Aars Hot Topics Member Newsletter
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chloracne: from Clinic to Research
DERMATOLOGICA SINICA 30 (2012) 2e6 Contents lists available at SciVerse ScienceDirect Dermatologica Sinica journal homepage: http://www.derm-sinica.com REVIEW ARTICLE Chloracne: From clinic to research Qiang Ju 1, Kuochia Yang 2, Christos C. Zouboulis 3, Johannes Ring 4, Wenchieh Chen 4,* 1 Department of Dermatology, Shanghai Skin Disease and STD Hospital, Shanghai, People’s Republic of China 2 Department of Dermatology, Changhua Christian Hospital, Changhua, Taiwan 3 Departments of Dermatology, Venereology, Allergology and Immunology, Dessau Medical Center, Dessau, Germany 4 Department of Dermatology and Allergy, Technische Universität München, Munich, Germany article info abstract Article history: Chloracne is the most sensitive and specific marker for a possible dioxin (2,3,7,8-tetrachlorodibenzo-p- Received: Oct 31, 2011 dioxin) intoxication. It is clinically characterized by multiple acneiform comedone-like cystic eruptions Revised: Nov 9, 2011 mainly involving face in the malar, temporal, mandibular, auricular/retroauricular regions, and the Accepted: Nov 9, 2011 genitalia, often occurring in age groups not typical for acne vulgaris. Histopathology is essential for adefinite diagnosis, which exhibits atrophy or absence of sebaceous glands as well as infundibular Keywords: dilatation or cystic formation of hair follicles, hyperplasia of epidermis, and hyperpigmentation of aryl hydrocarbon receptor stratum corneum. The appearance of chloracne and its clinical severity does not correlate with the blood chloracne “ ” 2,3,7,8-tetrachlorodibenzo-p-dioxin levels of dioxins. Pathogenesis of chloracne remains largely unclear. An aryl hydrocarbon receptor - polyhalogenated aromatic hydrocarbons mediated signaling pathway affecting the multipotent stem cells in the pilosebaceous units is probably sebaceous gland the major molecular mechanism inducing chloracne. -
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
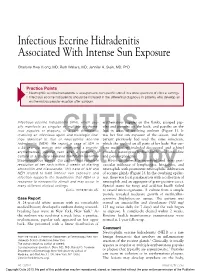
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Endocrinology 12 Michel Faure, Evelyne Drapier-Faure
Chapter 12 Endocrinology 12 Michel Faure, Evelyne Drapier-Faure Key points 12.1 Introduction Q HS does not generally appear to be In 1986 Mortimer et al. [14] reported that hi- associated with signs of hyperan- dradenitis suppurativa (HS) responded to treat- drogenism ment with the potent antiandrogen cyproterone acetate. They suggested that the disease could Q Sex hormones may affect the course of be androgen-dependent [8]. This hypothesis HS indirectly through, for example, was also upheld by occasional reports of women their effects on inflammation with HS under antiandrogen therapy [18]. Actu- ally, the androgen dependence of HS (similarly Q The role of end-organ sensitivity to acne) is only poorly substantiated. cannot be excluded at the time of writing 12.2 Hyperandrogenism and the Skin Q The prevalence of polycystic ovary syndrome in HS has not been system- Androgen-dependent disorders encompass a atically investigated broad spectrum of overlapping entities that may be related in women to the clinical consequenc- es of the effects of androgens on target tissues and of associated endocrine and metabolic dys- functions, when present. #ONTENTS 12.1 Introduction ...........................95 12.2.1 Androgenization 12.2 Hyperandrogenism and the Skin .........95 12.2.1 Androgenization .......................95 One of the less sex-specific effects of androgens 12.2.2 Androgen Metabolism ..................96 12.2.3 Causes of Hyperandrogenism ...........96 is that on the skin and its appendages, and in particular their action on the pilosebaceous 12.3 Lack of Association between HS unit. Hirsutism is the major symptom of hyper- and Endocrinopathies ..................97 androgenism in women. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Compensation for Occupational Skin Diseases
ORIGINAL ARTICLE http://dx.doi.org/10.3346/jkms.2014.29.S.S52 • J Korean Med Sci 2014; 29: S52-58 Compensation for Occupational Skin Diseases Han-Soo Song1 and Hyun-chul Ryou2 The Korean list of occupational skin diseases was amended in July 2013. The past list was constructed according to the causative agent and the target organ, and the items of that 1 Department of Occupational and Environmental list had not been reviewed for a long period. The revised list was reconstructed to include Medicine, College of Medicine, Chosun University, Gwangju; 2Teo Center of Occupational and diseases classified by the International Classification of Diseases (10th version). Therefore, Environmental Medicine, Changwon, Korea the items of compensable occupational skin diseases in the amended list in Korea comprise contact dermatitis; chemical burns; Stevens-Johnson syndrome; tar-related skin diseases; Received: 19 December 2013 infectious skin diseases; skin injury-induced cellulitis; and skin conditions resulting from Accepted: 2 May 2014 physical factors such as heat, cold, sun exposure, and ionized radiation. This list will be Address for Correspondence: more practical and convenient for physicians and workers because it follows a disease- Han-Soo Song, MD based approach. The revised list is in accordance with the International Labor Organization Department of Occupational and Environmental Medicine, Chosun University Hospital, 365 Pilmun-daero, Dong-gu, list and is refined according to Korean worker’s compensation and the actual occurrence of Gwangju 501-717, Korea occupational skin diseases. However, this revised list does not perfectly reflect the actual Tel: +82.62-220-3689, Fax: +82.62-443-5035 E-mail: [email protected] status of skin diseases because of the few cases of occupational skin diseases, incomplete statistics of skin diseases, and insufficient scientific evidence. -

General Dermatology an Atlas of Diagnosis and Management 2007
An Atlas of Diagnosis and Management GENERAL DERMATOLOGY John SC English, FRCP Department of Dermatology Queen's Medical Centre Nottingham University Hospitals NHS Trust Nottingham, UK CLINICAL PUBLISHING OXFORD Clinical Publishing An imprint of Atlas Medical Publishing Ltd Oxford Centre for Innovation Mill Street, Oxford OX2 0JX, UK tel: +44 1865 811116 fax: +44 1865 251550 email: [email protected] web: www.clinicalpublishing.co.uk Distributed in USA and Canada by: Clinical Publishing 30 Amberwood Parkway Ashland OH 44805 USA tel: 800-247-6553 (toll free within US and Canada) fax: 419-281-6883 email: [email protected] Distributed in UK and Rest of World by: Marston Book Services Ltd PO Box 269 Abingdon Oxon OX14 4YN UK tel: +44 1235 465500 fax: +44 1235 465555 email: [email protected] © Atlas Medical Publishing Ltd 2007 First published 2007 All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any form or by any means, without the prior permission in writing of Clinical Publishing or Atlas Medical Publishing Ltd. Although every effort has been made to ensure that all owners of copyright material have been acknowledged in this publication, we would be glad to acknowledge in subsequent reprints or editions any omissions brought to our attention. A catalogue record of this book is available from the British Library ISBN-13 978 1 904392 76 7 Electronic ISBN 978 1 84692 568 9 The publisher makes no representation, express or implied, that the dosages in this book are correct. Readers must therefore always check the product information and clinical procedures with the most up-to-date published product information and data sheets provided by the manufacturers and the most recent codes of conduct and safety regulations. -

Metformin for the Treatment of Hidradenitis Suppurativa: a Little Help Along the Way
DOI: 10.1111/j.1468-3083.2012.04668.x JEADV ORIGINAL ARTICLE Metformin for the treatment of hidradenitis suppurativa: a little help along the way R. Verdolini,† N. Clayton,‡,* A. Smith,‡ N. Alwash,† B. Mannello§ †Department of Dermatology, Princess Alexandra Hospital NHS trust, Harlow, Essex, and ‡Department of Dermatology, The Royal London Hospital, London, UK §Mannello Statistics, Via Rodi, Ancona, Italy *Correspondence: N. Clayton. E-mail: [email protected]; [email protected] Abstract Background Despite recent insights into its aetiology, hidradenitis suppurativa (HS) remains an intractable and debilitating condition for its sufferers, affecting an estimated 2% of the population. It is characterized by chronic, relapsing abscesses, with accompanying fistula formation within the apocrine glandbearing skin, such as the axillae, ano-genital areas and breasts. Standard treatments remain ineffectual and the disease often runs a chronic relapsing course associated with significant psychosocial trauma for its sufferers. Objective To evaluate the clinical efficacy of Metformin in treating cases of HS which have not responded to standard therapies. Methods Twenty-five patients were treated with Metformin over a period of 24 weeks. Clinical severity of the disease was assessed at time 0, then after 12 weeks and finally after 24 weeks. Results were evaluated using Sartorius and DLQI scores. Results Eighteen patients clinically improved with a significant average reduction in their Sartorius score of 12.7 and number of monthly work days lost reduced from 1.5 to 0.4. Dermatology life quality index (DLQI) also showed a significant improvement in 16 cases, with a drop in DLQI score of 7.6. -

Acne in Childhood: an Update Wendy Kim, DO; and Anthony J
FEATURE Acne in Childhood: An Update Wendy Kim, DO; and Anthony J. Mancini, MD cne is the most common chron- ic skin disease affecting chil- A dren and adolescents, with an 85% prevalence rate among those aged 12 to 24 years.1 However, recent data suggest a younger age of onset is com- mon and that teenagers only comprise 36.5% of patients with acne.2,3 This ar- ticle provides an overview of acne, its pathophysiology, and contemporary classification; reviews treatment op- tions; and reviews recently published algorithms for treating acne of differing levels of severity. Acne can be classified based on le- sion type (morphology) and the age All images courtesy of Anthony J. Mancini, MD. group affected.4 The contemporary Figure 1. Comedonal acne. This patient has numerous closed comedones (ie, “whiteheads”). classification of acne based on sev- eral recent reviews is addressed below. Acne lesions (see Table 1, page 419) can be divided into noninflammatory lesions (open and closed comedones, see Figure 1) and inflammatory lesions (papules, pustules, and nodules, see Figure 2). The comedone begins with Wendy Kim, DO, is Assistant Professor of In- ternal Medicine and Pediatrics, Division of Der- matology, Loyola University Medical Center, Chicago. Anthony J. Mancini, MD, is Professor of Pediatrics and Dermatology, Northwestern University Feinberg School of Medicine, Ann and Robert H. Lurie Children’s Hospital of Chi- cago. Address correspondence to: Anthony J. Man- Figure 2. Moderate mixed acne. In this patient, a combination of closed comedones, inflammatory pap- ules, and pustules can be seen. cini, MD, Division of Dermatology Box #107, Ann and Robert H. -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F. -

Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) • Definition: O Inflammation Of
Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) Definition: o Inflammation of the hair follicle caused by either chemical/physical irritation or viral/bacterial infection o Folliculitis is the smallest and most minor o Furuncles are larger, carbuncles larger than that, and boils even larger (3) Taken From: http://www.shorthillsderm .com/blog/wp- Common associations: content/uploads/2014/11/ o Diabetes, immunosuppression, shaving What-is-Folliculitis.jpg Diagnosis: o Based on appearance and history o Usually seen on scalp, face, legs, back, chest, axilla o Folliculitis is usually not tender compared to carbuncles and furuncles o If someone has had recent contact w/ hot tub or DM, consider pseudomonas as potential bacteria (3) o May see hyper- or hypopigmentation post infection Tx: o Warm compresses 3 times/day o Antibiotics as treatment of recurrent infections is controversial as increased antibiotic use may lead to increased resistance . Topical mupirocin for moderate folliculitis, more severe infections may require antibiotics . For tx of strep: dicloxacillin or cefadroxil; tx of strep infections helps to prevent PSGN but no effect on rheumatic fever (3) . For tx of pseudomonas: fluoroquinolones or carbapenems or other anti-pseudomonal options . For tx staph (particularly MRSA): 7-10 day course of Bactrim, clindamycin, doxycycline, vancomycin, linezolid,… other antibiotics reserved for more severe infections. (5) o Many people carry MRSA in their nares. Between 10-35% are persistent carriers and 20-75% intermittent carriers. (4) . Should we treat carriers? (Mashhood AA, 2006) recommends nasal Taken from http://riversideonline.com swab testing in all patients with recurrent “furunculosis” aka boils /source/images/image_po aka abscesses. -

Understanding Hidradenitis Suppurativa (Hs)
UNDERSTANDING HIDRADENITIS SUPPURATIVA (HS) Information to help you work with your doctor so you can better manage your HS WHAT’S INSIDE Hidradenitis suppurativa (HS) in brief . 4 HS – the facts . 5 Living with HS . 9 Coping with HS . 11 Tips and tricks for living with HS . 12 Addressing your thoughts and feelings . 14 Coping with stress . 16 Working with your health care team . 17 Symptom self-assessment questionnaire . 19 Useful online resources . 23 3 HIDRADENITIS SUPPURATIVA (HS) IN BRIEF You have been diagnosed with HS, a disease which is: PAINFUL PRORESSIVE INFLAMMATORY GETTING WORSE CAUSING OVER TIME SWELLING CHRONIC SYSTEMIC LASTING AFFECTING A LONG TIME THE WHOLE BODY HS is known to produce lesions in the skin that are inflamed (swollen), recurrent (reappearing after lesions disappear), and chronic (lasting a long period of time). HS can have both a physical and psychological impact. The resulting pain and affected areas of your skin can restrict movement and your ability to do day-to-day tasks. Because of the areas of the body affected and how unsightly, smelly, and uncomfortable or painful HS may be, it can also lead to negative feelings such as embarrassment, stress and low mood. While we understand this is how some people with HS may feel, it’s important to remember that HS is a medical condition — its development is not your fault. 4 It’s important to be able to manage the physical side of the condition while also trying to reduce any feelings of embarrassment you may feel. There is more information about addressing your thoughts and feelings on page 14.