Hair and Nails
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
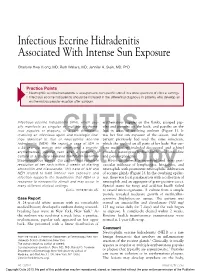
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Abnormal Hair Follicle Development and Altered Cell Fate of Follicular
ERRATUM Development 137, 1775 (2010) doi:10.1242/dev.053116 Abnormal hair follicle development and altered cell fate of follicular keratinocytes in transgenic mice expressing Np63 Rose-Anne Romano, Kirsten Smalley, Song Liu and Satrajit Sinha There was a technical problem with the ePress version of Development 137, 1431-1439 published on 24 March 2010. A number of Greek symbols were missing from the text and figure headings in the Results section. A replacement ePress article was published on 31 March 2010. The online issue and print copy are correct. We apologise to authors and readers for this error. DEVELOPMENT AND STEM CELLS RESEARCH ARTICLE 1431 Development 137, 1431-1439 (2010) doi:10.1242/dev.045427 © 2010. Published by The Company of Biologists Ltd Abnormal hair follicle development and altered cell fate of follicular keratinocytes in transgenic mice expressing DNp63a Rose-Anne Romano1, Kirsten Smalley1, Song Liu2,3 and Satrajit Sinha1,* SUMMARY The transcription factor p63 plays an essential role in epidermal morphogenesis. Animals lacking p63 fail to form many ectodermal organs, including the skin and hair follicles. Although the indispensable role of p63 in stratified epithelial skin development is well established, relatively little is known about this transcriptional regulator in directing hair follicle morphogenesis. Here, using specific antibodies, we have established the expression pattern of DNp63 in hair follicle development and cycling. DNp63 is expressed in the developing hair placode, whereas in mature hair its expression is restricted to the outer root sheath (ORS), matrix cells and to the stem cells of the hair follicle bulge. To investigate the role of DNp63 in hair follicle morphogenesis and cycling, we have utilized a Tet-inducible mouse model system with targeted expression of this isoform to the ORS of the hair follicle. -

Anatomy and Physiology of Hair
Chapter 2 Provisional chapter Anatomy and Physiology of Hair Anatomy and Physiology of Hair Bilgen Erdoğan ğ AdditionalBilgen Erdo informationan is available at the end of the chapter Additional information is available at the end of the chapter http://dx.doi.org/10.5772/67269 Abstract Hair is one of the characteristic features of mammals and has various functions such as protection against external factors; producing sebum, apocrine sweat and pheromones; impact on social and sexual interactions; thermoregulation and being a resource for stem cells. Hair is a derivative of the epidermis and consists of two distinct parts: the follicle and the hair shaft. The follicle is the essential unit for the generation of hair. The hair shaft consists of a cortex and cuticle cells, and a medulla for some types of hairs. Hair follicle has a continuous growth and rest sequence named hair cycle. The duration of growth and rest cycles is coordinated by many endocrine, vascular and neural stimuli and depends not only on localization of the hair but also on various factors, like age and nutritional habits. Distinctive anatomy and physiology of hair follicle are presented in this chapter. Extensive knowledge on anatomical and physiological aspects of hair can contribute to understand and heal different hair disorders. Keywords: hair, follicle, anatomy, physiology, shaft 1. Introduction The hair follicle is one of the characteristic features of mammals serves as a unique miniorgan (Figure 1). In humans, hair has various functions such as protection against external factors, sebum, apocrine sweat and pheromones production and thermoregulation. The hair also plays important roles for the individual’s social and sexual interaction [1, 2]. -

Fungal Infections from Human and Animal Contact
Journal of Patient-Centered Research and Reviews Volume 4 Issue 2 Article 4 4-25-2017 Fungal Infections From Human and Animal Contact Dennis J. Baumgardner Follow this and additional works at: https://aurora.org/jpcrr Part of the Bacterial Infections and Mycoses Commons, Infectious Disease Commons, and the Skin and Connective Tissue Diseases Commons Recommended Citation Baumgardner DJ. Fungal infections from human and animal contact. J Patient Cent Res Rev. 2017;4:78-89. doi: 10.17294/2330-0698.1418 Published quarterly by Midwest-based health system Advocate Aurora Health and indexed in PubMed Central, the Journal of Patient-Centered Research and Reviews (JPCRR) is an open access, peer-reviewed medical journal focused on disseminating scholarly works devoted to improving patient-centered care practices, health outcomes, and the patient experience. REVIEW Fungal Infections From Human and Animal Contact Dennis J. Baumgardner, MD Aurora University of Wisconsin Medical Group, Aurora Health Care, Milwaukee, WI; Department of Family Medicine and Community Health, University of Wisconsin School of Medicine and Public Health, Madison, WI; Center for Urban Population Health, Milwaukee, WI Abstract Fungal infections in humans resulting from human or animal contact are relatively uncommon, but they include a significant proportion of dermatophyte infections. Some of the most commonly encountered diseases of the integument are dermatomycoses. Human or animal contact may be the source of all types of tinea infections, occasional candidal infections, and some other types of superficial or deep fungal infections. This narrative review focuses on the epidemiology, clinical features, diagnosis and treatment of anthropophilic dermatophyte infections primarily found in North America. -

Pediatric and Adolescent Dermatology
Pediatric and adolescent dermatology Management and referral guidelines ICD-10 guide • Acne: L70.0 acne vulgaris; L70.1 acne conglobata; • Molluscum contagiosum: B08.1 L70.4 infantile acne; L70.5 acne excoriae; L70.8 • Nevi (moles): Start with D22 and rest depends other acne; or L70.9 acne unspecified on site • Alopecia areata: L63 alopecia; L63.0 alopecia • Onychomycosis (nail fungus): B35.1 (capitis) totalis; L63.1 alopecia universalis; L63.8 other alopecia areata; or L63.9 alopecia areata • Psoriasis: L40.0 plaque; L40.1 generalized unspecified pustular psoriasis; L40.3 palmoplantar pustulosis; L40.4 guttate; L40.54 psoriatic juvenile • Atopic dermatitis (eczema): L20.82 flexural; arthropathy; L40.8 other psoriasis; or L40.9 L20.83 infantile; L20.89 other atopic dermatitis; or psoriasis unspecified L20.9 atopic dermatitis unspecified • Scabies: B86 • Hemangioma of infancy: D18 hemangioma and lymphangioma any site; D18.0 hemangioma; • Seborrheic dermatitis: L21.0 capitis; L21.1 infantile; D18.00 hemangioma unspecified site; D18.01 L21.8 other seborrheic dermatitis; or L21.9 hemangioma of skin and subcutaneous tissue; seborrheic dermatitis unspecified D18.02 hemangioma of intracranial structures; • Tinea capitis: B35.0 D18.03 hemangioma of intraabdominal structures; or D18.09 hemangioma of other sites • Tinea versicolor: B36.0 • Hyperhidrosis: R61 generalized hyperhidrosis; • Vitiligo: L80 L74.5 focal hyperhidrosis; L74.51 primary focal • Warts: B07.0 verruca plantaris; B07.8 verruca hyperhidrosis, rest depends on site; L74.52 vulgaris (common warts); B07.9 viral wart secondary focal hyperhidrosis unspecified; or A63.0 anogenital warts • Keratosis pilaris: L85.8 other specified epidermal thickening 1 Acne Treatment basics • Tretinoin 0.025% or 0.05% cream • Education: Medications often take weeks to work AND and the patient’s skin may get “worse” (dry and red) • Clindamycin-benzoyl peroxide 1%-5% gel in the before it gets better. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G
Isotretinoin Induced Periungal Pyogenic Granuloma Resolution with Combination Therapy Jonathan G. Bellew, DO, PGY3; Chad Taylor, DO; Jaldeep Daulat, DO; Vernon T. Mackey, DO Advanced Desert Dermatology & Mohave Centers for Dermatology and Plastic Surgery, Peoria, AZ & Las Vegas, NV Abstract Management & Clinical Course Discussion Conclusion Pyogenic granulomas are vascular hyperplasias presenting At the time of the periungal eruption on the distal fingernails, Excess granulation tissue and pyogenic granulomas have It has been reported that the resolution of excess as red papules, polyps, or nodules on the gingiva, fingers, the patient was undergoing isotretinoin therapy for severe been described in both previous acne scars and periungal granulation tissue secondary to systemic retinoid therapy lips, face and tongue of children and young adults. Most nodulocystic acne with significant scarring. He was in his locations.4 Literature review illustrates rare reports of this occurs on withdrawal of isotretinoin.7 Unfortunately for our commonly they are associated with trauma, but systemic fifth month of isotretinoin therapy with a cumulative dose of adverse event. In addition, the mechanism by which patient, discontinuation of isotretinoin and prevention of retinoids have rarely been implicated as a causative factor 140 mg/kg. He began isotretinoin therapy at a dose of 40 retinoids cause excess granulation tissue of the skin is not secondary infection in areas of excess granulation tissue in their appearance. mg daily (0.52 mg/kg/day) for the first month and his dose well known. According to the available literature, a course was insufficient in resolving these lesions. To date, there is We present a case of eruptive pyogenic granulomas of the later increased to 80 mg daily (1.04 mg/kg/day). -

Nestin Expression in Hair Follicle Sheath Progenitor Cells
Nestin expression in hair follicle sheath progenitor cells Lingna Li*, John Mignone†, Meng Yang*, Maja Matic‡, Sheldon Penman§, Grigori Enikolopov†, and Robert M. Hoffman*¶ *AntiCancer, Inc., 7917 Ostrow Street, San Diego, CA 92111; †Cold Spring Harbor Laboratory, 1 Bungtown Road, Cold Spring Harbor, NY 11724; §Department of Biology, Massachusetts Institute of Technology, 77 Massachusetts Avenue, Cambridge, MA 02139-4307; and ‡Stony Brook University, Stony Brook, NY 11794 Contributed by Sheldon Penman, June 25, 2003 The intermediate filament protein, nestin, marks progenitor expression of the neural stem cell protein nestin in hair follicle cells of the CNS. Such CNS stem cells are selectively labeled by stem cells suggests a possible relation. placing GFP under the control of the nestin regulatory se- quences. During early anagen or growth phase of the hair Materials and Methods follicle, nestin-expressing cells, marked by GFP fluorescence in Nestin-GFP Transgenic Mice. Nestin is an intermediate filament nestin-GFP transgenic mice, appear in the permanent upper hair (IF) gene that is a marker for CNS progenitor cells and follicle immediately below the sebaceous glands in the follicle neuroepithelial stem cells (5). Enhanced GFP (EGFP) trans- bulge. This is where stem cells for the hair follicle outer-root genic mice carrying EGFP under the control of the nestin sheath are thought to be located. The relatively small, oval- second-intron enhancer are used for studying and visualizing shaped, nestin-expressing cells in the bulge area surround the the self-renewal and multipotency of CNS stem cells (5–7). hair shaft and are interconnected by short dendrites. The precise Here we report that hair follicle stem cells strongly express locations of the nestin-expressing cells in the hair follicle vary nestin as evidenced by nestin-regulated EGFP expression. -

Management of Cicatricial Alopecia by Hair Transplantation Using Follicular Unit Extraction
Clinical Dermatology: Research and Therapy CASE REPORT Management of Cicatricial Alopecia by Hair Transplantation using Follicular Unit Extraction Gillian Roga*, Jyoti Gupta, Amrendra Kumar and Kavish Chouhan Department of Dermatology, St. John’s medical college and hospital, India ARTICLE INFO ABSTRACT Hair transplantation by Follicular Unit Extraction (FUE) has been commonly used in androgenetic Received Date: August 23, 2017 alopecia but there is comparatively less experience with cicatricial alopecia. In this article we have Accepted Date: October 31, 2017 discussed and reviewed various factors influencing the modality of surgical treatment in cicatricial Published Date: November 09, 2017s alopecia. Although there have been many speculations about viability and results, we have noted successful results by FUE in a scar tissue. Cicatricial alopecia can be succesfully managed by hair transplantation provided certain requisites are satisfied.With adept surgical skill and insightfulness KEYWORDS we can restore good density coverage in even a compromised recipient area. Cicatricial alopecia; Hair transplant; INTRODUCTION Follicular unit extraction Cicatricial or scarring alopecia is an irreversible hair loss causing permanent damage of the stem cells in the hair follicle bulge appearing as shiny atrophic patches with effacement of follicular orifices [1]. Being only confined to the scalp, it may not harm a person physically but it definitely Copyright: © 2017 Roga G et al., Clin affects the self-image and self-esteem of the patient [2,3]. The best way to reach a confirmatory Dermatol Res Ther This is an open access diagnosis of cicatricial alopecia is by histopathological examination. Treatment usually requires a article distributed under the Creative combination of medical as well as surgical intervention which comprises of hair transplantation or Commons Attribution License, which surgical excision [4,5]. -

Alopecia Areata Part 1: Pathogenesis, Diagnosis, and Prognosis
Clinical Review Alopecia areata Part 1: pathogenesis, diagnosis, and prognosis Frank Spano MD CCFP Jeff C. Donovan MD PhD FRCPC Abstract Objective To provide family physicians with a background understanding of the epidemiology, pathogenesis, histology, and clinical approach to the diagnosis of alopecia areata (AA). Sources of information PubMed was searched for relevant articles regarding the pathogenesis, diagnosis, and prognosis of AA. Main message Alopecia areata is a form of autoimmune hair loss with a lifetime prevalence of approximately 2%. A personal or family history of concomitant autoimmune disorders, such as vitiligo or thyroid disease, might be noted in a small subset of patients. Diagnosis can often be made clinically, based on the characteristic nonscarring, circular areas of hair loss, with small “exclamation mark” hairs at the periphery in those with early stages of the condition. The diagnosis of more complex cases or unusual presentations can be facilitated by biopsy and histologic examination. The prognosis varies widely, and poor outcomes are associated with an early age of onset, extensive loss, the ophiasis variant, nail changes, a family history, or comorbid autoimmune disorders. Conclusion Alopecia areata is an autoimmune form of hair loss seen regularly in primary care. Family physicians are well placed to identify AA, characterize the severity of disease, and form an appropriate differential diagnosis. Further, they are able educate their patients about the clinical course of AA, as well as the overall prognosis, depending on the patient subtype. Case A 25-year-old man was getting his regular haircut when his EDITor’s KEY POINTS • Alopecia areata is an autoimmune form of barber pointed out several areas of hair loss. -

Hypertrichosis in Alopecia Universalis and Complex Regional Pain Syndrome
NEUROIMAGES Hypertrichosis in alopecia universalis and complex regional pain syndrome Figure 1 Alopecia universalis in a 46-year- Figure 2 Hypertrichosis of the fifth digit of the old woman with complex regional complex regional pain syndrome– pain syndrome I affected hand This 46-year-old woman developed complex regional pain syndrome (CRPS) I in the right hand after distor- tion of the wrist. Ten years before, the diagnosis of alopecia areata was made with subsequent complete loss of scalp and body hair (alopecia universalis; figure 1). Apart from sensory, motor, and autonomic changes, most strikingly, hypertrichosis of the fifth digit was detectable on the right hand (figure 2). Hypertrichosis is common in CRPS.1 The underlying mechanisms are poorly understood and may involve increased neurogenic inflammation.2 This case nicely illustrates the powerful hair growth stimulus in CRPS. Florian T. Nickel, MD, Christian Maiho¨fner, MD, PhD, Erlangen, Germany Disclosure: The authors report no disclosures. Address correspondence and reprint requests to Dr. Florian T. Nickel, Department of Neurology, University of Erlangen-Nuremberg, Schwabachanlage 6, 91054 Erlangen, Germany; [email protected] 1. Birklein F, Riedl B, Sieweke N, Weber M, Neundorfer B. Neurological findings in complex regional pain syndromes: analysis of 145 cases. Acta Neurol Scand 2000;101:262–269. 2. Birklein F, Schmelz M, Schifter S, Weber M. The important role of neuropeptides in complex regional pain syndrome. Neurology 2001;57:2179–2184. Copyright © 2010 by -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous,