Understanding Hidradenitis Suppurativa (Hs)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
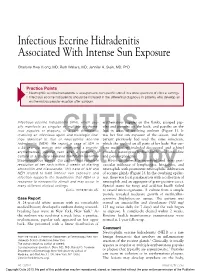
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Endocrinology 12 Michel Faure, Evelyne Drapier-Faure
Chapter 12 Endocrinology 12 Michel Faure, Evelyne Drapier-Faure Key points 12.1 Introduction Q HS does not generally appear to be In 1986 Mortimer et al. [14] reported that hi- associated with signs of hyperan- dradenitis suppurativa (HS) responded to treat- drogenism ment with the potent antiandrogen cyproterone acetate. They suggested that the disease could Q Sex hormones may affect the course of be androgen-dependent [8]. This hypothesis HS indirectly through, for example, was also upheld by occasional reports of women their effects on inflammation with HS under antiandrogen therapy [18]. Actu- ally, the androgen dependence of HS (similarly Q The role of end-organ sensitivity to acne) is only poorly substantiated. cannot be excluded at the time of writing 12.2 Hyperandrogenism and the Skin Q The prevalence of polycystic ovary syndrome in HS has not been system- Androgen-dependent disorders encompass a atically investigated broad spectrum of overlapping entities that may be related in women to the clinical consequenc- es of the effects of androgens on target tissues and of associated endocrine and metabolic dys- functions, when present. #ONTENTS 12.1 Introduction ...........................95 12.2.1 Androgenization 12.2 Hyperandrogenism and the Skin .........95 12.2.1 Androgenization .......................95 One of the less sex-specific effects of androgens 12.2.2 Androgen Metabolism ..................96 12.2.3 Causes of Hyperandrogenism ...........96 is that on the skin and its appendages, and in particular their action on the pilosebaceous 12.3 Lack of Association between HS unit. Hirsutism is the major symptom of hyper- and Endocrinopathies ..................97 androgenism in women. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Metformin for the Treatment of Hidradenitis Suppurativa: a Little Help Along the Way
DOI: 10.1111/j.1468-3083.2012.04668.x JEADV ORIGINAL ARTICLE Metformin for the treatment of hidradenitis suppurativa: a little help along the way R. Verdolini,† N. Clayton,‡,* A. Smith,‡ N. Alwash,† B. Mannello§ †Department of Dermatology, Princess Alexandra Hospital NHS trust, Harlow, Essex, and ‡Department of Dermatology, The Royal London Hospital, London, UK §Mannello Statistics, Via Rodi, Ancona, Italy *Correspondence: N. Clayton. E-mail: [email protected]; [email protected] Abstract Background Despite recent insights into its aetiology, hidradenitis suppurativa (HS) remains an intractable and debilitating condition for its sufferers, affecting an estimated 2% of the population. It is characterized by chronic, relapsing abscesses, with accompanying fistula formation within the apocrine glandbearing skin, such as the axillae, ano-genital areas and breasts. Standard treatments remain ineffectual and the disease often runs a chronic relapsing course associated with significant psychosocial trauma for its sufferers. Objective To evaluate the clinical efficacy of Metformin in treating cases of HS which have not responded to standard therapies. Methods Twenty-five patients were treated with Metformin over a period of 24 weeks. Clinical severity of the disease was assessed at time 0, then after 12 weeks and finally after 24 weeks. Results were evaluated using Sartorius and DLQI scores. Results Eighteen patients clinically improved with a significant average reduction in their Sartorius score of 12.7 and number of monthly work days lost reduced from 1.5 to 0.4. Dermatology life quality index (DLQI) also showed a significant improvement in 16 cases, with a drop in DLQI score of 7.6. -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F. -

Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) • Definition: O Inflammation Of
Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) Definition: o Inflammation of the hair follicle caused by either chemical/physical irritation or viral/bacterial infection o Folliculitis is the smallest and most minor o Furuncles are larger, carbuncles larger than that, and boils even larger (3) Taken From: http://www.shorthillsderm .com/blog/wp- Common associations: content/uploads/2014/11/ o Diabetes, immunosuppression, shaving What-is-Folliculitis.jpg Diagnosis: o Based on appearance and history o Usually seen on scalp, face, legs, back, chest, axilla o Folliculitis is usually not tender compared to carbuncles and furuncles o If someone has had recent contact w/ hot tub or DM, consider pseudomonas as potential bacteria (3) o May see hyper- or hypopigmentation post infection Tx: o Warm compresses 3 times/day o Antibiotics as treatment of recurrent infections is controversial as increased antibiotic use may lead to increased resistance . Topical mupirocin for moderate folliculitis, more severe infections may require antibiotics . For tx of strep: dicloxacillin or cefadroxil; tx of strep infections helps to prevent PSGN but no effect on rheumatic fever (3) . For tx of pseudomonas: fluoroquinolones or carbapenems or other anti-pseudomonal options . For tx staph (particularly MRSA): 7-10 day course of Bactrim, clindamycin, doxycycline, vancomycin, linezolid,… other antibiotics reserved for more severe infections. (5) o Many people carry MRSA in their nares. Between 10-35% are persistent carriers and 20-75% intermittent carriers. (4) . Should we treat carriers? (Mashhood AA, 2006) recommends nasal Taken from http://riversideonline.com swab testing in all patients with recurrent “furunculosis” aka boils /source/images/image_po aka abscesses. -

RIPE for the PICKING Experts Profile the Future of Biologic Treatments
RIPE FOR THE PICKING Experts profile the future of biologic treatments 22 DERMATOLOGY WORLD // September 2015 www.aad.org/dw BY VICTORIA HOUGHTON, ASSISTANT MANAGING EDITOR John Harris, MD, PhD, assistant professor of medicine at the University of Massachusetts in the division of dermatology — like many dermatologists — has watched the impressive evolution of treatments for psoriasis over the last decade with anticipation. “We initially had very broad immunosuppressants that were somewhat effective in some patients, but they also had significant side effects,” Dr. Harris said. However, “The onset of biologics and other targeted therapies has been incredible. They’ve revolutionized treatment for psoriasis.” However, while physicians are enthusiastic about the progress of these treatments for psoriasis, there is also hope that interest in developing these innovative therapies is increasingly shifting to other skin conditions. “Pharmaceutical companies have to start looking elsewhere, given how good current psoriasis therapies are,” Dr. Harris said. “The real room for growth is in other diseases.” As psoriasis has paved the way for an interest in developing biologic and other targeted treatments in skin conditions, physicians are anticipating a promising future for these treatments in the following conditions: Atopic dermatitis Hidradenitis suppurativa Chronic urticaria Vitiligo Dermatomyositis >> Alopecia areata DERMATOLOGY WORLD // September 2015 23 RIPE FOR THE PICKING Atopic dermatitis 133; 6:1626-34). The study showed that by blocking the According to Lawrence Eichenfield, MD, professor of immune pathways with CsA, the molecular abnormalities dermatology and pediatrics at the University of California, with AD skin barrier genes, such as filaggrin and loricrin, San Diego and chief of pediatric and adolescent dermatology normalized. -

Hidradenitis Suppurativa Hidradenitis Suppurativa (HS) Is an Inflammatory Skin Disease That Many People Mistake for Acne Or Infectious Boils
Dermatology Patient Education Hidradenitis Suppurativa Hidradenitis suppurativa (HS) is an inflammatory skin disease that many people mistake for acne or infectious boils. Another name for HS is acne inversa, which means acne that appears in the skin folds such as the underarms, groin, buttocks, and underneath the breasts. Unlike acne, many people have HS for life. Early diagnosis can help patients receive effective treatment options that will help control symptoms. WHAT DOES HS LOOK LIKE? HS typically looks like acne on a part of the body where you normally would not have acne, particularly on areas of the body where skin touches skin. You may notice: • Pimple-like bumps • Deep acne-like cysts and blackheads • Bumps with a hair coming out of them (folliculitis) • Boils • Scarring Hidradenitis Suppurativa If HS worsens, you may notice that your bumps grow larger, become painful, and feel hot and tender. If HS bumps break open or rupture, they can leak a blood-stained, foul-smelling pus. Once the bumps heal, deep scars can appear that look like tunnels under the skin. These scars can be painful and thicken. You may experience a limited range of motion in the area where the bumps appeared because of scarring and pain. HS is most common in the armpits and groin. It also forms on and under women’s breasts, on the buttocks, and around the anus. As it worsens, HS can appear on skin that receives a lot of friction such as around your waist, the inner thighs, and the back of your neck. It even develops behind the ears, on the scalp, and on the eyelids. -

Common Infections of the Skin Candida of Nails How to Diagnose
Candida of Nails • Occurs in persons who have hands in water • Green nails represent the co‐pathogen which is pseudomonas Common Infections of the Skin TREATMENT: • Fluconazole 150 mg qd x1 month PLUS Ciprofloxacin 500 bid x 2 weeks Toby Maurer, MD OR University of California, San Francisco Thymol 2‐4% soak 20 mins bid x 3 months and tobramycin or gentamycin ophthalmologic drops How to diagnose Onychomycosis • Not all dystrophic nails= onychomycosis • Topical treatment –use for the right type of • KOH‐difficult to do and operator dependent lesions • CULTURE is gold standard but takes 3 weeks to grow out. • Naftin gel for small superficial lesions • Now PCR‐used in Europe with high sensitivity and • Penlac (Ciclopirox 8%) reported to work 35‐ specificity 52% of the time • Cost effective and results in 24‐72 hours – cost: expensive 1 Right type of lesions for topicals • Lunula not affected • Griseofulvin‐least hepatotoxic but lower • Less than 5 nails affected efficacy‐ 250 mg bid x 12‐18 months • No thickening of nails • Fluconazole‐ 150 mg qweek for more than 6 • No separation of nail plate on sides months –July 2012 Dermat Tx Gupta AK et al • Itraconazole‐ can pulse it‐ 400 mg qd x 7 days q month x 4 months Terbinafine (Lamisil) • Still the leader of the pack‐most effective in BASELINE 1 YR 5 YR terms of INITIAL and LONG‐TERM cure rate. • DOSE: 250 mg qd Continuously x 3 months Terbinafine 77% 75% 50% for fingernails and x4 months for toenails Itraconazole 70% 50% 13% (July 2012) i.e. no pulsing Grispeg 41% Fluconazole ? ? ? 2 Liver toxicity What about laser? • Transaminase elevation 0.4% to 1% with • Photo‐ inactivation laser and destructive terbinafine and intraconazole laser • Transaminase elevation does not predict liver • 4 studies‐2 – no results; 2 show results but failure with recurrence. -

Finasteride for the Treatment of Hidradenitis Suppurativa in Children and Adolescents
OBSERVATION Finasteride for the Treatment of Hidradenitis Suppurativa in Children and Adolescents Harkamal Kaur Randhawa, MD; Jill Hamilton, MD; Elena Pope, MD Importance: Hidradenitis suppurativa (HS) is a chronic ity of disease flares with no significant adverse effects. debilitating cutaneous disease for which there is no uni- versally effective treatment. Patients typically present at Conclusions and Relevance: Finasteride is a thera- puberty with tender subcutaneous nodules that can prog- peutic option that provides benefit for pediatric patients ress to dermal abscess formation. Antiandrogens have been with HS. Further prospective data and randomized con- used in the treatment of HS, and studies have primarily trolled studies will provide helpful information in the man- focused on adult patients. agement of this disease. Observations: We present a case series of 3 pediatric JAMA Dermatol. 2013;149(6):732-735. patients with HS who were successfully treated with oral Published online March 20, 2013. finasteride, resulting in decreased frequency and sever- doi:10.1001/jamadermatol.2013.2874 IDRADENITIS SUPPURA- from that of cyproterone acetate, a previ- tiva (HS) is a chronic in- ously studied antiandrogen in patients flammatory disease that with HS. We outline findings in 3 cases primarily involves skin in presenting during childhood, all in pa- the axillae, groin, and tients who showed significant improve- Hanogenital regions, although disease may ment in disease activity with finasteride extend to the buttocks, chest, scalp, eye- treatment. lids, and retroauricular areas.1 Patients with HS develop exquisitely painful erythem- REPORT OF CASES atous subcutaneous nodules that may heal spontaneously or suppurate and coalesce to form dermal abscesses. -

Differential Diagnosis of the Scalp Hair Folliculitis
Acta Clin Croat 2011; 50:395-402 Review DIFFERENTIAL DIAGNOSIS OF THE SCALP HAIR FOLLICULITIS Liborija Lugović-Mihić1, Freja Barišić2, Vedrana Bulat1, Marija Buljan1, Mirna Šitum1, Lada Bradić1 and Josip Mihić3 1University Department of Dermatovenereology, 2University Department of Ophthalmology, Sestre milosrdnice University Hospital Center, Zagreb; 3Department of Neurosurgery, Dr Josip Benčević General Hospital, Slavonski Brod, Croatia SUMMARY – Scalp hair folliculitis is a relatively common condition in dermatological practice and a major diagnostic and therapeutic challenge due to the lack of exact guidelines. Generally, inflammatory diseases of the pilosebaceous follicle of the scalp most often manifest as folliculitis. There are numerous infective agents that may cause folliculitis, including bacteria, viruses and fungi, as well as many noninfective causes. Several noninfectious diseases may present as scalp hair folli- culitis, such as folliculitis decalvans capillitii, perifolliculitis capitis abscendens et suffodiens, erosive pustular dermatitis, lichen planopilaris, eosinophilic pustular folliculitis, etc. The classification of folliculitis is both confusing and controversial. There are many different forms of folliculitis and se- veral classifications. According to the considerable variability of histologic findings, there are three groups of folliculitis: infectious folliculitis, noninfectious folliculitis and perifolliculitis. The diagno- sis of folliculitis occasionally requires histologic confirmation and cannot be based