Hidradenitis Suppurativa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
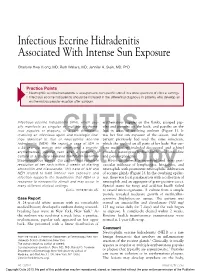
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F. -

Understanding Hidradenitis Suppurativa (Hs)
UNDERSTANDING HIDRADENITIS SUPPURATIVA (HS) Information to help you work with your doctor so you can better manage your HS WHAT’S INSIDE Hidradenitis suppurativa (HS) in brief . 4 HS – the facts . 5 Living with HS . 9 Coping with HS . 11 Tips and tricks for living with HS . 12 Addressing your thoughts and feelings . 14 Coping with stress . 16 Working with your health care team . 17 Symptom self-assessment questionnaire . 19 Useful online resources . 23 3 HIDRADENITIS SUPPURATIVA (HS) IN BRIEF You have been diagnosed with HS, a disease which is: PAINFUL PRORESSIVE INFLAMMATORY GETTING WORSE CAUSING OVER TIME SWELLING CHRONIC SYSTEMIC LASTING AFFECTING A LONG TIME THE WHOLE BODY HS is known to produce lesions in the skin that are inflamed (swollen), recurrent (reappearing after lesions disappear), and chronic (lasting a long period of time). HS can have both a physical and psychological impact. The resulting pain and affected areas of your skin can restrict movement and your ability to do day-to-day tasks. Because of the areas of the body affected and how unsightly, smelly, and uncomfortable or painful HS may be, it can also lead to negative feelings such as embarrassment, stress and low mood. While we understand this is how some people with HS may feel, it’s important to remember that HS is a medical condition — its development is not your fault. 4 It’s important to be able to manage the physical side of the condition while also trying to reduce any feelings of embarrassment you may feel. There is more information about addressing your thoughts and feelings on page 14. -

Hidradenitis Suppurativa Hidradenitis Suppurativa (HS) Is an Inflammatory Skin Disease That Many People Mistake for Acne Or Infectious Boils
Dermatology Patient Education Hidradenitis Suppurativa Hidradenitis suppurativa (HS) is an inflammatory skin disease that many people mistake for acne or infectious boils. Another name for HS is acne inversa, which means acne that appears in the skin folds such as the underarms, groin, buttocks, and underneath the breasts. Unlike acne, many people have HS for life. Early diagnosis can help patients receive effective treatment options that will help control symptoms. WHAT DOES HS LOOK LIKE? HS typically looks like acne on a part of the body where you normally would not have acne, particularly on areas of the body where skin touches skin. You may notice: • Pimple-like bumps • Deep acne-like cysts and blackheads • Bumps with a hair coming out of them (folliculitis) • Boils • Scarring Hidradenitis Suppurativa If HS worsens, you may notice that your bumps grow larger, become painful, and feel hot and tender. If HS bumps break open or rupture, they can leak a blood-stained, foul-smelling pus. Once the bumps heal, deep scars can appear that look like tunnels under the skin. These scars can be painful and thicken. You may experience a limited range of motion in the area where the bumps appeared because of scarring and pain. HS is most common in the armpits and groin. It also forms on and under women’s breasts, on the buttocks, and around the anus. As it worsens, HS can appear on skin that receives a lot of friction such as around your waist, the inner thighs, and the back of your neck. It even develops behind the ears, on the scalp, and on the eyelids. -

Differential Diagnosis of the Scalp Hair Folliculitis
Acta Clin Croat 2011; 50:395-402 Review DIFFERENTIAL DIAGNOSIS OF THE SCALP HAIR FOLLICULITIS Liborija Lugović-Mihić1, Freja Barišić2, Vedrana Bulat1, Marija Buljan1, Mirna Šitum1, Lada Bradić1 and Josip Mihić3 1University Department of Dermatovenereology, 2University Department of Ophthalmology, Sestre milosrdnice University Hospital Center, Zagreb; 3Department of Neurosurgery, Dr Josip Benčević General Hospital, Slavonski Brod, Croatia SUMMARY – Scalp hair folliculitis is a relatively common condition in dermatological practice and a major diagnostic and therapeutic challenge due to the lack of exact guidelines. Generally, inflammatory diseases of the pilosebaceous follicle of the scalp most often manifest as folliculitis. There are numerous infective agents that may cause folliculitis, including bacteria, viruses and fungi, as well as many noninfective causes. Several noninfectious diseases may present as scalp hair folli- culitis, such as folliculitis decalvans capillitii, perifolliculitis capitis abscendens et suffodiens, erosive pustular dermatitis, lichen planopilaris, eosinophilic pustular folliculitis, etc. The classification of folliculitis is both confusing and controversial. There are many different forms of folliculitis and se- veral classifications. According to the considerable variability of histologic findings, there are three groups of folliculitis: infectious folliculitis, noninfectious folliculitis and perifolliculitis. The diagno- sis of folliculitis occasionally requires histologic confirmation and cannot be based -

Hidradenitis Suppurativa: a Common and Burdensome, Yet Under-Recognised, Inflammatory Skin Disease Deirdre Nathalie Dufour,1 Lennart Emtestam,2 Gregor B Jemec1
PGMJ Online First, published on February 24, 2014 as 10.1136/postgradmedj-2013-131994 Postgrad Med J: first published as 10.1136/postgradmedj-2013-131994 on 24 February 2014. Downloaded from Review Hidradenitis suppurativa: a common and burdensome, yet under-recognised, inflammatory skin disease Deirdre Nathalie Dufour,1 Lennart Emtestam,2 Gregor B Jemec1 1Department of Dermatology, ABSTRACT patients with this disease. Topics such as aetiology, Health Sciences Faculty, Hidradenitis suppurativa (HS) is a chronic, relapsing, pathogenesis, therapeutic options and clinical man- Roskilde Hospital, University of fl Copenhagen, Copenhagen, in ammatory skin condition that typically occurs after agement clearly are important, but are beyond the Denmark puberty. The primary clinical presentation is painful scope of this review; however, these topics have – 2Department of Dermatology, inflamed nodules or boils in the apocrine gland-bearing been reviewed in other recent publications.6 11 Karolinska University Hospital regions (armpits, genital area, groin, breasts and and Karolinska Institutet, buttocks/anus) that progress to abscesses, sinus tracts Stockholm, Sweden PREVALENCE, PATIENT CHARACTERISTICS AND and scarring. Severity is typically described according to SEX DIFFERENCES Correspondence to three Hurley categories, with most patients having mild Before a study in a young Danish population under- Professor L Emtestam, or moderate disease. Estimated prevalence is 1–4% going screening for sexually transmitted diseases Department of Dermatology, worldwide and HS is three times more common in (N=507), in which Jemec et al1 found a point Karolinska University Hospital ’ and Karolinska Institutet, women than men. Patients disease burden includes prevalence of 4.1%, the prevalence of HS had not Stockholm SE-141 86, Sweden; intense pain, work disability and overall poor quality been estimated systematically (figure 1). -

Alopecia with Perifollicular Papules and Pustules
Tyler A. Moss, DO; Thomas M. Alopecia with perifollicular Beachkofsky, MD; Samuel F. Almquist, MD; Oliver J. Wisco, DO; papules and pustules Michael R. Murchland, MD A.T. Still University, Our 23-year-old patient thought his hair loss was Kirksville College of Osteopathic Medicine, probably “genetic.” But that didn’t explain the painful Kirksville, Mo (Dr. Moss); Kunsan AB, Republic of pustules. Korea (Dr. Beachkofsky); Wilford Hall Medical Center, Lackland AFB, Tex (Drs. Almquist, Wisco, and Murchland) A 23-year-old African American man Physical examination revealed multiple sought care at our medical center because perifollicular papules and pustules on the [email protected] he had been losing hair over the vertex of his vertex of his scalp with interspersed patches DEPARTMENT EDITOR scalp for the past several years. He indicated of alopecia (FIGURE 1). Th ere were no lesions Richard P. Usatine, MD that his father had early-onset male patterned elsewhere on his body and his past medical University of Texas Health alopecia. As a result, he considered his hair history was otherwise unremarkable. Science Center at San Antonio loss “genetic.” However, he described waxing and waning fl ares of painful pustules associ- ● The authors reported no WHAT IS YOUR DIAGNOSIS? potential confl ict of interest ated with occasional spontaneous bleeding relevant to this article. and discharge of purulent material that oc- ● HOW WOULD YOU MANAGE curred in the same area as the hair loss. THIS PATIENT? FIGURE 1 Alopecia with a painful twist A B PHOTOS COURTESY OF: OLIVER J. WISCO, DO PHOTOS COURTESY This 23-year-old patient said that he had spontaneous bleeding and discharge of purulent material in the area of his hair loss. -

Minor Procedures
MINOR PROCEDURES ELIZABETH BLUNT, RN, PHD, FNP-BC COLLEEN STELLABOTTE, RN, MSN, FNP-BC Today’s Agenda Digital block Subungual hematoma Ingrown toenail management Nail removal Abscess I & D Indication for Digital Blocks •Patients with crush injuries •Need x-rays •Need extensive wound exploration •Tendon injuries requiring evaluation •Multiple lacerations in same digit •Multiple foreign bodies in same digit •Partial or total nail removal Local Anesthetics •Mechanism of action • Infiltrate tissue and diffuse across neural sheaths and membranes • Interfere with neuronal depolarization • Prevent Na influx • No action potential, no nerve impulse •Onset of Action • Technique of injection, concentration, total dose • Knowledge of anatomy is important • Injection between dermis and subcutaneous tissue = immediate anesthesia •Duration of action • Increased with epinephrine • Do not use epinephrine in fingers, toes, nose, penis, ears • Increased with long acting anesthetics such as Bupivicaine and Marcaine Wound Anesthesia GOAL = Reduce Pain and Anxiety • Type of anesthetic used • Needle size 27 or 30-gauge • Inexperienced – start with 25-gauge • 25-gauge or 27-gauge ½-inch needle • pH - buffering • Temperature of solution • Speed and depth of injection Three Major Techniques for Digital Block • Dorsal surface • Indicated when only the nail is involved • Aberrant anatomy may make the technique less than optimal • Web space • Need larger volume of anesthetic • Less control of instillation • Medial/lateral • Focused area of instillation • Volume parameters -

Buffalo Medical Group, P.C. Robert E
Buffalo Medical Group, P.C. Robert E. Kalb, M.D. Phone: (716) 630-1102 Fax: (716) 633-6507 Department of Dermatology 325 Essjay Road Williamsville, New York 14221 2 FOOT- 1 HAND SYNDROME 2 foot - 1 hand syndrome is a superficial infection of the skin caused by the common athlete's foot fungus. It is quite common for people to have a minor amount of an athlete's foot condition. This would appear as slight scaling and/or itching between the toes. In addition, patients may have thickened toenails as part of the athlete's foot condition. Again the problem on the feet is very common and often patients are not even aware of it. In some patients, however, the athlete's foot fungus can spread to another area of the body. For some strange and unknown reason, it seems to affect only one hand. That is why the condition is called 2 foot - 1 hand syndrome. It is not clear why the problem develops in only one hand or why the right or left is involved in some patients. Fortunately there is very effective treatment to control this minor skin problem. If the problem with the superficial fungus infection is confined to the skin, then a short course of treatment with an oral antibiotic is all that is required. This antibiotic is very safe and normally clears the skin up fairly rapidly. It is often used with a topical cream to speed the healing process. If, however, the fingernails of the affected hand are also involved then a more prolonged course of the antibiotic will be necessary. -

Treatment Consideration for US Military Members with Skin Disease
MILITARY DERMATOLOGY IN PARTNERSHIP WITH THE ASSOCIATION OF MILITARY DERMATOLOGISTS Treatment Consideration for US Military Members With Skin Disease Kristina R. Burke, MD; David C. Larrymore, MD; Sunghun Cho, MD Medical readiness is maintaining a unit that is medi- PRACTICE POINTS cally able to perform its military function both at home • Certain conditions and treatments are incompatible and in a deployed environment. Military members’ medical with military service and may result in separation. readiness status is carefully tracked and determined via • Dermatologists must consider a patient’s profession annual physical, dental, hearing, and vision examina- when choosing a treatment modality. tions, as well as human immunodeficiency virus status and immunizations. The readiness status of the unit (ie, the number of troops ready to deploy at any given time) Recent changes to military medicine precipitated by the National is available to commanders at all levels at any time. Each Defense Authorization Act for Fiscal Year 2017 are expected to result military branch hascopy tracking systems that allow command- in civilian specialists playing a larger role in the care of our military ers to know when a member is past due for an examina- population. Medical readiness and deployment eligibility should be tion or if a member’s medical status has changed, making taken into consideration when establishing a treatment plan for service them nondeployable. When a member is nondeployable, members. This article highlights unique factors civilian dermatologists it affects the unit’s ability to perform its mission and must consider when treating active-duty military patients with acne, degradesnot its readiness.