Differential Diagnosis of the Scalp Hair Folliculitis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
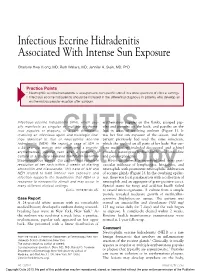
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Abscess Prevention
ABSCESS PREVENTION ▪ Chest pains may occur if infection How do you soak/use Avoiding abscesses goes to heart or lungs compresses? • Wash your hands and the injection site. What should I do if I get ▪ Use warm/hot water (that doesn’t burn your skin) • Use alcohol pads and wipe an abscess? ▪ Soak in tub of plain hot water or hot back & forth (rub hard) over ▪ Treat at home with warm soaks water with Epsom salts injection site to remove dirt. only if: ▪ Use hot, wet, clean washcloth and - No red streaks hold on abscess, if abscess cannot • Then use another new alcohol - Skin not hot and puffy be soaked in tub pad for the final cleaning. ▪ Soak abscess 3 to 4 times a day for ▪ Go to a clinic if abscess: 10-15 minutes each time, if possible What is a skin abscess? - Not improving, especially ▪ Cover with a clean dry bandage after after 5-7 days soaking ▪ Pocket of pus - Gets bigger and/or very ▪ soaking/using compresses ▪ Often found at injection sites, but STOP painful when abscess starts draining can be found elsewhere - Is hot and puffy ▪ More likely with Red streaks start spreading skin-popping from the abscess-go ASAP! muscling What about missing a vein ▪ Go to emergency room if: ▪ May occur even after you stop Chest pain antibiotics? injecting High fever, chills ▪ Take all antibiotics, if Infection looks like it is How do you know it’s an spreading fast prescribed, even if you feel better abscess? ▪ Take antibiotics after you fix (if ▪ using heroin) ▪ Pink or reddish lump on skin ▪ Do not take antibiotics with ▪ Tender or painful Warning -

Multiple Asymptomatic Papules on the Back of the Right Side of the Chest Angoori Gnaneshwar Rao
QUIZ Multiple Asymptomatic Papules on the Back of the Right Side of the Chest Angoori Gnaneshwar Rao A 43-year-old male presented with multiple asymptomatic complete blood picture, blood sugar, complete urine examination, papules on the back of the right side of the chest of 1 year blood urea, serum creatinine, liver function tests and serum duration. He was asymptomatic a year back then he developed lipid profile were normal. Fundus was normal. A slit skin smear small papules on the right side of the front of the chest initially for acid fast bacilli was negative. A punch biopsy from the and later on involved the front and back of the chest. No representative lesion subjected to histopathological examination history was suggestive of leprosy and hyperlipidemias. Family revealed a cyst with an intricately folded wall, lined by two to history was negative for similar problem. Examination revealed three layers of flattened squamous epithelium and the absence multiple skin-colored to yellowish papules distributed on the of the granular layer. Lobules of sebaceous glands were found front and back of the chest and shoulder region on the right embedded in cyst lining. The lumen was filled with amorphous side [Figure 1]. Also, there were multiple hyperpigmented eosinophilic material and multiple hair shafts [Figures 2-4]. macules on the right infrascapular region. There was no nerve thickening and no sensory deficit and there were no Question hypopigmented or anesthetic patches. Systemic examination did not reveal any abnormality. Routine investigations including What is your diagnosis? (Original) Multiple skin-colored to yellowish papules on the back of chest Figure 1: Figure 2: (Original) Histopathology of skin showing a cyst with an intricately folded and shoulder region on the right side wall lined by two to three layers of flattened squamous epithelium and the absence of granular layer. -

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

Rapid Development of Perifolliculitis Following Mesotherapy
CASE LETTER Rapid Development of Perifolliculitis Following Mesotherapy Weihuang Vivian Ning, MD; Sameer Bashey, MD; Gene H. Kim, MD patient received mesotherapy with an unknown substance PRACTICE POINTS for cosmetic rejuvenation; the rash was localized only to the injection sites.copy She did not note any fever, chills, • Mesotherapy—the delivery of vitamins, chemicals, and plant extracts directly into the dermis via nausea, vomiting, diarrhea, headache, arthralgia, or upper injections—is a common procedure performed respiratory tract symptoms. She further denied starting in both medical and nonmedical settings for any new medications, herbal products, or topical therapies cosmetic rejuvenation. apart from the procedure she had received 2 weeks prior. • Complications can occur from mesotherapy treatment. Thenot patient was found to be in no acute distress and • Patients should be advised to seek medical care with vital signs were stable. Laboratory testing was remarkable US Food and Drug Administration–approved cosmetic for elevations in alanine aminotransferase (62 U/L [refer- techniques and substances only. ence range, 10–40 U/L]) and aspartate aminotransferase (72 U/L [reference range 10–30 U/L]). Moreover, she had Doan absolute neutrophil count of 0.5×103 cells/µL (refer- ence range 1.8–8.0×103 cells/µL). An electrolyte panel, To the Editor: creatinine level, and urinalysis were normal. Physical Mesotherapy, also known as intradermotherapy, is a examination revealed numerous 4- to 5-mm erythematous cosmetic procedure in which multiple -

Borrelia Burgdorferi and Treponema Pallidum: a Comparison of Functional Genomics, Environmental Adaptations, and Pathogenic Mechanisms
PERSPECTIVE SERIES Bacterial polymorphisms Martin J. Blaser and James M. Musser, Series Editors Borrelia burgdorferi and Treponema pallidum: a comparison of functional genomics, environmental adaptations, and pathogenic mechanisms Stephen F. Porcella and Tom G. Schwan Laboratory of Human Bacterial Pathogenesis, Rocky Mountain Laboratories, National Institute of Allergy and Infectious Diseases, NIH, Hamilton, Montana, USA Address correspondence to: Tom G. Schwan, Rocky Mountain Laboratories, 903 South 4th Street, Hamilton, Montana 59840, USA. Phone: (406) 363-9250; Fax: (406) 363-9445; E-mail: [email protected]. Spirochetes are a diverse group of bacteria found in (6–8). Here, we compare the biology and genomes of soil, deep in marine sediments, commensal in the gut these two spirochetal pathogens with reference to their of termites and other arthropods, or obligate parasites different host associations and modes of transmission. of vertebrates. Two pathogenic spirochetes that are the focus of this perspective are Borrelia burgdorferi sensu Genomic structure lato, a causative agent of Lyme disease, and Treponema A striking difference between B. burgdorferi and T. pal- pallidum subspecies pallidum, the agent of venereal lidum is their total genomic structure. Although both syphilis. Although these organisms are bound togeth- pathogens have small genomes, compared with many er by ancient ancestry and similar morphology (Figure well known bacteria such as Escherichia coli and Mycobac- 1), as well as by the protean nature of the infections terium tuberculosis, the genomic structure of B. burgdorferi they cause, many differences exist in their life cycles, environmental adaptations, and impact on human health and behavior. The specific mechanisms con- tributing to multisystem disease and persistent, long- term infections caused by both organisms in spite of significant immune responses are not yet understood. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA). -

Primary Follicular Mucinosis
International Journal of Scientific & Engineering Research Volume 8, Issue 6, June-2017 1303 ISSN 2229-5518 Case Report Primary Follicular Mucinosis: A Case Report From Saudi Arabia With Successful Treatment And Literature Review SalaimanAlsaiari1 AwadhAlAmri2 AmerAlmuqati Ibrahim Allihibi ABSTRACT: Background:Follicular mucinosis is an uncommon inflammatory disorder that characteristically presents as clearly defined, erythematous plaques or papules, with follicular projections, superficial scaling, and alopecia in terminal hair bearing areas, characterized histologically by mucin accumulation in pilosebaceous units (follicular epithelium and sebaceous glands) . The condition is generally divided into primary (idiopathic) and secondary forms in association with several conditions including benign and malignant diseases. There are many local and systemic treatments. Main observations: We report a case of 15 years old male with primary follicular mucinosis treated effectively by intralesional steroid injections. Conclusions: This is a new case of Primary follicular mucinosis from Saudi Arabia was treated successfully with intralesional corticosteroids without relapse. KEYWORDS:follicular mucinosis, intralesional corticosteroids, treatment. —————————— —————————— INTRODUCTIONIJSER Follicular mucinosis is a rare condition, of unknown cause, which affects all races, ages and both sexes.1,2It is defined as the accumulation of mucin in the follicular epithelium and sebaceous glands.3,5 It was initially described in 1957 by Pinkus who named it -

C.O.E. Continuing Education Curriculum Coordinator
CONTINUING EDUCATION All Rights Reserved. Materials may not be copied, edited, reproduced, distributed, imitated in any way without written permission from C.O. E. Continuing Education. The course provided was prepared by C.O.E. Continuing Education Curriculum Coordinator. It is not meant to provide medical, legal or C.O.E. professional services advice. If necessary, it is recommended that you consult a medical, legal or professional services expert licensed in your state. Page 1 of 199 Click Here To Take Test Now (Complete the Reading Material first then click on the Take Test Now Button to start the test. Test is at the bottom of this page) 5 hr. Nail Structure and Growth & TCSG Health and Safety Outline Why Study Nail Structure and Growth? • The Natural Nail • Nail Anatomy • Nail Growth • Know Your Nails Objectives After completing this section, you should be able to: C.O.E.• Describe CONTINUING the structure and composition of nails. EDUCATION • Discuss how nails grow. • Identify diseases and disorders of the nail All Rights Reserved. Materials may not be copied, edited, reproduced, distributed, imitated in any way without written permission from C.O. E. Continuing Education. The course provided was prepared by C.O.E. Continuing Education Curriculum Coordinator. It is not meant to provide medical, legal or professional services advice. If necessary, it is recommended that you consult a medical, legal or professional services expert licensed in your state. 1 CONTINUING EDUCATION All Rights Reserved. Materials may not be copied, edited, reproduced, distributed, imitated in any way without written permission from C.O. -

Eradication of Staphylococcus Aureus and MRSA in the Nares: a Historical Perspective of the Ecological Niche, with Suggestions for Future Therapy Considerations
Advances in Microbiology, 2017, 7, 420-449 http://www.scirp.org/journal/aim ISSN Online: 2165-3410 ISSN Print: 2165-3402 Eradication of Staphylococcus aureus and MRSA in the Nares: A Historical Perspective of the Ecological Niche, with Suggestions for Future Therapy Considerations Eric Bornstein Nomir Medical Technologies, Woodmere, NY, USA How to cite this paper: Bornstein, E. (2017) Abstract Eradication of Staphylococcus aureus and MRSA in the Nares: A Historical Perspec- Nasal colonization with pathogenic bacteria continues to present challenges for tive of the Ecological Niche, with Sugges- patients undergoing surgical procedures, and for the physicians that treat them. tions for Future Therapy Considerations. Advances in Microbiology, 7, 420-449. Even as molecular medicine produces ever faster and improved data sets for cli- https://doi.org/10.4236/aim.2017.76034 nicians, it would benefit all medical personnel attempting to decolonize the nose to better understand the historical nasal decolonization data with specific refer- Received: April 28, 2017 ence to the ecological niche for these bacteria, as it has been recorded for more Accepted: June 12, 2017 Published: June 15, 2017 than a century. Much of the historical data points to the largest ecological niche for nasal Staphylococcus aureus as the vibrissae of the vestibulum nasi. A careful Copyright © 2017 by author and study shows that any topical antimicrobial preparation needs to successfully Scientific Research Publishing Inc. This work is licensed under the Creative penetrate the deepest recesses of these specialized nasal hair follicles, if decolo- Commons Attribution International nization is to be adequately accomplished. This review highlights the most rele- License (CC BY 4.0). -

Dermatology Volume 58 Issue 2 March-April 2013 Indian Journal Of
Indian Journal of ISSN: 0019-5154 Dermatology Volume 58 Issue 2 March-April 2013 Indian Journal of Highlights of the issue Dermatology • Update on cutaneous calciphylaxis • Macrophage migration inhibitory factor in • V Dermatology olume • Fixed duration therapy in leprosy 58 • Issue • Environmental dermatoses in Ladakh • Demodex folliculorum as a risk factor in 2 • Diagnosing rosacea March-April • Annular lesions in Dermatology 2013 • Pages Clinical and photomicrograph of Mycosis fungoides, PET-CT for staging and response assessment IJD® Symposium: Integrative Dermatology 87-**** Guest Editor: S R Narahari IJD® www.e-ijd.org E‑Case Report Angiolymphoid Hyperplasia with Eosinophilia with Follicular Mucinosis Rameshwar Gutte, Bhavana Doshi, Uday Khopkar From the Department of Dermatology, Seth G. S. Medical College and King Edward Memorial Hospital, Mumbai, India Abstract Follicular mucinosis occurring along with angiolymphoid hyperplasia with eosinophils (ALHE) has been described in a 49-year-old male. The patient presented with pruritic hyperpigmented papules and nodules on the vertex and right parietal scalp. There was no any other complaint. Histopathological examination from one of the papule showed prominent blood vessels in the dermis lined by plump histiocytoid endothelial cells that were surrounded by a dense lymphoid infiltrate with numerous eosinophils; these findings are typical of angiolymphoid hyperplasia with eosinophilia. Features of follicular mucinosis were observed in the same section with 3 hyperplastic follicular infundibula containing pools of mucin in the infundibular epithelium. The concurrent occurrence of these 2 distinct histopathological patterns in the same biopsy specimen has been reported rarely. Key Words: Angiolymphoid hyperplasia, eosinophilia, follicular mucinosis, scalp What was known? perivascular area and other parts of the dermis.