Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
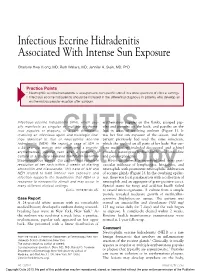
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Familial Hyperinsulinism Due to HNF4A Deficiency and Benign Premature Adrenarche: a Case Report
Case Report Familial Hyperinsulinism due to HNF4A Deficiency and Benign Premature Adrenarche: A Case Report Edward Compton,1 David H. Geller,2 Alaina P. Vidmar MD.3 Abstract Background: Familial Hyperinsulinism due to HNF4A deficiency (FHI-HNF4A) is a form of diazoxide-sensitive, diffuse hyperinsulinism, characterized by transient or persistent hyperinsulinemic hypoglycemia, and a propensity to develop Maturity-Onset Diabetes of the Young type 1 (MODY1). The association between FHI-HNF4A deficiency and benign premature adrenarche (BPA) is unknown. The Case: We report the case of a 5-year-old girl with FHI-HNF4A, controlled on diazoxide, who presented with BPA and Tanner stage 3 pubic hair associated with body odor and acne. Work-up revealed elevated dehydroepiandrosterone sulfate (DHEAS), elevated free testosterone, and advanced bone age. Insulin levels were elevated in the setting of normal fasting blood glucose. We discuss the possible hormonal underpinnings of hyperandrogenism. Conclusion: Though the underlying pathophysiology of this phenotype is unclear, a possible synergistic mechanism exists between insulin-induced hyperandrogenism and HNF4A deficiency leading to a transient decrease of SHBG and thus increased free testosterone levels. Further investigation is required to determine the association between HNF4A dysfunction and BPA. Key Words: Hyperinsulinism; Congenital Hyperinsulinism; Adrenarche; HNF4A; Hyperandrogenism (Source: MeSH-NLM). Introduction Congenital hyperinsulinism (CHI) is due to a variety of etiologies that Highlights: result in dysregulated insulin release from pancreatic β-cells. There are Familial Hyperinsulinism due to HNF4A deficiency (FHI-HNF4A) is a two histological variants of CHI, focal and diffuse, which differ in the form of diazoxide-sensitive; diffuse hyperinsulinism, characterized by extent of pancreatic involvement. -

Notalgia Paresthetica: Cervical Spine Disease and Neuropathic Pruritus
Open Access Case Report DOI: 10.7759/cureus.12975 Notalgia Paresthetica: Cervical Spine Disease and Neuropathic Pruritus Ayesha Akram 1 1. Internal Medicine, Rawalpindi Medical University, Rawalpindi, PAK Corresponding author: Ayesha Akram, [email protected] Abstract Notalgia paresthetica (NP) is a dermatologic condition with predominant, primarily left unilateral pruritus and hyperpigmentation that typically occurs on the upper and middle back. The etiology remains largely elusive. A 57-year-old female with a history of neck pain presented with refractory NP since six months. Through diagnostic x-ray, cervical degenerative changes were discovered at the C5-C6 level, and she was prescribed a course of cervical traction. The cervical theory of NP is presented and is supported with x-ray findings in this case. Categories: Dermatology, Neurology Keywords: notalgia paresthetica, cervical spondylosis, enigmatic link Introduction Notalgia paresthetica (NP) is a cutaneous sensory neuropathy that predominantly affects females, with onset at middle age or older [1,2]. Although it is common, patients underestimate their symptoms, and physicians present an inertia to consider the possibility of NP, and far fewer know about the neuropathic itch. Doubtless, many cases go largely unrecognized, underdiagnosed, or overlooked in the routine clinical practice [3,4]. Pruritus is the overwhelming clinical symptom in the majority of patients [1,5]. A left-sided and posterior location matches well with the location of NP; almost always, NP is unilateral [1]. Hyperpigmentation in the affected area often results from scratching itchy, desensate skin [1]. Along with the pruritus, patients may also experience burning, tingling, coldness, hyperesthesia, hypoesthesia, numbness, or nerve pain in the area where pruritus appeared [6]. -
A Case Report of Refractory Notalgia Paresthetica Treated with Lidocaine
ISSN 1941-5923 © Am J Case Rep, 2017; 18: 1225-1228 DOI: 10.12659/AJCR.905676 Received: 2017.06.07 Accepted: 2017.06.28 A Case Report of Refractory Notalgia Published: 2017.11.20 Paresthetica Treated with Lidocaine Infusions Authors’ Contribution: BEF 1 Yaroslava Chtompel 1 Department of Anesthesiology and Chronic Pain Management, University Study Design A ABE 2 Marzieh Eghtesadi Hospital of Montreal (CHUM), Montreal, QC, Canada Data Collection B 2 Department of Chronic Pain and Headache Medicine, University Hospital of Statistical Analysis C ADE 1 Grisell Vargas-Schaffer Montreal (CHUM), Montreal, QC, Canada Data Interpretation D Manuscript Preparation E Literature Search F Funds Collection G Corresponding Author: Yaroslava Chtompel, e-mail: [email protected] Conflict of interest: None declared Patient: Female, 50 Final Diagnosis: Notalgia parethetica Symptoms: Hyperalgesia • Pruritus Medication: — Clinical Procedure: Intravenous lidocaine infusion Specialty: Anesthesiology Objective: Unusual or unexpected effect of treatment Background: Notalgia paresthetica is a neuropathic condition that manifests as a chronic itch in the thoraco-dorsal region. It is often resistant to treatment, and specific guidelines for its management are lacking. As such, we present a treatment approach with intravenous lidocaine infusions. Case Report: The case involves a 50-year-old woman with spinal cord injury caused by an epidural abscess. The patient de- veloped notalgia paresthetica and sublesional neuropathic pain following its drainage. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Treatment of Hyperhidrosis Dr
“ Finding a solution to my sweating problem has With advanced technology and skilled hands, wholly changed my life. After having the Botox Matthew R. Kelleher, MD provides a full Premier Dermatology spectrum of services and procedures, including: for hyperhidrosis treatment, I am a thousand • Liposculpture times more confi dent and no longer afraid to • Botox, Juvéderm®, and Voluma™ Treatment TREATMENT OF lift my arms and be completely myself. I am so of Wrinkles thankful that this treatment exists!” • Laser Removal of Age Spots and Freckles HYPERHIDROSIS • Laser Facial Rejuvenation - Olivia • Laser Hair Removal Botox for hyperhidrosis patient • Laser Treatments of Rosacea, Facial Redness, and Spider Veins • Laser Scar Reduction • Laser Treatment of Stretch Marks “ Suffering from axillary hyperhidrosis, I thought • Laser Tattoo Removal • Laser Removal of Vascular Birthmarks there was nothing I could do. My condition • Laser and Photodynamic Treatment of Acne made me reluctant to participate in any social • Sclerotherapy for Leg Veins environment. Every day was a struggle until • Thermage® Radiofrequency Tissue Tightening liposuction for hyperhidrosis changed my life! • Microdermabrasion • Botox and Liposculpture Treatment of Hyperhidrosis Dr. Kelleher gave me the confi dence to feel • Sculpsure and Kybella for nonsurgical body sculpting comfortable in my own skin, and I never have to worry about embarrassing sweat stains again!” - Matthew Liposculpture for hyperhidrosis of the underarms patient “ After dealing with my excessive sweating for many years, without fully understanding it was a medical condition, Dr. Kelleher took the time to explain the treatment options available along with their results. I experienced immediate, positive results after my fi rst treatment which gave me a new sense of confi dence and removed the insurmountable stress I carried daily. -

Puberty Journal for Facilitators
JOURNAL Puberty is the bridge between childhood and adulthood. Puberty can start as early as __8 or 9__ years old or as late as__18 or 19__ years old. The average age for girls is ___10.5__ years old. The average age for boys is ___11.5___ years old. Puberty lasts for about _3 to 5__ years. The __pituitary gland__ in the brain signals the production of new hormones or chemicals in the body. Females tend Males tend to have more to have more estrogen and testosterone progesterone hormone. hormones. 2 Set up your board/wall/floor/etc. so that you have three columns for the vocabulary words provided from DMNS: BOYS BOTH GIRLS The DMNS educator will instruct your students to take the vocabulary cards and arrange them into the appropriate column. You should have these cards cut prior to the program. If the students get wrong answers, that is okay and part of the learning process. Once your students see the correct list from the DMNS educator’s presentation, have your students correct their list. It should look as follows after the corrections: BOYS BOTH GIRLS Sperm Production Growth Egg Maturation Erection Voice Changes Menstruation Ejaculation Body Shape Changes Breast Development Nocturnal Emission Interest Changes Emotional Changes Acne Body Hair Body Odor Please keep the list up during the program as the DMNS instructor will be referencing it during the class. Graph the Growth. Analyzing the Data: What do you notice about the girls growth pattern? ___________________________________________________ ___________________________________________________ What do you notice about the boys growth pattern? __________________________________________________ __________________________________________________ 3 NOTES: 4 Draw the actual size of a human egg in the box below: NOTES: 5 Everyone has emotions. -

Got Body Odor? Don’T Sweat It
Healthy Yo u The Nation’s Health May 2021 Got body odor? Don’t sweat it. Follow these tips By Aaron Warnick more frequent or more potent body odor. For example, it will come as no surprise eople don’t naturally smell like to parents that teenagers generally produce lavender or pine or whatever your stronger body odors. Their sweat usually deodorant scent is. It’s normal to stink P will be chemically more potent than an adult’s a little after a workout or long day. But for because they are being flooded with new some, body odor is an everyday problem. In hormones through the puberty process. some cases, your body might be trying to tell Growing older can also change the way we you something is wrong. smell, as our skin changes as we age. A lot of body odor is caused by natural Men, in general, are more likely to produce human functions. >> For more information on body odor stronger body odors and hyperhidrosis, visit www.aad.org Your body releases from sweat. They don’t sweat to cool you down, necessarily sweat more, which is why you’re but they may stink more through your nose that it’s time to check sweatier on hot summer when they do. in on your mental health. days or when you Your diet can also A change in body odor can also occur exercise. But it’s not worsen your body odor. with diabetes. Due to changes in how the sweat that makes you “Foods like onions and body interacts with chemicals, people with work up a stink. -

Skin Conditions and Related Need for Medical Care Among Persons 1=74 Years United States, 1971-1974
Data from the Series 11 NATIONAL HEALTH SURVEY Number 212 Skin Conditions and Related Need for Medical Care Among Persons 1=74 Years United States, 1971-1974 DHEW Publication No. (PHS) 79-1660 U.S, DEPARTMENT OF HEALTH, EDUCATION, AND WELFARE Public Health Service Office of the Assistant Secretary for Health National Center for Health Statistics Hyattsville, Md. November 1978 NATIONAL CENTIER FOR HEALTH STATISTICS DOROTHY P. RICE, Director ROBERT A. ISRAEL, Deputy Director JACOB J. FELDAMN, Ph.D., Associate Director for Amdy.sis GAIL F. FISHER, Ph.D., Associate Director for the Cooperative Health Statistics System ELIJAH L. WHITE, Associate Director for Data Systems JAMES T. BAIRD, JR., Ph.D., Associate Director for International Statistics ROBERT C. HUBER, Associate Director for Managewzent MONROE G. SIRKEN, Ph.D., Associate Director for Mathematical Statistics PETER L. HURLEY, Associate Director for Operations JAMES M. ROBEY, Ph.D., Associate Director for Program Development PAUL E. LEAVERTON, Ph.D., Associate Director for Research ALICE HAYWOOD,, Information Officer DIVISION OF HEALTH EXAMINATION STATISTICS MICHAEL A. W. HATTWICK, M.D., Director JEAN ROEERTS, Chiej, Medical Statistics Branch ROBERT S. MURPHY, Chiej Survey Planning and Development Branch DIVISION OF OPERATIONS HENRY MILLER, ChieJ Health -Examination Field Operations Branch COOPERATION OF THE U.S. BUREAU OF THE CENSUS Under the legislation establishing the National Health Survey, the Public Health Service is authorized to use, insofar as possible, the sesw?icesor facilities of other Federal, State, or private agencies. In accordance with specifications established by the National Center for Health Statis- tics, the U.S. Bureau of the Census participated in the design and selection of the sample and carried out the household interview stage of :the data collection and certain parts of the statis- tical processing. -

Combatting Body Odor by the Means of Microbial Transplantations
Faculty of Bio-science engineering Academic year 2013 – 2014 Combatting body odor by the means of microbial transplantations Murielle Meunier Promotor: Prof. dr. ir. Tom Van De Wiele Promotor: Prof. dr. ir. Nico Boon Tutor: dr. ir. Chris Callewaert A master thesis submitted in partial fulfillment of the requirements for the degree of Master in Bio-science engineering Copyright / Confidentiality “This document may contain confidential information proprietary to the University of Ghent. It is therefore strictly forbidden to publish, cite or make public in any way this document or any part thereof without the express written permission by the University of Ghent. Under no circumstance this document may be communicated to or put at the disposal of third parties; photocopying or duplicating it in any other way is strictly prohibited. Disregarding the confidential nature of this document may cause irremediable damage to the University of Ghent. The author and the promotors do not give the permission to use this thesis for consultation and to copy parts of it for personal use. Every use is subject to the copyright laws, more specifically the source must be extensively specified when using results from this thesis” Ghent, June 2014 The promotors The author Prof. dr. ir. Tom Van de Wiele Murielle Meunier Prof. dr. ir. Nico Boon Acknowledgements This work has been brought to life due to the support and contribution of many people who I would like to thank in particular. First, special thanks to my tutor ir. Chris Callewaert, for his infinite support and comprehension. My promotors prof. dr. ir. Nico Boon and prof. -

Notalgia Paresthetica: Successful Treatment with Exercises
356 Letters to the Editor Notalgia Paresthetica: Successful Treatment with Exercises Anne B. Fleischer1, Tammy J. Meade1 and Alan B. Fleischer2* Departments of 1Physical and Occupational Therapy and 2Dermatology, Wake Forest University Health Sciences, 131 Miller Street, Winston-Salem, NC 27103, USA. *E-mail: [email protected] Accepted September 29, 2010. Notalgia paresthetica (NP) presents typically as a uni- Considering this anatomy, ABF noted that she sat lateral localized itch in the midscapular area. Although with rounded shoulders, which protracted and elevated the pathogenesis of NP has not been fully elucidated, it her scapulae and flexed her head and spine. Within this is widely believed to be a neurogenic itch resulting from position, the cutaneous spinal nerves are under constant spinal nerve impingement or chronic nerve trauma (1, stretch, which causes the spinal nerve angles to become 2). Massey & Fleet (3) postulate that spinal nerves from more severe. T2 to T6 emerge through the multifidus spinae muscle at Knowing that the nerves first pierce the rhomboid right angles and are therefore exposed to chronic trauma. and trapezius muscles prior to becoming cutaneous Further evidence supporting this neurologic causation nerves, ABF thought that she may be able to lessen resides in the reported effective treatment options, which this nerve angle if she strengthened her rhomboids include typical neuralgia therapies, such as topical capsai- and latissimus dorsi muscles as well as stretched the cin (4), gabapentin (5), oxcarbazepine (6), and botulinum pectoral muscles (Fig. 1). By completing these exer- toxin type A (7). In addition, Savk et al. (8) demonstrated cises and stretches, her posture changed from having the use of transcutaneous electrical nerve stimulation to reduce the symptoms of 15 adults with NP. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F.