Minor Procedures
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
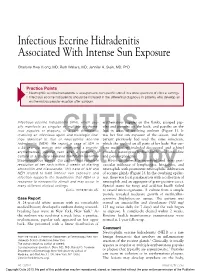
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Proper Preop Makes for Easier Toenail Surgery
April 15, 2007 • www.familypracticenews.com Skin Disorders 25 Proper Preop Makes for Easier Toenail Surgery BY JEFF EVANS sia using a digital block or a distal approach to take ef- Senior Writer fect. Premedication with NSAIDs, codeine, or dextro- propoxyphene also may be appropriate, he said. WASHINGTON — Proper early management of in- To cut away the offending section of nail, an English grown toenails may help to decrease the risk of recur- anvil nail splitter is inserted under the nail plate and the rence whether or not surgery is necessary, Dr. C. Ralph cut is made all the way to the proximal nail fold. The hy- Daniel III said at the annual meeting of the American pertrophic, granulated tissue should be cut away as well. Academy of Dermatology. Many ingrown toenails are recurrent, so Dr. Daniel per- “An ingrown nail is primarily acting as a foreign-body forms a chemical matricectomy in nearly all patients after reaction. That rigid spicule penetrates soft surrounding tis- making sure that the surgical field is dry and bloodless. sue” and produces swelling, granulation tissue, and some- The proximal nail fold can be flared back to expose more times a secondary infection, said Dr. Daniel of the de- of the proximal matrix if necessary. Dr. Daniel inserts a Cal- partments of dermatology at the University of Mississippi, giswab coated with 88% phenol or 10% sodium hydroxide Jackson, and the University of Alabama, Birmingham. and applies the chemical for 30 seconds to the portion of For the early management of stage I ingrown toenails the nail matrix that needs to be destroyed. -

DERMCASE Test Your Knowledge with Multiple-Choice Cases
DERMCASE Test your knowledge with multiple-choice cases This month—5 cases: Case 1 1. “What’s wrong with my feet?” 2. “Doc...what is this spot?” 3. “My toenail looks funny!” 4. A foot problem 5. “What’s this rash?” “What’s wrong with my feet?” This 60-year-old woman has had a problem with her feet for several years. What can it be? a. Contact dermatitis b. Pustular psoriasis c. Dyshidrotic eczema d. Mycoses fungoides e. Tinea pedis Answer Pustular psoriasis (answer b) frequently involves the palms and soles. While it does The following have also been used with occur in both sexes, it is most common in mid- varying degrees of success: dle-aged women. It is characterized by recur- • oral etretinate, rent sterile pustules on an erythematous base. • tetracycline, As the pustules dry, they form brown spots. • cyclosporin and The cause of pustular psoriasis is unknown • methotrexate. and once it is established, it can last for years. Cigarette smoking has been associated with There is significant morbidity related to chron- this condition and should be discouraged. ic itch, pain and fissuring. Treatment options consists of: • oil soaks, • emollient creams and ointments, • topical steroids and • retinoid gels. Stanley Wine, MD, FRCPC, is a Dermatologist, Toronto, Ontario. The Canadian Journal of CME / June 2006 63 DERMCASE Case 2 “Doc...what is this spot?” A 42-year-old male presents with a well- defined erythematous atrophic patch with a ker- atotic, raised border. What is it? a. Squamous cell carcinoma b. Bowen’s disease c. Porokeratosis of Mibelli d. -

Dermatology DDX Deck, 2Nd Edition 65
63. Herpes simplex (cold sores, fever blisters) PREMALIGNANT AND MALIGNANT NON- 64. Varicella (chicken pox) MELANOMA SKIN TUMORS Dermatology DDX Deck, 2nd Edition 65. Herpes zoster (shingles) 126. Basal cell carcinoma 66. Hand, foot, and mouth disease 127. Actinic keratosis TOPICAL THERAPY 128. Squamous cell carcinoma 1. Basic principles of treatment FUNGAL INFECTIONS 129. Bowen disease 2. Topical corticosteroids 67. Candidiasis (moniliasis) 130. Leukoplakia 68. Candidal balanitis 131. Cutaneous T-cell lymphoma ECZEMA 69. Candidiasis (diaper dermatitis) 132. Paget disease of the breast 3. Acute eczematous inflammation 70. Candidiasis of large skin folds (candidal 133. Extramammary Paget disease 4. Rhus dermatitis (poison ivy, poison oak, intertrigo) 134. Cutaneous metastasis poison sumac) 71. Tinea versicolor 5. Subacute eczematous inflammation 72. Tinea of the nails NEVI AND MALIGNANT MELANOMA 6. Chronic eczematous inflammation 73. Angular cheilitis 135. Nevi, melanocytic nevi, moles 7. Lichen simplex chronicus 74. Cutaneous fungal infections (tinea) 136. Atypical mole syndrome (dysplastic nevus 8. Hand eczema 75. Tinea of the foot syndrome) 9. Asteatotic eczema 76. Tinea of the groin 137. Malignant melanoma, lentigo maligna 10. Chapped, fissured feet 77. Tinea of the body 138. Melanoma mimics 11. Allergic contact dermatitis 78. Tinea of the hand 139. Congenital melanocytic nevi 12. Irritant contact dermatitis 79. Tinea incognito 13. Fingertip eczema 80. Tinea of the scalp VASCULAR TUMORS AND MALFORMATIONS 14. Keratolysis exfoliativa 81. Tinea of the beard 140. Hemangiomas of infancy 15. Nummular eczema 141. Vascular malformations 16. Pompholyx EXANTHEMS AND DRUG REACTIONS 142. Cherry angioma 17. Prurigo nodularis 82. Non-specific viral rash 143. Angiokeratoma 18. Stasis dermatitis 83. -

Coexistence of Antibodies to Tick-Borne
Mem Inst Oswaldo Cruz, Rio de Janeiro, Vol. 98(3): 311-318, April 2003 311 Coexistence of Antibodies to Tick-borne Agents of Babesiosis and Lyme Borreliosis in Patients from Cotia County, State of São Paulo, Brazil Natalino Hajime Yoshinari/+, Milena Garcia Abrão, Virginia Lúcia Nazário Bonoldi, Cleber Oliveira Soares*, Claudio Roberto Madruga*, Alessandra Scofield**, Carlos Luis Massard**, Adivaldo Henrique da Fonseca** Laboratório de Investigação em Reumatologia (LIM-17), Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo, Av. Dr. Arnaldo 455, 3º andar, 01246-903 São Paulo, SP, Brasil *Embrapa Gado de Corte, Campo Grande, MS, Brasil **Universidade Federal Rural do Rio de Janeiro, Seropédica, RJ, Brasil This paper reports a case of coinfection caused by pathogens of Lyme disease and babesiosis in brothers. This was the first case of borreliosis in Brazil, acquired in Cotia County, State of São Paulo, Brazil. Both children had tick bite history, presented erythema migrans, fever, arthralgia, mialgia, and developed positive serology (ELISA and Western-blotting) directed to Borrelia burgdorferi G 39/40 and Babesia bovis antigens, mainly of IgM class antibodies, suggestive of acute disease. Also, high frequencies of antibodies to B. bovis was observed in a group of 59 Brazilian patients with Lyme borreliosis (25.4%), when compared with that obtained in a normal control group (10.2%) (chi-square = 5.6; p < 0.05). Interestingly, both children presented the highest titers for IgM antibodies directed to both infective diseases, among all patients with Lyme borreliosis. Key words: lyme borreliosis - lyme disease - spirochetosis - borreliosis - babesiosis - coinfection - tick-borne disease - Brazil Babesiosis is a tick-borne disease distributed world- The first case of babesiosis in a healthy person, with wide, caused by hemoprotozoans of the genus Babesia, intact spleen, was reported in 1969 in a woman from Nan- which infects wild and domestic animals, promoting eco- tucket Island (Massachusetts, USA)(Wester et al. -

Nail Problems
Nail Problems Components of the Nail Congenital Disorders Racket nails, characterized by a broad short thumb nail, is the commonest congenital nail defect, dominantly inherited and seen in 1% of the population. The basic abnormality is shortness of the underlying terminal phalanx. In the yellow nail syndrome, the nail changes begin in adult life, against a background of hypoplasia of the lymphatic system. Peripheral edema is usually present and pleural effusions may occur. The nails grow very slowly and become thickened and greenish-yellow; their surface is smooth but they are over curved from side to side. Acquired Nail Changes Beau's Lines Transverse lines or grooves in nail. Causes include any severe systemic illness or medications (chemotherapy), which affects growth of the nail matrix. Clinically: The grooves or lines move distally; the distance from the nail fold lets one assess the time of trauma. Onycholysis Separation of nail from nail bed. Causes include psoriasis, dermatitis, fungal infections; medications (photo-onycholysis from tetracyclines or psoralens), thyroid disease; rarely inherited. Idiopathic onycholysis is most common among women; painless separation of nail without apparent cause. Typically, the distal third separates and underlying nail bed becomes darker and thickened. Therapy: Cut nail very short to reduce leverage encouraging separation, apply antifungal solution. Usually self-limited process. Ingrown Nail Penetration of nail plate into tissue of lateral nail fold. Almost always involves great toes. Causes include congenital malformation of nail (pincer nail), improper trimming, and tightly fitting shoes. Clinically: Distorted nail with swelling, pain, and granulation tissue along the lateral nail fold. Therapy: Mild cases: Eliminate pressure, trim nail; topical antiseptics as foot soaks or on small piece of cotton wool pushed under affected nail. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Bacterial Infections Diseases Picture Cause Basic Lesion
page: 117 Chapter 6: alphabetical Bacterial infections diseases picture cause basic lesion search contents print last screen viewed back next Bacterial infections diseases Impetigo page: 118 6.1 Impetigo alphabetical Bullous impetigo Bullae with cloudy contents, often surrounded by an erythematous halo. These bullae rupture easily picture and are rapidly replaced by extensive crusty patches. Bullous impetigo is classically caused by Staphylococcus aureus. cause basic lesion Basic Lesions: Bullae; Crusts Causes: Infection search contents print last screen viewed back next Bacterial infections diseases Impetigo page: 119 alphabetical Non-bullous impetigo Erythematous patches covered by a yellowish crust. Lesions are most frequently around the mouth. picture Lesions around the nose are very characteristic and require prolonged treatment. ß-Haemolytic streptococcus is cause most frequently found in this type of impetigo. basic lesion Basic Lesions: Erythematous Macule; Crusts Causes: Infection search contents print last screen viewed back next Bacterial infections diseases Ecthyma page: 120 6.2 Ecthyma alphabetical Slow and gradually deepening ulceration surmounted by a thick crust. The usual site of ecthyma are the legs. After healing there is a permanent scar. The pathogen is picture often a streptococcus. Ecthyma is very common in tropical countries. cause basic lesion Basic Lesions: Crusts; Ulcers Causes: Infection search contents print last screen viewed back next Bacterial infections diseases Folliculitis page: 121 6.3 Folliculitis -

Proper Preop Makes for Easier Toenail Surgery
20 Dermatologic Surgery S KIN & ALLERGY N EWS • April 2007 Proper Preop Makes for Easier Toenail Surgery BY JEFF EVANS produces swelling, granulation tissue, and tor or a 1- to 2-mm curette. has served as a speaker, consultant, and in- Senior Writer sometimes a secondary infection, said Dr. He also uses a technique for early-stage vestigator for the company. Daniel of the departments of dermatol- ingrown toenails in which dental floss is in- A procedure that uses an acrylic-affixed WASHINGTON — Proper early man- ogy at the University of Mississippi, Jack- serted under the ingrown nail corner with- gutter splint has been reported to be suc- agement of ingrown toenails may help to son, and the University of Alabama, Birm- out anesthesia and is kept there to separate cessful for avoiding surgery, Dr. Daniel decrease the risk of recurrence whether or ingham. the nail edge from adjacent soft tissue (J. said. A plastic gutter tube is set under the not surgery is necessary, Dr. C. Ralph For the early management of stage I in- Am. Acad. Dermatol. 2004;50:939-40). ingrown part of the nail and acrylic is Daniel III said at the annual meeting of the grown toenails in which some granula- Dr. Daniel formerly was on the board of sculpted and allowed to polymerize American Academy of Dermatology. tion tissue but no infection is present, Dr. directors for Doak Dermatologics, a sub- around the ingrown part of the nail and “An ingrown nail is primarily acting as Daniel has trained his nurse to push wisps sidiary of Bradley Pharmaceuticals Inc., hold the gutter tube in place. -

Abscesses Are a Serious Problem for People Who Shoot Drugs
Where to Get Your Abscess Seen Abscesses are a serious problem for people who shoot drugs. But what the hell are they and where can you go for care? What are abscesses? Abscesses are pockets of bacteria and pus underneath you skin and occasionally in your muscle. Your body creates a wall around the bacteria in order to keep the bacteria from infecting your whole body. Another name for an abscess is a “soft tissues infection”. What are bacteria? Bacteria are microscopic organisms. Bacteria are everywhere in our environment and a few kinds cause infections and disease. The main bacteria that cause abscesses are: staphylococcus (staff-lo-coc-us) aureus (or-e-us). How can you tell when you have an abscess? Because they are pockets of infection abscesses cause swollen lumps under the skin which are often red (or in darker skinned people darker than the surrounding skin) warm to the touch and painful (often VERY painful). What is the worst thing that can happen? The worst thing that can happen with abscesses is that they can burst under your skin and cause a general infection of your whole body or blood. An all over bacterial infection can kill you. Another super bad thing that can happen is a endocarditis, which is an infection of the lining of your heart, and “septic embolism”, which means that a lump of the contaminates in your abscess get loose in your body and lodge in your lungs or brain. Why do abscesses happen? Abscesses are caused when bad bacteria come in to contact with healthy flesh. -

Cellulitis (You Say, Sell-You-Ly-Tis)
Cellulitis (you say, sell-you-ly-tis) Any area of skin can become infected with cellulitis if the skin is broken, for example from a sore, insect bite, boil, rash, cut, burn or graze. Cellulitis can also infect the flesh under the skin if it is damaged or bruised or if there is poor circulation. Signs your child has cellulitis: The skin will look red, and feel warm and painful to touch. There may be pus or fluid leaking from the skin. The skin may start swelling. The red area keeps growing. Gently mark the edge of the infected red area How is with a pen to see if the red area grows bigger. cellulitis spread? Red lines may appear in the skin spreading out from the centre of the infection. Bad bacteria (germs) gets into broken skin such as a cut or insect bite. What to do Wash your hands before and Cellulitis is a serious infection that needs to after touching the infected area. be treated with antibiotics. Keep your child’s nails short and Go to the doctor if the infected area is clean. painful or bigger than a 10 cent piece. Don’t let your child share Go to the doctor immediately if cellulitis is bath water, towels, sheets and near an eye as this can be very serious. clothes. Make sure your child takes the antibiotics Make sure your child rests every day until they are finished, even if and eats plenty of fruit and the infection seems to have cleared up. The vegetables and drinks plenty of antibiotics need to keep killing the infection water. -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin.