP. -

Role of King Abdullah II Fitness Award in Improving the Physical Level of the Tenth Grade from the Point of View of Teachers in the Northern Governorates
Journal of Education and Practice www.iiste.org ISSN 2222-1735 (Paper) ISSN 2222-288X (Online) Vol.7, No.20, 2016 Role of King Abdullah II Fitness Award in Improving the Physical Level of the Tenth Grade from the Point of View of Teachers in the Northern Governorates Dr.Hamed Mohammed Doum Associate professor -Department of Educational Sciences, Ajloun University College, AL-Balqa Applied University. JORDAN Abstract The study aimed to identify the role of King Abdullah II fitness award in improving the physical level to the tenth grade from the point of view of teachers in the of Northern region governates. The researcher used the descriptive survey method for its suitability to the objectives of the study, the researcher built a questionnaire that consisted of (20) items and confirmed its validity and reliability, a sample of 183 teachers were chosen from the northern governorates (Irbid, Ajloun, Jerash). The results showed a high degree to the role of King Abdullah fitness award in improving the physical level of the tenth grade in the north northern governorates. And that there were no statistically significant differences at the level of (0.05) for the role of King Abdullah fitness award in improving the physical level to the tenth grade in the Northern Governorates according to the variables of (gender, scientific expertise, qualification). The study suggested some recommendations like giving importance to the award implementation, encouraging the students towards fitness exercise to improve their physical level, raising awareness among all students and teachers of the importance of the award. Keywords : King Abdullah award, fitness, physical level. -

Jordan: Ajloun Governorate Reference Map
Jordan: Ajloun Governorate Reference Map Taibeh Taibeh Dair Ess'eneh Rkhayyem Bait Yafa Irbid Irbid Jinien Essafa Iskayeen Sammo' Shaikh Hussein Alyah Aidoon Ham Natfeh Abu Ziyad Kofor Kiefia Sarieh Zmal Zamaliyyeh Dair Abi Sa'id Johfiyyeh Diar Yoosef Hoafa El-Mazar Jeffien Sowwan Kofor El-Ma' Enbeh Hoson Abu El-Qain Tebneh Habka Mazar Shamali Raqqah Kora Kora Ashrafiyyeh Mazar Ash-shamali Mazar Ash-shamali Bani ObaidBani Obaid Kofor Rakeb Samad Rahmah Tabaqat Fahl Mashari'e Ibrahimiyyeh (Sarras) Za'tara Bait Iedes Ketem Zoobya dir al birak Kherbet El-Hawi Rhaba Shatana Kofor Owan Ghwar Ashamalya Ghwar Ashamalya NULL Marzeh Kofor Abiel Jdaitta NULL NULL Rahwah Bier Eddalyeh NULL NULL Arjan Samta Halawah Ras Munif NULL Sakhera NULL NULL Sakhrah Tayyarah Mehnah Hashemiyyeh NULL Kofor Khall NULL Ebbien Karkamah Shtafaina Sbiereh Ajloun Ebellien NULL Dair Smadiyyeh Shamali NULL souan Qarn Dair Smadiyyeh Janoobi Ain Janna Sakhneh NULL Ajloun Ajloun Slaikhat Ajloun Wahadneh JORDAN Meqebleh Soof Anjarah Mukhayyam Soof Kofranjah Jerash Shkarah NULL Jarash NULL Riemoon Sakeb Berkeh NULL Zaqreet Wahadneh Oqdeh NULL Nahleh Krayymeh Um Erramel Harth balass MukhayyMaman Gshiayzyzeet hHashem Nubah Sofsafah Haddadeh Khellet Wardeh Um El-Yanabi'e Jamla Safieneh Kellet Salem Sakhneh NULL Fakhreh Zarra'ah kaeb al maloul Jerash Kofranja Kofranja Rashaydeh balass Shkarah Najdeh Amameh Rasoon Balawneh thaghret zbad Oasarah Gabal Aghdar Keshiebeh El-Foqa' Merjam Berma Erjan Hooneh Khazma Mansoorah (khshaibeh) Fawara Sena'ar Dherar Mashtal Faisal Shaikh Mefrej -

Preparatory Survey Report on the Project for Improvement of Waste Management Equipment in Northern Region Hosting Syrian Refugees in the Hashemite Kingdom of Jordan
Ministry of Municipal Affairs (MOMA) The Hashemite Kingdome of Jordan PREPARATORY SURVEY REPORT ON THE PROJECT FOR IMPROVEMENT OF WASTE MANAGEMENT EQUIPMENT IN NORTHERN REGION HOSTING SYRIAN REFUGEES IN THE HASHEMITE KINGDOM OF JORDAN OCTOBER 2017 JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) KOKUSAI KOGYO CO., LTD. GE JR 17-115 The exchange rate used in this report is as follows US$ 1.0 = 115.63 Yen, 1 EURO = 123.08 Yen, 1 JD = 162.58 Yen (Average rate of three months from Dec 2016, Jan and Feb 2017) Summary 1. Outline of the Country (1) Land and Nature Jordan, formally known as the Hashemite Kingdome of Jordan, has an area of about 89,000 km2, surrounded by Syria on the north and Iraq, Saudi Arabia and Israel in a clockwise order. Its coastline is only 15 km on the south end facing the Gulf of Aqaba. The Jordan Valley, which forms the northern tip of the African Great Rift Valley, runs in the west of the country from south to north and is famous for the world’s lowest elevation at 200 to 400 meters below sea level. Being warm in winter and hot in summer, the area is prosperous in irrigated agriculture. To the east are hilly plateaus of Mediterranean climate with some peaks over 1,500 m high. In the hilly plateaus in winter, sometimes there is snowfall that makes the passage of vehicles difficult. Further to the east is desert, which covers as much as 80% of the country. Its southeast part is extremely dry as the yearly rainfall can be less than 35 mm. -
Governorates Budgets According to the Determined Ceiling
Total of Capital Expenditures Distributed According to the Determined Ceilings for the Fiscal Year 2018 ( In JDs ) Expenditures of GOVERNORATE Sustaining the Capital Total Work of the Expenditures Governorates Councils Irbid Governorate 372,000 22,981,000 23,353,000 Mafraq Governorate 325,000 18,952,000 19,277,000 Jerash Governorate 176,000 14,974,000 15,150,000 Ajloun Governorate 189,000 15,818,000 16,007,000 The Capital Governorate 474,000 34,464,000 34,938,000 Balqa' Governorate 216,000 16,400,000 16,616,000 Zarqa Governorate 284,000 20,322,000 20,606,000 Ma'daba Governorate 162,000 13,691,000 13,853,000 Karak Governorate 230,000 14,361,000 14,591,000 Ma'an Governorate 162,000 19,121,000 19,283,000 Tafileh Governorate 155,000 13,785,000 13,940,000 Aqaba Governorate 155,000 15,131,000 15,286,000 Total 2,900,000 220,000,000 222,900,000 Budget Summary of Irbid Governorate for the Years 2018 - 2020 ( In JDs) Description Estimated Indicative Indicative 2018 2019 2020 Expenditures of Sustaining the Work of the Governorate Council 372,000 385,000 385,000 Capital Expendituers 22,981,000 23,967,000 25,733,000 Total 23,353,000 24,352,000 26,118,000 Appropriations of Sustaining the Council Work of Irbid Governorate for the Years 2018 - 2020 ( In JDs) Description Estimated Indicative Indicative 2018 2019 2020 001 Council of Irbid Governorate 372,000 385,000 385,000 001 Bonuses 312,000 312,000 312,000 004 Hospitality 3,900 3,900 3,900 999 Others 56,100 69,100 69,100 Total 372,000 385,000 385,000 Capital Budget for Irbid Governorate for the years -

Determinants of Human Security and Hard Security in Ajloun
Determinants of Human Security and Hard Security in Ajloun West Asia-North Africa Institute, April 2019 This project is led by the WANA Institute, funded through the Netherlands Organisation for Scientific Research (NWO-WOTRO), commissioned by the Ministry of Foreign Affairs of The Netherlands, and developed in close collaboration with the Knowledge Platform Security & Rule of Law. This publication reflects the views of the authors only, and not necessarily that of NWO. PERMISSION TO REPRODUCE The information in this publication may not be reproduced, in part or in whole and by any means, without charge or further permission from the WANA Institute. For permission to reproduce the information in this publication, please contact the WANA Institute Communications Department at [email protected]. Published by the WANA Institute, Royal Scientific Society in Amman, Jordan Authors: Dr Neven Bondokji, Barik Mhadeen, Lina AlHaj Translation: Project Tarjim Cover Design: Hadeel Qatamin Printed in Amman, Jordan © 2019 WANA Institute. All rights reserved. Manufactured in Jordan Human Security or State-Centric Security Approaches in Ajloun TABLE OF CONTENTS 1. Introduction .............................................................................................................................................. 3 2. Human Security and State-Centric Security ......................................................................................... 4 2.1 Citizens and Security Officers ........................................................................................................ -

Emerging Trends in the Jordanian Host Community
Journal of Sociology and Social Work December 2019, Vol. 7, No. 2, pp. 115-125 ISSN: 2333-5807 (Print), 2333-5815 (Online) Copyright © The Author(s). All Rights Reserved. Published by American Research Institute for Policy Development DOI: 10.15640/jssw.v7n2a12 URL: https://doi.org/10.15640/jssw.v7n2a12 Emerging trends in the Jordanian Host Community: Service Delivery Gaps, Ethnographic Shifts and Social Tension: a Field Study in the Governorates of Jerash and Ajloun Dr. Basem Al Atom1 Abstract This field research study examines the underlying causes of social tension between Syrian refugees and the Jordanian host community in Northern Jordan. It does so, moreover, within the framework of the current shift being undertaken by international and local non-governmental organizations from an emergency response to Syrian refugees to a development response. Specifically, such a shift brings with it an increased focus on livelihoods as a means of sustainable economic empowerment. With a focus on livelihoods, however, comes an increase in the potential for tension between employers and employees. Furthermore, this tension complements an already-existing tension that exists between landlords and tenants. Understanding the sources of these types of conflict will help mitigate against future tensions and better facilitate social cohesion amongst Syrian refugees and the Jordanian host community. Keywords: Syrian refugees, host communities, social cohesion, social tension, dispute resolution 1. Introduction This research study provides an overview and analysis of research undertaken between February 2018 and April 2018. The purpose of this report is to examine the underlying causes of social tension between Syrian refugees and the Jordanian host community in Northern Jordan, and to help mitigate against future tensions and better facilitate social cohesion between these two communities.