Annual Health Report 2075/76
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -

Japan International Cooperation Agency (JICA)
Chapter 3 Project Evaluation and Recommendations 3-1 Project Effect It is appropriate to implement the Project under Japan's Grant Aid Assistance, because the Project will have the following effects: (1) Direct Effects 1) Improvement of Educational Environment By replacing deteriorated classrooms, which are danger in structure, with rainwater leakage, and/or insufficient natural lighting and ventilation, with new ones of better quality, the Project will contribute to improving the education environment, which will be effective for improving internal efficiency. Furthermore, provision of toilets and water-supply facilities will greatly encourage the attendance of female teachers and students. Present(※) After Project Completion Usable classrooms in Target Districts 19,177 classrooms 21,707 classrooms Number of Students accommodated in the 709,410 students 835,820 students usable classrooms ※ Including the classrooms to be constructed under BPEP-II by July 2004 2) Improvement of Teacher Training Environment By constructing exclusive facilities for Resource Centres, the Project will contribute to activating teacher training and information-sharing, which will lead to improved quality of education. (2) Indirect Effects 1) Enhancement of Community Participation to Education Community participation in overall primary school management activities will be enhanced through participation in this construction project and by receiving guidance on various educational matters from the government. 91 3-2 Recommendations For the effective implementation of the project, it is recommended that HMG of Nepal take the following actions: 1) Coordination with other donors As and when necessary for the effective implementation of the Project, the DOE should ensure effective coordination with the CIP donors in terms of the CIP components including the allocation of target districts. -

Study of Potentiality of Rainwater Harvesting As a Climate Change Adaptation 2016
Study of Potentiality of Rainwater Harvesting As a climate Change Adaptation 2016 Government of Nepal Ministry of Water Supply & Sanitation Department of Water Supply & Sewerage Water supply & Sanitation Division Office, Arghakhanchi Study of Potentiality of Rainwater Harvesting System as a Climate Change Adaptation Option in Arghamaidan, Arghakhanchi district Nov 15, 2016 Submitted by: Water Supply & Sanitation Division office, Arghakhanchi Tel.: 077420110 Email:[email protected], 1 WSSDO,Arghakhanchi Study of Potentiality of Rainwater Harvesting As a climate Change Adaptation 2016 Contents List of Figures .......................................................................................................................................... 4 List of Tables ........................................................................................................................................... 4 ACRONYMS AND ABBREVIATIONS .......................................................................................................... 5 EXECUTIVE SUMMARY ............................................................................................................................ 6 1. GENERAL INFORMATION .................................................................................................................... 8 1.1 Introduction .................................................................................................................................. 8 1.2 Project Background ...................................................................................................................... -

Strengthening the Role of Civil Society and Women in Democracy And
HARIYO BAN PROGRAM Monitoring and Evaluation Plan 25 November 2011 – 25 August 2016 (Cooperative Agreement No: AID-367-A-11-00003) Submitted to: UNITED STATES AGENCY FOR INTERNATIONAL DEVELOPMENT NEPAL MISSION Maharajgunj, Kathmandu, Nepal Submitted by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660, Baluwatar, Kathmandu, Nepal First approved on April 18, 2013 Updated and approved on January 5, 2015 Updated and approved on July 31, 2015 Updated and approved on August 31, 2015 Updated and approved on January 19, 2016 January 19, 2016 Ms. Judy Oglethorpe Chief of Party, Hariyo Ban Program WWF Nepal Baluwatar, Kathmandu Subject: Approval for revised M&E Plan for the Hariyo Ban Program Reference: Cooperative Agreement # 367-A-11-00003 Dear Judy, This letter is in response to the updated Monitoring and Evaluation Plan (M&E Plan) for the Hariyo Program that you submitted to me on January 14, 2016. I would like to thank WWF and all consortium partners (CARE, NTNC, and FECOFUN) for submitting the updated M&E Plan. The revised M&E Plan is consistent with the approved Annual Work Plan and the Program Description of the Cooperative Agreement (CA). This updated M&E has added/revised/updated targets to systematically align additional earthquake recovery funding added into the award through 8th modification of Hariyo Ban award to WWF to address very unexpected and burning issues, primarily in four Hariyo Ban program districts (Gorkha, Dhading, Rasuwa and Nuwakot) and partly in other districts, due to recent earthquake and associated climatic/environmental challenges. This updated M&E Plan, including its added/revised/updated indicators and targets, will have very good programmatic meaning for the program’s overall performance monitoring process in the future. -

Council Notification Letter
GLOBAL ENVIRONMENT FACILITY INVESTING IN OUR PLANET Naoko Ishii CEO and Chairperson March 18, 2015 Dear LDCF /SCCF Council Member: F AO as the Implementing Agency for the project entitled: Nepal: Reducing Vulnerability and Increasing Adaptive Capacity to Respond to Impacts of Climate Change and Variability for Sustainable Livelihoods in Agriculture Sector in Nepal has submitted the attached proposed project document for CEO endorsement prior to final approval of the project document in accordance. with F AO procedures. The Secretariat has reviewed the project document. It is consistent with the proposal approved by LDCF/SCCF Council in May 2013 and the proposed project remains consistent with the Instrument and LDCF/SCCF policies and procedures. The attached explanation prepared by F AO satisfactorily details how Council's comments have been addressed. I am, therefore, endorsing the project document. We have today posted the proposed project document on the GEF website at www.TheGEF.org. If you do not have access to the Web, you may request the local field office of UNDP or the World Bank to download the document for you. Alternatively, you may request a copy of the document from the Secretariat. If you make such a request, please confirm for us your current mailing address. Sincerely, Naoko Ishii Chief Executive Officer and Chairperson Attachment: GEFSEC Project Review Document Copy to: Country Operational Focal Point, GEF Agencies, STAP, Trustee 1818 H Street, NW• Washington, DC 20433 •USA Tel:+ 1 (202) 473 3202 - Fax:+ 1 (202) 522 -

Analysis on Causes of Deforestation and Forest Degradation of Dang District: Using DPSIR Framework
Nep J Environ Sci (2015), 3, 27-34 ISSN 2350-8647 Research Article Analysis on causes of deforestation and forest degradation of Dang district: using DPSIR framework Krishna Dev Hengaju1* and Ugan Manandhar2 1School of Environmental Science and Management, Pokhara University (affiliated), Kathmandu, Nepal 2World Wildlife Fund, Kathmandu, Nepal Abstract Forests play a prodigious significance in many aspects. It is home to sundry species that exist on earth. Further, forest plays vital role as sinks of CO 2 and has been estimated that standing forests sequester about 20% of global CO 2 emission. However, deforestation and forest degradation (D & D) has been continued to be a major global environmental problem. The study was focused on identifying the causes of D & D of Dang district using the Drivers – Pressures – State – Impacts – Responses (DPSIR) framework. A detailed review of relevant and existing literatures about the study area was done and also field observation and survey was carried out during the study in different village development committees (VDCs) of Dang district. Data and information collected were used for preparing the DPSIR model framework making the DPSIR key words table and DPSIR map. The VDCs were identified by comparing the land use land cover map of Dang district of 2000 and 2010. The study reveals that main causes of D & D in Dang District are forest encroachment, population growth, forest fire, urbanization, infrastructure development, illegal harvesting of forest resources, etc. It is causing a serious impact on environment. In order to overcome with the situation, government, with an effort from community people, has started awareness programs and many other activities under forest management programs. -
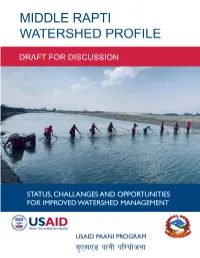
Middle Rapti Watershed Profile: Status, Challenges and Opportunities for Improved Water Resource Management Draft for Discussion
Cover photo: Tharu women fishing together with traditional fishing gear called tapi in the Rapti River, Dang. Photo credit: USAID Paani Program/HWEPC/Pradeep Majgaiya II MIDDLE RAPTI WATERSHED PROFILE: STATUS, CHALLENGES AND OPPORTUNITIES FOR IMPROVED WATER RESOURCE MANAGEMENT DRAFT FOR DISCUSSION Program Title: USAID Paani Program DAI Project Number: 1002810 Sponsoring USAID Office: USAID/Nepal IDIQ Number: AID-OAA-I-14-00014 Task Order Number: AID-367-TO-16-00001 Contractor: DAI Global LLC Date of Publication: January 31, 2019 The authors’ views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. III CONTENTS TABLES ....................................................................................................................... VI ABBREVIATIONS ..................................................................................................... IX ACKNOWLEDGEMENTS .......................................................................................... 1 EXECUTIVE SUMMARY ............................................................................................ 2 1. MIDDLE RAPTI WATERSHED: NATURE, WEALTH AND POWER ....... 9 2.1 MIDDLE RAPTI WATERSHED ......................................................................................... 10 2.2 WATER AVAILABILITY AND QUALITY .......................................................................... 11 2.3 LAND USE AND LAND COVER ........................................................................................... -

CHITWAN-ANNAPURNA LANDSCAPE: a RAPID ASSESSMENT Published in August 2013 by WWF Nepal
Hariyo Ban Program CHITWAN-ANNAPURNA LANDSCAPE: A RAPID ASSESSMENT Published in August 2013 by WWF Nepal Any reproduction of this publication in full or in part must mention the title and credit the above-mentioned publisher as the copyright owner. Citation: WWF Nepal 2013. Chitwan Annapurna Landscape (CHAL): A Rapid Assessment, Nepal, August 2013 Cover photo: © Neyret & Benastar / WWF-Canon Gerald S. Cubitt / WWF-Canon Simon de TREY-WHITE / WWF-UK James W. Thorsell / WWF-Canon Michel Gunther / WWF-Canon WWF Nepal, Hariyo Ban Program / Pallavi Dhakal Disclaimer This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of Kathmandu Forestry College (KAFCOL) and do not necessarily reflect the views of WWF, USAID or the United States Government. © WWF Nepal. All rights reserved. WWF Nepal, PO Box: 7660 Baluwatar, Kathmandu, Nepal T: +977 1 4434820, F: +977 1 4438458 [email protected] www.wwfnepal.org/hariyobanprogram Hariyo Ban Program CHITWAN-ANNAPURNA LANDSCAPE: A RAPID ASSESSMENT Foreword With its diverse topographical, geographical and climatic variation, Nepal is rich in biodiversity and ecosystem services. It boasts a large diversity of flora and fauna at genetic, species and ecosystem levels. Nepal has several critical sites and wetlands including the fragile Churia ecosystem. These critical sites and biodiversity are subjected to various anthropogenic and climatic threats. Several bilateral partners and donors are working in partnership with the Government of Nepal to conserve Nepal’s rich natural heritage. USAID funded Hariyo Ban Program, implemented by a consortium of four partners with WWF Nepal leading alongside CARE Nepal, FECOFUN and NTNC, is working towards reducing the adverse impacts of climate change, threats to biodiversity and improving livelihoods of the people in Nepal. -

District Disaster Risk Management Plan for Arghakhanchi District
Ministry of Agriculture Food and Agriculture and Cooperatives (MOAC) Organization of the United Nations District Disaster Risk Management Plan (DDRMP) Arghakhanchi District April 2011 Priority Framework for Action Climate Change Adaptation and Disaster Risk Management in Agriculture Publisher: Government of Nepal Ministry of Agriculture and Cooperatives Kathmandu, Nepal Copyright: April 2011 Ministry of Agriculture and Cooperatives Government of Nepal Prepared under the FAO Technical Assistance to the Government of Nepal (TCP/NEP/3201 (D) and UNJP/NEP/OO5/UNJ) Table of Contents Acronyms and Abbreviations Preface Executive Summary Page 1. Introduction ................................................................................................................................... 1 1.1. The Rationale for District Disaster Risk Management Plans ................................................ 1 1.2. Objectives of the Arghakhanchi DDRMP ............................................................................. 1 1.3. Methodology .......................................................................................................................... 4 1.3.1. Framework for DDRMP Preparation .............................................................................. 4 1.3.2. Building the picture – Assessing the disaster context in Arghakhanchi ......................... 4 1.3.3. Data collection methods .................................................................................................. 6 1.4. Layout of the Plan ................................................................................................................ -

Enacting Dialogue Searching for Peace Through Storytelling
EnActing Dialogue Searching for Peace Through Storytelling EnActing Dialogue Searching for Peace Through Storytelling EnActing Dialogue Searching for Peace Through Storytelling with means of : Published by and Copyright © Forum for Protection of Public Interest (Pro Public) Link Marg, Kuleshwor PO Box: 14307, Kathmandu, Nepal Phone: +977-01-4283469, 4286361 http://www.propublic.org CSSP-Berlin Center for Integrative Mediation Berlin Office: +49/ 30/ 4000651 - 11 | fax: +49/ 30/ 4000651 -21 Landgrafenstraße 15, 10787 Berlin http://www.cssp-mediation.org Publication Year 2017 Layout, Printing and Publication Coordination Middleway Films, 9841435961 Table of Contents Acknowledgements .................................................................................................................................................................1 Introduction ................................................................................................................................................................................3 Wounds of War ...........................................................................................................................................................................9 He Went Just Like That .......................................................................................................................................................... 13 Let Such Days Never Come Back Again ......................................................................................................................... -

C E N T R a L W E S T E
Bhijer J u m l a Saldang N E P A L - W E S T E R N R E G I O N Patarasi Chhonhup f Zones, Districts and Village Development Committees, April 2015 Tinje Lo M anthang Kaingaon National boundary Zone boundary Village Development Comm ittee boundary Phoksundo Chhosar Region boundary District boundary Gothichour Charang Date Created: 28 Apr 2015 Contact: [email protected] Data sources: WFP, Survey Department of Nepal, SRTM Website: www.wfp.org 0 10 20 40 Rim i Prepared by: HQ, OSEP GIS The designations employed and the presentation of material in M I D - W E Dho S T E R N the map(s) do not imply the expression of any opinion on the Kilom eters part of WFP concerning the legal or constitutional status of any Map Reference: country, territory, city or sea, or concerning the delimitation of its ± frontiers or boundaries. Sarmi NPL_ADMIN_WesternRegion_A0L Pahada © World Food Programme 2015 Narku Chharka Liku Gham i Tripurakot Kalika K A R N A L I FAR-W ESTERN Lhan Raha MID-W ESTERN BJ a Hj a Er kRo It Surkhang Bhagawatitol Juphal D o l p a M u s t a n g W ESTERN Lawan Suhu Chhusang CENTRAL Gotam kot EASTERN Dunai Majhphal Mukot Kagbeni Sahartara Jhong Phu Nar Syalakhadhi Sisne Marpha Muktinath Jom som Tangkim anang Tukuche Ranm am aikot M a n a n g Baphikot Jang Pipal Pwang R u k u m Kowang Khangsar Ghyaru Mudi Pokhara M y a g d i Bhraka Sam agaun Gurja Ransi Hukam Syalpakha Kunjo Thoche W LeteE S T Manang E R N Chokhawang Kanda Narachyang Sankh Shova Chhekam par Kol Bagarchhap Pisang Kuinem angale Marwang Taksera Prok Dana Bihi Lulang Chim khola -
BIODIVERSITY, PEOPLE and CLIMATE CHANGE Final Technical Report of the Hariyo Ban Program, First Phase
BIODIVERSITY, PEOPLE AND CLIMATE CHANGE Final Technical Report of the Hariyo Ban Program, First Phase Volume Two Detailed Annexes HARIYO BAN PROGRAM This final technical report for Hariyo Ban Program Phase One is submitted to the United States Agency for International Development Nepal Mission by World Wildlife Fund Nepal in partnership with CARE, the Federation of Community Forest Users Nepal and the National Trust for Nature Conservation, under Cooperative Agreement Number AID-367-A-11-00003. © WWF Nepal 2017 All rights reserved Citation Please cite this report as: WWF Nepal. 2017. Biodiversity, People and Climate Change: Final Technical Report of the Hariyo Ban Program, First Phase. WWF Nepal, Hariyo Ban Program, Kathmandu, Nepal. Cover photo credit © Karine Aigner/WWF-US Disclaimer: This report is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of WWF and do not necessarily reflect the views of USAID or the United States Government. 7 April, 2017 Table of Contents ANNEX 5: HARIYO BAN PROGRAM WORKING AREAS ......................................................................... 1 ANNEX 6: COMMUNITY BASED ANTI-POACHING UNITS FORMED/REFORMED ................................. 4 ANNEX 7: SUPPORT FOR INTEGRATED SUB-WATERSHED MANAGEMENT PLANS ........................... 11 ANNEX 8: CHARACTERISTICS OF PAYMENTS FOR ECOSYSTEM SERVICES SCHEMES PILOTED ......... 12 ANNEX 9: COMMUNITY ADAPTATION PLANS OF ACTION PREPARED .............................................