Methodology for Cultural Adaptation of National CAN-MDS Toolkits Target Group Partners and Any Stakeholder Interested in Developing a CAN-MDS
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Strategia De Dezvoltare Economică Şi Socială a Judeţului Suceava, Perioada 2011 – 2020
UNIUNEA EUROPEANĂ GUVERNUL ROMÂNIEI Inovaţie în administraţie Fondul Social European Ministerul Administraţiei şi Programul Operaţional Internelor "Dezvoltarea Capacităţii Administrative” STRATEGIA DE DEZVOLTARE ECONOMICĂ ŞI SOCIALĂ A JUDEŢULUI SUCEAVA, PERIOADA 2011 – 2020 Proiect cofinanțat din Fondul Social European, prin Programul Operațional “Dezvoltarea Capacității Administrative” 1 CUPRINS SECŢIUNEA A. CADRUL DE REFERINŢĂ – Evaluarea situaţiei existente din punct de vedere socio - economic, al mediului şi al nivelului de echipare tehnică şi socială în judeţul Suceava ................................................ 4 CAPITOLUL I. CADRUL NATURAL............................................................................................................................... 4 I.1. Aşezarea geografică. Frontiere ....................................................................................................................... 4 I.2. Suprafaţa ........................................................................................................................................................... 4 I.3. Populaţia ........................................................................................................................................................... 4 I.4. Unităţile administrativ-teritoriale .................................................................................................................. 4 I.5. Reţeaua hidrografică ...................................................................................................................................... -
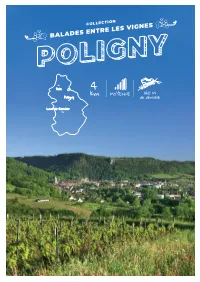
Balades Entre Les Vignes
COLLECTION BALADES ENTRE LES VIGNES Dole 4 MOYENNE 140 M Poligny km de dénivelé Lons-le-Saunier POUR ALLER DE POLIGNY, ON RETIENT SOUVENT QU’ELLE EST LA CAPITALE MONDIALE LE PLUS LOIN… DU COMTÉ. MAIS CETTE CITÉ DE CARACTÈRE EST AUSSI L’HÉRITIÈRE UNE ŒUVRE D’UNE RICHE HISTOIRE ET D’UNE TRADITION VITICOLE AFFIRMÉE. PARCOURS 1 DE DÉCOUVERTE À L’EMBOUCHURE DE LA “RECULÉE” DE POLIGNY, CETTE BALADE VOUS EMMÈNE À LA DÉCOUVERTE DE VESTIGES ET DE VIGNES SECRÈTES • Départ sur le parking jouxtant l’ONF, OÙ DE SUBLIMES PANORAMAS S’OFFRIRONT À VOUS. CÔTÉ VILLE, en haut de la rue de la Doye. VOUS AUREZ L’OCCASION DE DÉCOUVRIR L’HABITAT TRADITIONNEL Pour cette promenade le balisage est jaune puis blanc et rouge (GR 59) puis à La statue du Vigneron est une belle VIGNERON (QUARTIER DE CHARCIGNY). sculpture de bronze dédiée à Wladimir nouveau jaune. Gagneur, célèbre militant et député • En partant de l’ONF, descendez la fouriériste qui se situe Square de Charcigny. Elle valorise les valeurs progressistes du XIXe rue de la Doye puis la rue de Faîte en siècle : l’épanouissement par l’étude (le livre) direction du village, jusqu’au poteau et le travail (le bigot). Un chef d’œuvre signé Marguerite Syamour inauguré en 1889. “Charcigny”. Laissez sur la gauche, la tour de la Sergenterie, les vestiges du château de Grimont au pied duquel coule le UN BELVÉDÈRE Sergenterin. Vous êtes dans le typique 2 quartier vigneron de Charcigny dont les GORGES DE GREUBEY caves affleurent par des trappes sur la rue ; • Au poteau “Charcigny”, prenez la direc- tion “Gorges de Greubey”. -

Harmonizing State- and EU-Funded Projects in Regions | Final Synthesis Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Public Disclosure Authorized Harmonizing STATE- AND EU-FUNDED PROJECTS in Regions | Final Synthesis Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Agreement for Harmonizing State- and EU-funded Final Investment Programs Romania Regional Development Program 2 Synthesis Dated November 26, 2015 Project co-financed from the European Regional Development Fund through the Operational Programme Technical Assistance (OPTA) 2007-2013 Agreement for Advisory Services on Assistance to the Romanian Ministry of Regional Development and Public Administration on Harmonizing State- and EU- funded Projects in Regions Final Synthesis November 26, 2015 Romania Regional Development Program 2 4 Table of Contents Table of Contents ....................................................................................................................................... i List of Figures ............................................................................................................................................ iii List of Tables ............................................................................................................................................. iv List of Boxes .............................................................................................................................................. iv List of Acronyms ........................................................................................................................................ v Sumary ........................................................................................................................................................ -

Monografia Judeţului Iaşi
MONOGRAFIA JUDEŢULUI SUCEAVA Cuprins 1. Locul judeţului Suceava în economia naţională ............................................... 2. Prezentarea generală a judeţului....................................................................... Indicatori sintetici ai activităţii economice .................................................... 12 4. Agenţi economici ........................................................................................... 1 5. Unităţi locale active ....................................................................................... 1 6. Unităţi locale active din industrie, construcţii, comerţ şi alte servicii………15 7. Agricultura şi silvicultura ............................................................................... 17 8. Transporturi .................................................................................................... 2 9. Comerţ exterior .............................................................................................. 21 1 . Forţa de muncă şi veniturile salariale ........................................................... 2 11. Activitatea bancară ....................................................................................... 26 12. Investiţii străine ............................................................................................ 2 Bibliografie ........................................................................................................ 1. Locul judeţului Suceava în economia naţională Indicatori 1 11 Suprafaţa totală (ha) 2 2 2 2 Numărul -

Strategia Integrată De Dezvoltare Urbană a Municipiului Giurgiu 2014-2020
STRATEGIA INTEGRATĂ DE DEZVOLTARE URBANĂ A MUNICIPIULUI GIURGIU 2014-2020 1 ABREVIERI FEDR Fondul European pentru Dezvoltare Regională FSE Fondul European Social IMM Întreprinderi Mici şi Mijlocii INS Institutul Naţional pentru Statistică ONG Organizaţii Neguvernamentale PIB Produs Intern Brut PO Programul Operaţional POR Programul Operaţional Regional PO CU Programul Operaţional Capital Uman POIM Programul Operațional Infrastructură Mare AFM Administrația Fondului pentru Mediu PUG Planul Urbanistic General PUZ Plan Urbanistic Zonal PUD Plan de Urbanism de Detaliu SF Studiu de Fezabilitate PT și DDE Proiect Tehnic și Detalii de Execuție PIDU Plan intregrat de dezvoltare urbană PMUD Plan de Mobilitate Urbană Durabilă ZUM Zonă Urbană Marginalizată 2 CUPRINS CAPITOLUL I. Contextul urban și identificarea principalelor probleme și provocări la nivel local ............................... 4 Subcapitolul 1 – Definirea situației existente ............................................................................................................... 4 1.1 Municipiul Giurgiu - aşezare, populaţie, suprafaţă ..................................................................... 4 1.2 Unităţi administrativ-teritoriale ................................................................................................. 10 1.3 Cadrul natural ........................................................................................................................... 11 1.2 Economia ................................................................................................................................... -

13: 978-1-60244-079-1 Isbn-10: 1-60244-079-4
Evaluation of the World Bank’s Assistance to Basic Education in Romania A Country Case Study Sue E. Berryman Amber Gove Dana Sapatoru Anca Tirca Director-General, Independent Evaluation: Vinod Thomas Director, Independent Evaluation Group, World Bank: Ajay Chhibber Manager: Alain Barbu Task Manager: H. Dean Nielsen 2007 The World Bank This paper is available upon request from IEG. Washington, D.C. ENHANCING DEVELOPMENT EFFECTIVENESS THROUGH EXCELLENCE AND INDEPENDENCE IN EVALUATION The Independent Evaluation Group is an independent unit within the World Bank Group; it reports directly to the Bank’s Board of Executive Directors. IEG assesses what works, and what does not; how a borrower plans to run and maintain a project; and the lasting contribution of the Bank to a country’s overall development. The goals of evaluation are to learn from experience, to provide an objective basis for assessing the results of the Bank’s work, and to provide accountability in the achievement of its objectives. It also improves Bank work by identifying and disseminating the lessons learned from experience and by framing recommendations drawn from evaluation findings. IEG Working Papers are an informal series to disseminate the findings of work in progress and to encourage the exchange of ideas about development effectiveness through evaluation. The findings, interpretations, and conclusions expressed here are those of the author(s) and do not necessarily reflect the views of the Board of Executive Directors of the World Bank or the governments they represent. The World Bank cannot guarantee the accuracy of the data included in this work. The boundaries, colors, denominations, and other information shown on any map in this work do not imply on the part of the World Bank any judgment of the legal status of any territory or the endorsement or acceptance of such boundaries. -

Funcţiile Terţiare Ale Municipiului Cluj-Napoca
UNIVERSITATEA BABEŞ-BOLYAI CLUJ-NAPOCA FACULTATEA DE GEOGRAFIE CATEDRA DE GEOGRAFIE UMANĂ TEZĂ DE DOCTORAT Rezumat FUNCŢIILE TERŢIARE ALE MUNICIPIULUI CLUJ-NAPOCA COORDONATOR ŞTIINŢIFIC: Prof. univ. dr. SURD VASILE DOCTORAND: PĂCURAR BOGDAN-NICOLAE CLUJ-NAPOCA 2011 CUPRINS 1. Memoriu epistemologic..............................................................................................................6 2. Etapele abordării geografiei urbane în ştiinţa geografică.....................................................10 2.1. Abordările geografiei internaţionale în ştiinţa geografiei urbane..................................10 2.2. Abordările geografiei româneşti în ştiinţa geografiei urbane........................................16 2.3. Geografia urbană în şcoala geografică clujeană.............................................................18 3. Funcţiile aşezărilor. Clasificare şi fundamentare epistemologică........................................21 3.1. Consideraţii funcţionaliste asupra conceptelor şi termenilor definitorii în structurarea concepţiei asupra funcţiilor aşezărilor..................................................................................21 3.2. Funcţiile aşezărilor. Clasificare şi fundamentare epistemologică..................................27 3.2.1. Funcţiile aşezărilor rurale................................................................................27 3.2.2. Funcţiile aşezărilor urbane...............................................................................31 4. Funcţiile terţiare ale municipiului -
ISO 3166-2 NEWSLETTER Changes in the List of Subdivision Names And
ISO 3166-2 NEWSLETTER Date issued: 2010-02-03 No II-1 Corrected and reissued 2010-02-19 Changes in the list of subdivision names and code elements The ISO 3166 Maintenance Agency1) has agreed to effect changes to the header information, the list of subdivision names or the code elements of various countries listed in ISO 3166-2:2007 Codes for the representation of names of countries and their subdivisions — Part 2: Country subdivision code. The changes are based on information obtained from either national sources of the countries concerned or on information gathered by the Panel of Experts for the Maintenance of ISO 3166-2. ISO 3166-2 Newsletters are issued by the secretariat of the ISO 3166/MA when changes in the code lists of ISO 3166-2 have been decided upon by the ISO 3166/MA. ISO 3166-2 Newsletters are identified by a two-component number, stating the currently valid edition of ISO 3166-2 in Roman numerals (e.g. "I") and a consecutive order number (in Latin numerals) starting with "1" for each new edition of ISO 3166-2. For all countries affected a complete new entry is given in this Newsletter. A new entry replaces an old one in its entirety. The changes take effect on the date of publication of this Newsletter. The modified entries are listed from page 4 onwards. For reasons of user-friendliness, changes have been marked in red (additions) or in blue (deletions). The table below gives a short overview of the changes made. This Newsletter was initially issued 2010-02-03 and the entry for Serbia was incomplete and this Newsletter was reissued 2010-02-19. -

BAUMES, CIRQUES ET RECULEES EN ARBOIS (Jura)
Club Alpin Français d’Ile de France Michel LOHIER (tel : 02 32 51 90 15 ou à défaut 06 12 62 14 53) BAUMES, CIRQUES ET RECULEES EN ARBOIS (Jura) code 08-RW 23 niveau : M 22 au 24 mars 2008 édition du 2 janvier 2008 Cette randonnée au pied du Jura pourrait s’intituler : du sel, du vin et de l’eau . En effet à Salins, les salaisons de Séquanie étaient déjà très réputées du temps des Romains. Le sel valait plus que l’or au 17 e siècle et était conservé dans des lieux puissamment gardés comme à Arc et Senans à une trentaine de kilomètres de Salins. La première AOC de France est constituée de 5 cépages : Savagnin, Chardonnay, Pinot noir, Trousseau et Poulsard, donnant ce goût si particulier au vin d’Arbois. C’est dans la région que Louis Pasteur mena ses recherches sur la fermentation. Enfin l’eau qui a dessiné à travers des bancs calcaires ou marneux ces vallées aux parois abruptes formant baumes, cirques et reculées. Sans plus attendre voici le programme : Vendredi 21 mars : Transport : voir plus loin la rubrique : Comment se rendre sur place ? Rendez - vous dans le hall de la gare de Mouchard à 22h à l’arrivée du train. Transfert routier pour Salins les Bains . Hébergement en hôtel. Samedi 22 mars : Visite des Salines puis à pied au départ de Salins, Fort Saint André (construit par Vauban), Croix de Prétin, premiers vignobles à Montigny les Arsures, Arbois, visite de cave. Hébergement en ½ pension en hôtel pour 2 nuits. 4h30 Montée : 300 m Descente : 354 m Dimanche 23 mars : Circuit du Cirque du Fer à Cheval : Arbois, Mesnay, la Roche du Feu, les Planches près Arbois, cascade des Tufs et source de la Cuisance, le chemin des Diligences, belvédère du Fer à Cheval, Arbois. -

Profil Municipiul Suceava
Partea I Profilul localit ăŃ ii Cuprins 1. PREZENTARE GENERAL Ă A LOCALIT Ăł II ........................................................................... 1 1.1. POZI łIE GEOGRAFIC Ă ŞI LIMITE ................................................................................................ 1 1.2. ATESTARE DOCUMENTAR Ă ŞI SCURT ISTORIC ........................................................................... 2 1.3. OBIECTIVE TURISTICE ............................................................................................................. 4 1.4. OAMENI DE SEAM Ă ............................................................................................................... 12 2. CAPITAL NATURAL ................................................................................................................ 20 2.1. TIP CLIM Ă............................................................................................................................. 20 2.2. RELIEF ................................................................................................................................. 20 2.3. SOLURILE ............................................................................................................................ 21 2.4. VEGETA łIE .......................................................................................................................... 21 2.5. FAUNA ................................................................................................................................. 22 2.6. CALITATEA AERULUI -

Strategia Culturală a Municipiului T I M I Ș O A
GOVERNMENT OF ROMANIA SERBIAN GOVERNMENT STRATEGIA CULTURALĂ A MUNICIPIULUI TIMIȘOARA Investim în viitorul tău! Programul IPA de Cooperare Transfrontalieră România-Republica Serbia este finanţat de Uniunea Europeană prin Instrumentul 2014 - 2024 de Asistenţă pentru Preaderare (IPA) şi cofinanţat de statele partenere în program. Titlul proiectului: Politica culturală, instrument de dezvoltare comunitară şi regională Editorul materialului: Municipiul Timișoara Data publicării: noiembrie 2014 Conţinutul acestui material nu reprezintă în mod necesar poziţia oficială a Uniunii Europene. Pentru eventuale sesizări, contactaţi: [email protected] www.romania-serbia.net STRATEGIA CULTURALĂ A MUNICIPIULUI TIMIȘOARA 2014 - 2024 3 BENEFICIAR Primăria Municipiului Timişoara bd. C.D. Loga, nr. 1, cod poştal 300030 Timişoara, jud. Timiş T: +40 -(0)256408300, F.: +40 -(0)256490635 E: [email protected] I: www.primariatm.ro CONSORȚIU CONSULTANȚI Asociaţia MetruCub – resurse pentru cultură Calea Vitan nr. 201, bl.51, sc.1, et.8, ap.32, camera 2, cod poştal 031286, sector 3, Bucuresti T: +40 744399767 E: [email protected] I: www.m3culture.ro. A.T.U. – Asociaţia pentru Tranziţia Urbană str. Voila nr, 10, bl. 21, sc. 2, parler, ap. 16, camera 2, sector 4, Bucureşti T: +40 213126272 E: [email protected] I: www.atu.org.ro ECHIPA DE LUCRU Consorţiu contractat Coordonare: Vera Marin, Raluca Pop Planificare urbană şi planificare participativă: Vera Marin Politici culturale şi management cultural: Raluca Pop, Ioana Tamaş Arhitectură, patrimoniu, mediu -

Timisoara: Fragility Curves for Out-Of-Plane Local Mechanisms of Collapse
UNIVERSITÀ DEGLI STUDI DI PADOVA Dipartimento di Ingegneria Civile Edile e Ambientale Laurea Magistrale a Ciclo Unico in Ingegneria Edile – Architettura SEISMIC VULNERABILITY ASSESSMENT OF CLUSTERED BUILDINGS IN THE HISTORICAL CENTER OF TIMISOARA: FRAGILITY CURVES FOR OUT-OF-PLANE LOCAL MECHANISMS OF COLLAPSE RELATORE: Ch.ma Prof.ssa DA PORTO FRANCESCA CORRELATORI: Ch.mo Prof. CLAUDIO MODENA Ing. MARSON CLAUDIA Ing. MUNARI MARCO Ing. TAFFAREL SABRINA LAUREANDA: MARGHERITA ROVERATO ANNO ACCADEMICO 2014 / 2015 ACKNOWLEDGEMENTS I wish to express my sincere thanks to Prof. Francesca da Porto, supervisor of this thesis, and to Prof. Carlo Modena for the disposability shown and for the help provided in this thesis. My sincere thank you to Ing. Marco Munari, Ing. Claudia Marson and Ing. Sabrina Taffarel for the valuable guidance and the continuous encouragement as well as for the infinite patience. I am also grateful to the Polytechnic University of Timisoara for the help and the hospitality during the on-site activities and in particular I would like to thank Ing. Marius Mosoarca and Arch. Bogdan Demetrescu for the great disposability and the indispensable material provided. Thank you to my colleague and friend Claudia, with whom I spend the most part of my time and energy in the last months, to make enjoyable even the most difficult moments of this thesis. My heartfelt thanks to Elena, Giorgia and Linda, which join me and enjoy with me every day, and I mean literally every day, of these five years of University. My most beautiful academic memories are bond to you. I wish to express my deepest gratitude to my Family which has encouraged me and support me every day of my life, as well as tolerated me on my study periods.