Erythematous Plaque on the Scalp with Alopecia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Infectious Eccrine Hidradenitis Associated with Intense Sun Exposure
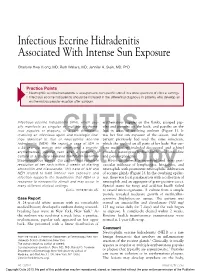
Infectious Eccrine Hidradenitis Associated With Intense Sun Exposure Charlotte Hwa Vuong, MD; Ruth Walters, MD; Jennifer A. Stein, MD, PhD Practice Points Neutrophilic eccrine hidradenitis is a response to nonspecific stimuli in a wide spectrum of clinical settings. Infectious eccrine hidradenitis should be included in the differential diagnosis in patients who develop an erythematous papular eruption after sunburn. Infectious eccrine hidradenitis (IEH), which usu- erythematous papules on the flanks, grouped pap- ally manifests as singular or multiple erythema- ules and pustules on the back, and papules on the tous papules or plaques, is a rare dermatosis legs in areas of resolving sunburn (Figure 1). It involving an infectious agent and histologic find- was her first sun exposure of the season, and the ings identical to that of CUTISneutrophilic eccrine patient previously had used the same sunscreen, hidradenitis (NEH). We report a case of IEH in which she applied on all parts of her body. Her cur- a 24-year-old woman who developed a pruritic, rent medications included desogestrel and ethinyl erythematous, papular rash after a sunburn. A estradiol, naratriptan hydrochloride, and loratadine culture of a pustule revealed methicillin-sensitive and pseudoephedrine. Staphylococcus aureus. Our patient had complete Histology showed a superficial and deep peri- resolution of her rash within 2 weeks of starting vascular infiltrate of lymphocytes, histiocytes, and amoxicillinDo and clavulanate. ThisNot case of IEH and neutrophils Copy with prominent neutrophilic infiltration NEH related to both intense sun exposure and of eccrine glands (Figure 2). In the overlying epider- infection supports the hypothesis that NEH is a mis, there was focal parakeratosis with a collection of response to nonspecific stimuli and may occur in neutrophils and an aggregate of gram-positive cocci. -

Hypertrichosis Terminalis
97297 Med Genet 1996;33:972-974 An autosomal dominant syndrome of acromegaloid facial appearance and generalised J Med Genet: first published as 10.1136/jmg.33.11.972 on 1 November 1996. Downloaded from Department of hypertrichosis terminalis Medical Genetics, Belfast City Hospital, Lisburn Road, Belfast BT9 7AB, Northern Ireland Alan D Irvine, Olivia M Dolan, David R Hadden, Fiona J Stewart, E Ann Bingham, A D Irvine Norman C Nevin F J Stewart N C Nevin Department of Dermatology, Royal Abstract A family with four affected subjects in three Group of Hospitals, Belfast BT12 6BA, We report a family in which a phenotype generations is reported. Affected subjects show Northern Ireland of acromegaloid facial appearance (AFA) a characteristic acromegaloid facial appearance 0 M Dolan and generalised hypertrichosis terminalis (AFA) and generalised hypertrichosis ter- E A Bingham segregates through three generations. minalis. The syndrome is inherited as an auto- Sir George E Clark Congenital hypertrichosis terminalis and somal dominant trait and appears to be fully Metabolic Unit, Royal AFA have been previously reported as in- penetrant. Acromegaloid facial appearance and Group of Hospitals, dependent autosomal dominant traits. hypertrichosis terminalis have been described Belfast BT12 6BA, Northern Ireland This is the first report to delineate an auto- in association with thickened oral mucosa and D R Hadden somal dominant transmission of the com- gingival hyperplasia.'"2 Affected patients in our Correspondence to: bined phenotype. family did not have intraoral lesions. The Dr Irvine. (JtMed Genet 1996;33:972-974) syndrome in our family appears to be discrete Received 14 May 1996 from the acromegaloid facial appearance syn- Revised version accepted for Key words: terminal hypertrichosis; acromegaloid drome,3 Gorlin-Chaudhry-Moss syndrome,4 publication 28 June 1996 facies; autosomal dominant. -

Endocrinology 12 Michel Faure, Evelyne Drapier-Faure
Chapter 12 Endocrinology 12 Michel Faure, Evelyne Drapier-Faure Key points 12.1 Introduction Q HS does not generally appear to be In 1986 Mortimer et al. [14] reported that hi- associated with signs of hyperan- dradenitis suppurativa (HS) responded to treat- drogenism ment with the potent antiandrogen cyproterone acetate. They suggested that the disease could Q Sex hormones may affect the course of be androgen-dependent [8]. This hypothesis HS indirectly through, for example, was also upheld by occasional reports of women their effects on inflammation with HS under antiandrogen therapy [18]. Actu- ally, the androgen dependence of HS (similarly Q The role of end-organ sensitivity to acne) is only poorly substantiated. cannot be excluded at the time of writing 12.2 Hyperandrogenism and the Skin Q The prevalence of polycystic ovary syndrome in HS has not been system- Androgen-dependent disorders encompass a atically investigated broad spectrum of overlapping entities that may be related in women to the clinical consequenc- es of the effects of androgens on target tissues and of associated endocrine and metabolic dys- functions, when present. #ONTENTS 12.1 Introduction ...........................95 12.2.1 Androgenization 12.2 Hyperandrogenism and the Skin .........95 12.2.1 Androgenization .......................95 One of the less sex-specific effects of androgens 12.2.2 Androgen Metabolism ..................96 12.2.3 Causes of Hyperandrogenism ...........96 is that on the skin and its appendages, and in particular their action on the pilosebaceous 12.3 Lack of Association between HS unit. Hirsutism is the major symptom of hyper- and Endocrinopathies ..................97 androgenism in women. -

Back to Basics: Understanding Hidradenitis Suppurativa
PRACTICE DEVELOPMENT Back to basics: understanding hidradenitis suppurativa KEY WORDS Hidradenitis Suppurativa (HS) is a chronic recurrent debilitating skin disease of the Dermatology hair follicle. It is a condition that has been overlooked in wound care publications, Fistulae with most articles found in dermatological journals. However, the condition affects Hidradenitis Suppurativa 1% of the population in Europe and produces painful nodules in one or more of Scarring Sinus tracts the apocrine-gland bearing aspects of the skin that can ulcerate and produce pain and a foul odour and can multiply and eventually develop sinus tracts and fistulae. HS is often misdiagnosed as alternative skin ulcerating conditions, leaving the individuals with many years of suffering from the physical symptoms and their psychological consequences. The disease often begins in puberty and burns out by middle age, leaving the individual with unsightly scarring. This article examines the pathophysiology, clinical presentations and comorbidities associated with the disease. The treatment options focus on controlling the comorbidities, moderating life-style behaviours and arresting the disease. The medical and surgical options are discussed along with their limitations. idrarenitis Suppurativa (HS) was first selection bias, however is thought to be 1% in described by the French surgeon Velpeau Europe (Gulliver et al, 2016; WUWHS, 2016). in 1839. The origin of the term HS comes Prevalence is rare in children and when HS does Hfrom the Greek hidros meaning sweat and aden occur in this population it is often associated with denoting glands (Ather et al, 2006). Initially it was hormonal disorders such as metabolic syndrome, thought to be due to infection of the sweat glands precocious puberty, adrenal hyperplasia and however it is now recognized as an acneform premature adrenarche (Vivar and Kruse, 2017). -

Digital Clubbing
Review Article Digital clubbing Malay Sarkar, D. M. Mahesh1, Irappa Madabhavi2 Department of Pulmonary Medicine, Indira Gandhi Medical College, Shimla, 1Department of Endocrinology, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, 2Post Graduate Student (Medicine), Indira Gandhi Medical College, Shimla, India ABSTRACT Digital clubbing is an ancient and important clinical signs in medicine. Although clubbed fingers are mostly asymptomatic, it often predicts the presence of some dreaded underlying diseases. Its exact pathogenesis is not known, but platelet‑derived growth factor and vascular endothelial growth factor are recently incriminated in its causation. The association of digital clubbing with various disease processes and its clinical implications are discussed in this review. KEY WORDS: Cancer, digital clubbing, hypertrophic osteoarthropathy, megakaryocytes, vascular endothelial growth factor Address for correspondence: Dr. Malay Sarkar, Department of Pulmonary Medicine, Indira Gandhi Medical College, Shimla ‑ 171 001, India. E‑mail: [email protected] INTRODUCTION long bones and occasional painful joint enlargement. It was initially known as hypertrophic pulmonary Digital clubbing is characterized by a focal bulbous osteoarthropathy (HPOA) based on the fact that majority enlargement of the terminal segments of the fingers of cases of HOA are due to malignant thoracic tumors. and/or toes due to proliferation of connective tissue The term “pulmonary” was later abandoned as it was between nail matrix and the distal phalanx. It results in realized that the skeletal syndrome may occur in several increase in both anteroposterior and lateral diameter of non‑pulmonary diseases and even may occur without the nails.[1] Clubbed fingers are also known as watch‑glass any underlying illness. -

Metformin for the Treatment of Hidradenitis Suppurativa: a Little Help Along the Way
DOI: 10.1111/j.1468-3083.2012.04668.x JEADV ORIGINAL ARTICLE Metformin for the treatment of hidradenitis suppurativa: a little help along the way R. Verdolini,† N. Clayton,‡,* A. Smith,‡ N. Alwash,† B. Mannello§ †Department of Dermatology, Princess Alexandra Hospital NHS trust, Harlow, Essex, and ‡Department of Dermatology, The Royal London Hospital, London, UK §Mannello Statistics, Via Rodi, Ancona, Italy *Correspondence: N. Clayton. E-mail: [email protected]; [email protected] Abstract Background Despite recent insights into its aetiology, hidradenitis suppurativa (HS) remains an intractable and debilitating condition for its sufferers, affecting an estimated 2% of the population. It is characterized by chronic, relapsing abscesses, with accompanying fistula formation within the apocrine glandbearing skin, such as the axillae, ano-genital areas and breasts. Standard treatments remain ineffectual and the disease often runs a chronic relapsing course associated with significant psychosocial trauma for its sufferers. Objective To evaluate the clinical efficacy of Metformin in treating cases of HS which have not responded to standard therapies. Methods Twenty-five patients were treated with Metformin over a period of 24 weeks. Clinical severity of the disease was assessed at time 0, then after 12 weeks and finally after 24 weeks. Results were evaluated using Sartorius and DLQI scores. Results Eighteen patients clinically improved with a significant average reduction in their Sartorius score of 12.7 and number of monthly work days lost reduced from 1.5 to 0.4. Dermatology life quality index (DLQI) also showed a significant improvement in 16 cases, with a drop in DLQI score of 7.6. -

Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review
toxins Review Therapeutic Use of Botulinum Neurotoxins in Dermatology: Systematic Review Emanuela Martina †, Federico Diotallevi †, Giulia Radi †, Anna Campanati * and Annamaria Offidani Dermatological Clinic, Department of Clinical and Molecular Sciences, Polytechnic Marche University, 60020 Ancona, Italy; [email protected] (E.M.); [email protected] (F.D.); [email protected] (G.R.); annamaria.offi[email protected] (A.O.) * Correspondence: [email protected] † These authors equally contributed to the manuscript. Abstract: Botulinum toxin is a superfamily of neurotoxins produced by the bacterium Clostridium Botulinum with well-established efficacy and safety profile in focal idiopathic hyperhidrosis. Recently, botulinum toxins have also been used in many other skin diseases, in off label regimen. The objective of this manuscript is to review and analyze the main therapeutic applications of botulinum toxins in skin diseases. A systematic review of the published data was conducted, following Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. Botulinum toxins present several label and off-label indications of interest for dermatologists. The best-reported evidence concerns focal idiopathic hyperhidrosis, Raynaud phenomenon, suppurative hidradenitis, Hailey–Hailey disease, epidermolysis bullosa simplex Weber–Cockayne type, Darier’s disease, pachyonychia congenita, aquagenic keratoderma, alopecia, psoriasis, notalgia paresthetica, facial erythema and flushing, and oily skin. -

Hidradenitis Suppurativa FOUR CORNERS of CARE
THE www.thedermdigest.com Vol. 2, No. 3 | March 2021 Hidradenitis Suppurativa FOUR CORNERS OF CARE Topical CBD: Hope or Hype? The Dermatologist as PCP Ask the Experts Permit No. 129 No. Permit Your Most High-Impact Columbus, WI Columbus, PAID Cosmetic Innovations US Postage US Prsrt Mkt Prsrt EDUCATIONAL • INTERACTIVE • AUTHORITATIVE Say Hello again to Not Actual Size Most eligible commercially $ per prescription insured patients pay as little as 20at any pharmacy* * Certain restrictions apply. The LEO Pharma CONNECT program may reduce out-of-pocket expenses. Must be 12 years of age or older to be eligible, and a legal guardian over 18 years of age must redeem the card for patients aged 12 to 17. You are not eligible if you are enrolled or you participate in any state or federally funded health care program (eg, Medicare, Medicaid, etc). Full details of the LEO Pharma CONNECT program are available at www.FinaceaFoam.com/hcp or may be obtained by calling 1-877-678-7494 between 8:30 AM and 8:30 PM (Eastern), Monday through Friday. The LEO Pharma logo, LEO Pharma, and Finacea are registered trademarks of LEO Pharma A/S. www.FinaceaFoam.com ©2020 LEO Pharma Inc. All rights reserved. March 2020 MAT-32481 THE Contents www.thedermdigest.com Volume 2, Number 3 | March 2021 14 Cover Article You can help hidradenitis suppurativa patients achieve long-term control and avoid flares 2 20 Ted Talks Pediatrics Do you talk politics in your office? Combination therapy can produce good clearance of pediatric warts 6 Literature Lessons Research updates in rheumatologic diseases, psoriasis, hair and nails, contact dermatitis, acne, rosacea, and more continued on page 3 March 2021 | 1 Ted Talks “ In politics, stupidity is not a handicap.” —Attributed to Napoleon Bonaparte he year was 1960, in the middle of a highly conten- T tious presidential contest between John F. -

Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) • Definition: O Inflammation Of
Folliculitis Highlights Author: Indira Gowda (EM Resident Physician, Mount Sinai Hospital) Definition: o Inflammation of the hair follicle caused by either chemical/physical irritation or viral/bacterial infection o Folliculitis is the smallest and most minor o Furuncles are larger, carbuncles larger than that, and boils even larger (3) Taken From: http://www.shorthillsderm .com/blog/wp- Common associations: content/uploads/2014/11/ o Diabetes, immunosuppression, shaving What-is-Folliculitis.jpg Diagnosis: o Based on appearance and history o Usually seen on scalp, face, legs, back, chest, axilla o Folliculitis is usually not tender compared to carbuncles and furuncles o If someone has had recent contact w/ hot tub or DM, consider pseudomonas as potential bacteria (3) o May see hyper- or hypopigmentation post infection Tx: o Warm compresses 3 times/day o Antibiotics as treatment of recurrent infections is controversial as increased antibiotic use may lead to increased resistance . Topical mupirocin for moderate folliculitis, more severe infections may require antibiotics . For tx of strep: dicloxacillin or cefadroxil; tx of strep infections helps to prevent PSGN but no effect on rheumatic fever (3) . For tx of pseudomonas: fluoroquinolones or carbapenems or other anti-pseudomonal options . For tx staph (particularly MRSA): 7-10 day course of Bactrim, clindamycin, doxycycline, vancomycin, linezolid,… other antibiotics reserved for more severe infections. (5) o Many people carry MRSA in their nares. Between 10-35% are persistent carriers and 20-75% intermittent carriers. (4) . Should we treat carriers? (Mashhood AA, 2006) recommends nasal Taken from http://riversideonline.com swab testing in all patients with recurrent “furunculosis” aka boils /source/images/image_po aka abscesses. -

Pachydermoperiostosis in a Patient with Crohn's Disease: Treatment
IJMS Vol 43, No 1, January 2018 Case Report Pachydermoperiostosis in a Patient with Crohn’s Disease: Treatment and Literature Review Maryam Mobini1, MD; Abstract Ozra Akha1, MD; Hafez Fakheri2, MD; Pachydermoperiostosis (PDP) is a rare disorder characterized Hadi Majidi3, MD; by pachydermia, digital clubbing, periostitis, and an excess Sanam Fattahi4, MD of affected males. It is the primary form of hypertrophic osteoarthropathy (HOA) and there are some rare associations of PDP with other disorders. Here we describe a patient with 1Department of Internal Medicine, Diabetes Research Center, Faculty of Crohn’s disease associated with PDP. A 26-year-old man, who Medicine, Mazandaran University of was a known case of Crohn’s disease, referred with diffuse Medical Sciences, Sari, Iran; 2Department of Gastroenterology, swelling in the upper and lower limbs and cutis verticis gyrata Inflammatory Gut and Liver Research since 7 years ago. PDP was suspected and endocrinological Center, Mazandaran University of and radiological studies were conducted for the evaluation Medical Sciences, Sari, Iran; 3Department of Radiology, Orthopedic of underlying disease. He was prescribed celecoxib, low- Research Center, Faculty of Medicine, dose prednisolone, and pamidronate to control the swelling, Mazandaran University of Medical periostitis, azathiopurine, and mesalazine according to Sciences, Sari, Iran; 4Medical Student, Faculty of Medicine, gastrointestinal involvement. In conclusion, it is important to Mazandaran University of Medical identify this condition since a misdiagnosis might subject the Sciences, Sari, Iran patient to unnecessary investigations. Correspondence: Maryam Mobini, MD; Please cite this article as: Mobini M, Akha O, Fakheri H, Majidi H, Fattahi S. Imam Khomeini Hospital, Pachydermoperiostosis in a Patient with Crohn’s Disease: Treatment and Razi Street, Sari, Iran Literature Review. -

Understanding Hidradenitis Suppurativa (Hs)
UNDERSTANDING HIDRADENITIS SUPPURATIVA (HS) Information to help you work with your doctor so you can better manage your HS WHAT’S INSIDE Hidradenitis suppurativa (HS) in brief . 4 HS – the facts . 5 Living with HS . 9 Coping with HS . 11 Tips and tricks for living with HS . 12 Addressing your thoughts and feelings . 14 Coping with stress . 16 Working with your health care team . 17 Symptom self-assessment questionnaire . 19 Useful online resources . 23 3 HIDRADENITIS SUPPURATIVA (HS) IN BRIEF You have been diagnosed with HS, a disease which is: PAINFUL PRORESSIVE INFLAMMATORY GETTING WORSE CAUSING OVER TIME SWELLING CHRONIC SYSTEMIC LASTING AFFECTING A LONG TIME THE WHOLE BODY HS is known to produce lesions in the skin that are inflamed (swollen), recurrent (reappearing after lesions disappear), and chronic (lasting a long period of time). HS can have both a physical and psychological impact. The resulting pain and affected areas of your skin can restrict movement and your ability to do day-to-day tasks. Because of the areas of the body affected and how unsightly, smelly, and uncomfortable or painful HS may be, it can also lead to negative feelings such as embarrassment, stress and low mood. While we understand this is how some people with HS may feel, it’s important to remember that HS is a medical condition — its development is not your fault. 4 It’s important to be able to manage the physical side of the condition while also trying to reduce any feelings of embarrassment you may feel. There is more information about addressing your thoughts and feelings on page 14. -

Pachydermoperiostosis (Touraine–Solente–Gole Syndrome): a Case
Joshi et al. Journal of Medical Case Reports (2019) 13:39 https://doi.org/10.1186/s13256-018-1961-z CASE REPORT Open Access Pachydermoperiostosis (Touraine–Solente– Gole syndrome): a case report Amir Joshi1* , Gaurav Nepal1, Yow Ka Shing2, Hari Prasad Panthi1 and Suman Baral1 Abstract Background: Pachydermoperiostosis (PDP) is a rare disorder characterized by clubbing of the fingers, thickening of the skin (pachyderma), and excessive sweating (hyperhidrosis). It typically appears during childhood or adolescence, often around the time of puberty, and progresses slowly. Clinical presentations of PDP can be confused with secondary hypertrophic osteoarthropathy, psoriatic arthritis, rheumatoid arthritis, thyroid acropachy, and acromegaly. Case presentation: A Mongolian male, aged 19 years, resident of a hilly district of Nepal, with history of consanguinity, presented to our outpatient department with chief complaints of pain and swelling in both hands and feet for 6 years. The pain was insidious in onset, throbbing in nature, and not relieved by over-the-counter medications. The patient also complained of profuse sweating, progressive enlargement of hands and feet, and gradual coarsening of facial features. On examination there were marked skin folds in the forehead, face, and eyelids. Clubbing and swelling of bilateral knee joints and ankle joints was also evident. He was subsequently investigated extensively for acromegaly. Insulin-like growth factor-1 level and oral glucose tolerance test were normal. Radiography of various bones showed