1 Pathology Week X
Total Page:16
File Type:pdf, Size:1020Kb
Recommended publications
-

General Pathomorpholog.Pdf
Ukrаiniаn Medicаl Stomаtologicаl Аcаdemy THE DEPАRTАMENT OF PАTHOLOGICАL АNАTOMY WITH SECTIONSL COURSE MАNUАL for the foreign students GENERАL PАTHOMORPHOLOGY Poltаvа-2020 УДК:616-091(075.8) ББК:52.5я73 COMPILERS: PROFESSOR I. STАRCHENKO ASSOCIATIVE PROFESSOR O. PRYLUTSKYI АSSISTАNT A. ZADVORNOVA ASSISTANT D. NIKOLENKO Рекомендовано Вченою радою Української медичної стоматологічної академії як навчальний посібник для іноземних студентів – здобувачів вищої освіти ступеня магістра, які навчаються за спеціальністю 221 «Стоматологія» у закладах вищої освіти МОЗ України (протокол №8 від 11.03.2020р) Reviewers Romanuk A. - MD, Professor, Head of the Department of Pathological Anatomy, Sumy State University. Sitnikova V. - MD, Professor of Department of Normal and Pathological Clinical Anatomy Odessa National Medical University. Yeroshenko G. - MD, Professor, Department of Histology, Cytology and Embryology Ukrainian Medical Dental Academy. A teaching manual in English, developed at the Department of Pathological Anatomy with a section course UMSA by Professor Starchenko II, Associative Professor Prylutsky OK, Assistant Zadvornova AP, Assistant Nikolenko DE. The manual presents the content and basic questions of the topic, practical skills in sufficient volume for each class to be mastered by students, algorithms for describing macro- and micropreparations, situational tasks. The formulation of tests, their number and variable level of difficulty, sufficient volume for each topic allows to recommend them as preparation for students to take the licensed integrated exam "STEP-1". 2 Contents p. 1 Introduction to pathomorphology. Subject matter and tasks of 5 pathomorphology. Main stages of development of pathomorphology. Methods of pathanatomical diagnostics. Methods of pathomorphological research. 2 Morphological changes of cells as response to stressor and toxic damage 8 (parenchimatouse / intracellular dystrophies). -

Classification of Thyroid Tumors Benign Tumors - Adenoma 1
DERMATOPATHOLOGY PATHOLOGY OF ENDOCRINE SYSTEM Thyroid carcinoma, Hashimoto thyroiditis, Graves‘ disease, neuroendocrine tumor, Institute of Pathological Anatomy melanoma, pigmented naevus, psoriasis, eczema FM CU BA DERMATOPATHOLOGY • 10-year-old boy with a pigmented lesion on his shoulder, sharply demarcated from the surrounding skin, with a diameter of 2.3 cm, dark brown in color, without noticeable changes. CASE NO. 1 ➢Suggested examinations? ➢Your diagnosis? ➢Describe the microscopic finding. Pigmented nevus of the skin Congenital pigmented nevus of the skin PIGMENTED NEVUS • benign skin formation arising as a result of melanocyte accumulation • the most common skin lesion of the white race • most nevi form in childhood and adolescence Classification of nevi according to the position of growth in the skin • Junctional nevus - nests of melanocytes are found at the dermo-epidermal junction • Mixed nevus - nests of melanocytes are found at the junction but also in the dermis • Intradermal nevus - clusters of melanocytes are found in the upper part of the dermis WITHOUT connection with the epidermis Histological variants of pigmented nevus • Congenital nevus • Blue nevus • Halo nevus • Familial dysplastic nevus Mixed pigmented nevus Junctional pigmented nevus Intradermal pigmented nevus • 73-year-old patient was admitted to hospital for progressive weakness, shortness of breath. You notice that both the skin and the sclera are icteric. • laboratory hyperbilirubinemia, hypoalbuminemia and mineral imbalance, positive oncomarkers (S100) • abdominal ultrasound with spherical structures found in the liver parenchyma • personal medical history - malignant melanoma of the eye CASE NO. 2 30 years ago, CLL 3 years ago, now in remission ➢Suggested examinations? ➢Your diagnosis? ➢Complications? ➢Describe the microscopic finding. -

Spontaneous Regression of Divided Nevus of the Eyelid Evaluated by Dermoscopy Leaving a Hypopigmented Lesion
Case Report Spontaneous regression of divided nevus of the eyelid evaluated by dermoscopy leaving a hypopigmented lesion Danang Tri Wahyudi1, Izzah Aulia2, Aida S.D. Hoemardani1, Agassi Suseno Sutarjo1 1. Department of Dermatology and Venereology, Dharmais National Cancer Hospital, Jakarta, Indonesia 2. Department of Dermatology and Venereology Faculty of Medicine Universitas Indonesia/ Dr. Cipto Mangunkusumo National Central General Hospital Jakarta, Indonesia Email: [email protected] Abstract Background: Divided nevus, also known as “kissing nevus,” is a rare form of congenital melanocytic nevus that occurs on opposing margins of upper and lower eyelids. A paucity of literature on this rare anomaly exists, with most being case reports and series. Moreover, regression of this lesion was rarely reported. Case Illustration: We present a rare case of congenital divided nevus of the eyelid that regressed after eight years, confirmed with dermoscopy. A siX-year-old boy presented to the Dharmais National Cancer Hospital with two pigmented macules on the upper and lower right eyelid since birth. A year ago, the lesions started gradually disappearing and were replaced by a hypopigmented area. We evaluated the clinical and dermoscopic findings for two consecutive years. The dermoscopy showed pseudopigment networks, surrounded by a hypopigmented area resembling a halo. The pigmented lesions cleared with no residual lesions. Discussion: The dermoscopic findings of the patient resemble a solar lentigo characterized by pseudopigment networks, a feature caused by the relatively flattened rete ridge on the face. The hypopigmented area reflects a regression process, like the halo nevus, and is accompanied by leukotrichia of the eyelashes, a feature usually found in patients with vitiligo. -

Clinical Dermatology Notice
This page intentionally left blank Clinical Dermatology Notice Medicine is an ever-changing science. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy are required. The editors and the publisher of this work have checked with sources believed to be reliable in their efforts to provide information that is complete and generally in accord with the standards accepted at the time of publication. However, in view of the possibility of human error or changes in medical sciences, neither the editors nor the publisher nor any other party who has been involved in the preparation or publication of this work warrants that the information contained herein is in every respect accurate or complete, and they disclaim all responsibility for any errors or omissions or for the results obtained from use of such information contained in this work. Readers are encouraged to confirm the information contained herein with other sources. For example and in particular, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this work is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs. a LANGE medical book Clinical Dermatology Carol Soutor, MD Clinical Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota Maria K. Hordinsky, MD Chair and Professor Department of Dermatology University of Minnesota Medical School Minneapolis, Minnesota New York Chicago San Francisco Lisbon London Madrid Mexico City Milan New Delhi San Juan Seoul Singapore Sydney Toronto Copyright © 2013 by McGraw-Hill Education, LLC. -

Photo Diagnosis
Photo Diagnosis Illustrated quizzes on problems seen in everyday practice Case 1 An 11-year-old boy presents with pain over the left clavicle after falling from an eight-foot high ladder and landing on a outstretched left hand. Questions 1. What is the diagnosis? 2. What is the significance? Answers 1. Fractured left clavicle. 2. The majority of clavicular fractures heal spontaneously through callus formation. Immobilization of the affected arm for pain control can be easily and effectively accomplished by an arm sling. A figure-of-eight splint offers no advantage over the sling and can be uncomfortable for some children. Inappropriate use of the splint may occasionally even lead to edema of the ipsilateral upper limb, compression of axillary vessels and brachial plexopathy. Provided by Dr. Alexander K.C. Leung; and Dr. Justine H.S. Fong, Calgary, Alberta. Share your photos and diagnoses with us! Do you have a photo diagnosis? Send us your photo and a brief text explaining the presentation of the illness, your diagnosis and treatment, and receive $25 per item if it is published. The Canadian Journal of Diagnosis 955, boul. St. Jean, suite 306, Pointe-Claire (Quebec) H9R 5K3 E-mail: [email protected] Fax: (514) 695-8554 The Canadian Journal of Diagnosis / January 2005 47 Photo Diagnosis Case 2 A 32-year-old former soccer player presents with recurrent attacks of excruciating pain in the right first metatarsophalangeal joint. The attacks have been occurring for the past six months. Questions 1. What is the diagnosis? 2. What is the significance? 3. What is the treatment? Answers 1. -

Wednesday Slide Conference 2008-2009
PROCEEDINGS DEPARTMENT OF VETERINARY PATHOLOGY WEDNESDAY SLIDE CONFERENCE 2008-2009 ARMED FORCES INSTITUTE OF PATHOLOGY WASHINGTON, D.C. 20306-6000 2009 ML2009 Armed Forces Institute of Pathology Department of Veterinary Pathology WEDNESDAY SLIDE CONFERENCE 2008-2009 100 Cases 100 Histopathology Slides 249 Images PROCEEDINGS PREPARED BY: Todd Bell, DVM Chief Editor: Todd O. Johnson, DVM, Diplomate ACVP Copy Editor: Sean Hahn Layout and Copy Editor: Fran Card WSC Online Management and Design Scott Shaffer ARMED FORCES INSTITUTE OF PATHOLOGY Washington, D.C. 20306-6000 2009 ML2009 i PREFACE The Armed Forces Institute of Pathology, Department of Veterinary Pathology has conducted a weekly slide conference during the resident training year since 12 November 1953. This ever- changing educational endeavor has evolved into the annual Wednesday Slide Conference program in which cases are presented on 25 Wednesdays throughout the academic year and distributed to 135 contributing military and civilian institutions from around the world. Many of these institutions provide structured veterinary pathology resident training programs. During the course of the training year, histopathology slides, digital images, and histories from selected cases are distributed to the participating institutions and to the Department of Veterinary Pathology at the AFIP. Following the conferences, the case diagnoses, comments, and reference listings are posted online to all participants. This study set has been assembled in an effort to make Wednesday Slide Conference materials available to a wider circle of interested pathologists and scientists, and to further the education of veterinary pathologists and residents-in-training. The number of histopathology slides that can be reproduced from smaller lesions requires us to limit the number of participating institutions. -

Pathology of Soft Tissue and Skin. Bone and Joint Pathology. Pathology of Soft Tissue and Skin
Pathology of soft tissue and skin. Bone and joint pathology. Pathology of soft tissue and skin. Bone and joint pathology. I.Microspecimens: № 188. Capillary hemangioma. (H.E. stain). Indications: 1. Epidermis. 2. Dermis 3. Spindle cells arranged compactly with spaces containing blood. 4. Reduced connective stroma. In the microspecimen is presented a well-defined subepidermal tumoral node, consisting of proliferating capillary blood vessels, poor loose stroma; epidermis with normal histological structure. Hemangioma is a benign tumor of vascular origin, histological variants are capillary, venous and cavernous hemangioma. It is located mainly in the skin, the mucosa of the gastrointestinal tract, the liver. Capillary hemangioma is the most common benign tumor in children and has a disembryoplazic character, being interpreted as a hamartoma - a tumor from the embryonic tissues. Macroscopically it has the appearance of a red-purple node or plaque. Cutaneous hemangiomas can be complicated by exulceration, bleeding, the association of secondary infection. 3 2 4 1 № 188. Capillary hemangioma. (H.E. stain). № 43. Fibrosarcoma. (H.E. stain). Indications: 1.Epidermis. 2.Dermis. 3.Atypical tumor cells (fibroblast-like). 4.Bundles of collagen fibers. In the skin, under the epidermis there is a rich cellular tumoral node, consisting of predominantly spindle-shaped cells, of the fibroblasts type, arranged in bundles, which intersect in different directions, the tumor has no precise limits, many mitoses, giant cells, foci of necrosis, hemorrhage, stroma is poor. Fibrosarcoma is a malignant tumor, which derives from fibroblasts, may have different degrees of differentiation. It is found in adults between the ages of 40 and 70, located more frequently in the deep tissues of the hip, knee, in the retroperitoneal area. -

Dermoscopy Patterns of Halo Nevi
OBSERVATION Dermoscopy Patterns of Halo Nevi Isabel Kolm, MD; Alessandro Di Stefani, MD; Rainer Hofmann-Wellenhof, MD; Regina Fink-Puches, MD; Ingrid H. Wolf, MD; Erika Richtig, MD; Josef Smolle, MD; Helmut Kerl, MD; H. Peter Soyer, MD; Iris Zalaudek, MD Background: Halo nevi (HN) are benign melanocytic globular and/or homogeneous patterns in more than 80% nevi surrounded by a depigmented area (halo). This study of HN. Follow-up of 33 HN revealed considerable size aims to evaluate the dermoscopic features of HN and their reduction of the nevus component, but this was not as- changes during digital dermoscopic follow-up and to in- sociated with significant structural changes. Of a total of vestigate the frequency of the halo phenomenon in a se- 475 melanomas, only 2 revealed an encircling halo, but ries of melanomas. both displayed clear-cut melanoma-specific patterns ac- cording to dermoscopy. Observations: In a retrospective study, digital dermo- scopic images of HN from patients who attended the Pig- Conclusions: Halo nevi exhibit the characteristic der- mented Skin Lesions Clinic of the Department of Der- moscopic features of benign melanocytic nevi, repre- matology, Medical University of Graz, between October sented by globular and/or homogeneous patterns that are 1, 1997, and March 31, 2004, were reviewed and classi- typically observed in children and young adults. Halo nevi fied by dermoscopic morphologic criteria. For HN that reveal considerable changes of area over time during digi- were followed up with digital dermoscopy, the percent- tal dermoscopic follow-up, albeit their structural pat- ages of changes in the size of the nevus and halo com- terns remain unchanged. -

Tern, It Was Felt of Use to Record the Experience in This Matter
PERSISTENT "INSECT BITES" (DERMAL EOSINOPHILIC GRANU- LOMAS) SIMULATING LYMPHOBLASTOMAS, HISTIOCYTOSES, AND SQUAMOUS CELL CARCINOMAS * ARrHUR C. ALLEN, MD. t (From the Army instute of Pathology, Washingtox 25, D.C.) In 1942, opportunity was afforded at the Army Institute of Pathol- ogy to review the histologic slides of a lesion said to have been pro- duced by a tick bite. The microscopic sections seemed at the time indistinguishable from mycosis fungoides or Hodgkin's disee, espe- cialy in view of the presence of multiple lesions in the patient. How- ever, following the study of the cutaneous reactions to arthropods (ticks, mosquitoes, and chiggers), it was quickly appreciated that not only were these diagnoses of neoplasia wrong but that the misinterpretation of these reactions was a common and serious error.' The errors in- volved the misconstruction not only of the dermal reaction but also of the epidermal changes. The latter response was confused with squa- mous cell carcinoma; the dermal infitrate was mistaken for mycosis fungoides, Hodgkin's disease, lymphosacoma, giant follicular lympho- blastoma, and Spiegler-Fendt sarcoid. Undoubtedly the principal rea- son for the failure to attnbute these reactions properly to bites of arachnida and insects was referable to the general impression, despite dear-cut cinical histories, that such reactions last only for days, whereas, in truth, they may persist for as long as 2 years. More re- cently, the problem has been further complicated by introduction into the literature of a lesion called "eosinophilic granuloma of skin," an entity of questionable nosologic justification.' Therefore, because of the major importance of establishing a definitive diagnosis and because of the interest in the pathogenesis of a much mimicked histologic pat- tern, it was felt of use to record the experience in this matter. -

(12) United States Patent (10) Patent No.: US 7,359,748 B1 Drugge (45) Date of Patent: Apr
USOO7359748B1 (12) United States Patent (10) Patent No.: US 7,359,748 B1 Drugge (45) Date of Patent: Apr. 15, 2008 (54) APPARATUS FOR TOTAL IMMERSION 6,339,216 B1* 1/2002 Wake ..................... 250,214. A PHOTOGRAPHY 6,397,091 B2 * 5/2002 Diab et al. .................. 600,323 6,556,858 B1 * 4/2003 Zeman ............. ... 600,473 (76) Inventor: Rhett Drugge, 50 Glenbrook Rd., Suite 6,597,941 B2. T/2003 Fontenot et al. ............ 600/473 1C, Stamford, NH (US) 06902-2914 7,092,014 B1 8/2006 Li et al. .................. 348.218.1 (*) Notice: Subject to any disclaimer, the term of this k cited. by examiner patent is extended or adjusted under 35 Primary Examiner Daniel Robinson U.S.C. 154(b) by 802 days. (74) Attorney, Agent, or Firm—McCarter & English, LLP (21) Appl. No.: 09/625,712 (57) ABSTRACT (22) Filed: Jul. 26, 2000 Total Immersion Photography (TIP) is disclosed, preferably for the use of screening for various medical and cosmetic (51) Int. Cl. conditions. TIP, in a preferred embodiment, comprises an A6 IB 6/00 (2006.01) enclosed structure that may be sized in accordance with an (52) U.S. Cl. ....................................... 600/476; 600/477 entire person, or individual body parts. Disposed therein are (58) Field of Classification Search ................ 600/476, a plurality of imaging means which may gather a variety of 600/162,407, 477, 478,479, 480; A61 B 6/00 information, e.g., chemical, light, temperature, etc. In a See application file for complete search history. preferred embodiment, a computer and plurality of USB (56) References Cited hubs are used to remotely operate and control digital cam eras. -

Buffalo Medical Group, P.C. Robert E
Buffalo Medical Group, P.C. Robert E. Kalb, M.D. Phone: (716) 630-1102 Fax: (716) 633-6507 Department of Dermatology 325 Essjay Road Williamsville, New York 14221 2 FOOT- 1 HAND SYNDROME 2 foot - 1 hand syndrome is a superficial infection of the skin caused by the common athlete's foot fungus. It is quite common for people to have a minor amount of an athlete's foot condition. This would appear as slight scaling and/or itching between the toes. In addition, patients may have thickened toenails as part of the athlete's foot condition. Again the problem on the feet is very common and often patients are not even aware of it. In some patients, however, the athlete's foot fungus can spread to another area of the body. For some strange and unknown reason, it seems to affect only one hand. That is why the condition is called 2 foot - 1 hand syndrome. It is not clear why the problem develops in only one hand or why the right or left is involved in some patients. Fortunately there is very effective treatment to control this minor skin problem. If the problem with the superficial fungus infection is confined to the skin, then a short course of treatment with an oral antibiotic is all that is required. This antibiotic is very safe and normally clears the skin up fairly rapidly. It is often used with a topical cream to speed the healing process. If, however, the fingernails of the affected hand are also involved then a more prolonged course of the antibiotic will be necessary. -
WSC 13-14 Conf 13 Layout
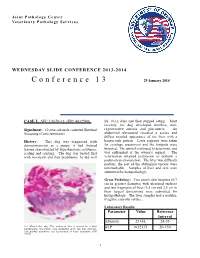
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2013-2014 Conference 13 29 January 2014 CASE I: AVC C3670-13 (JPC 4032590). for 10-12 days and then stopped eating. Most recently, the dog developed diarrhea, non- Signalment: 10-year-old male castrated Shetland regenerative anemia and glucosuria. An Sheepdog (Canis familiaris). abdominal ultrasound revealed a severe and diffuse mottled appearance of the liver with a History: This dog was diagnosed with honeycomb pattern. Liver aspirates were taken dermatomyositis as a puppy; it had footpad for cytology assessment and the footpads were lesions characterized by hyperkeratosis, erythema, biopsied. The animal continued to deteriorate and scaling and crusting. The dog was treated first was euthanized at the owner’s request. The with novalexin and then prednisone; he did well veterinarian obtained permission to perform a postmortem examination. The liver was diffusely nodular; the rest of the abdominal viscera were unremarkable. Samples of liver and skin were submitted for histopathology. Gross Pathology: Two punch skin biopsies (0.7 cm in greatest diameter) with ulcerated surfaces and two fragments of liver (3.5 cm and 2.5 cm in their largest dimension) were submitted for histopathology. The liver samples had a nodular, irregular, capsular surface. Laboratory Results: Parameter Value Reference Interval Albumin 23 G/L 24-55 1-1. Haired skin, dog: This section of skin is covered by a thick parakeratotic serocellular crust (extending down into hair follicles), ALP 1632 U/L 20-150 with marked acanthosis and hyperplasia of basal epithelium. (HE 0.63X) 1 WSC 2013-2014 ALT 442 U/L 10-118 Glucose 9.2 mmol/L 3.3-6.1 WBC 19.1 x 103/ 6.0-17.0 mm3 segmented 94% lymphocytes 3% monocytes 2% bands 1% RBC 4.12 x 106/ 5.50-8.50 mm3 urine glucose 3+ 1-2.