Campylobacter Case-Control Study
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
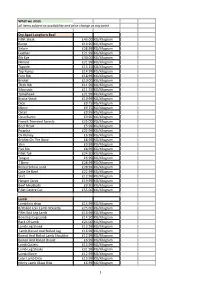
What We Stock All Items Subject to Availability and Price Change at Any Point
What we stock all items subject to availability and price change at any point Dry Aged Longhorn Beef Fillet Steak £45.00 KG/Kilogram Rump £19.95 KG/Kilogram Sirloin £28.99 KG/Kilogram Feather £21.99 KG/Kilogram Rib Eye £30.00 KG/Kilogram Minute £21.99 KG/Kilogram Topside £13.15 KG/Kilogram Top Rump £14.99 KG/Kilogram Fore Rib £18.99 KG/Kilogram Brisket £10.00 KG/Kilogram Thick Rib £11.99 KG/Kilogram Silverside £11.55 KG/Kilogram Tomahawk £21.99 KG/Kilogram Braise Steak £10.99 KG/Kilogram Dice £9.75 KG/Kilogram Mince £9.75 KG/Kilogram Oxtail £9.95 KG/Kilogram Osso Bucco £9.95 KG/Kilogram French Trimmed Forerib £25.00 KG/Kilogram Beef Heart £5.99 KG/Kilogram Picanha £22.99 KG/Kilogram Ox Kidney £6.99 KG/Kilogram Brisket On The Bone £8.99 KG/Kilogram Shin £9.99 KG/Kilogram Flat Rib £8.99 KG/Kilogram Fillet Tail £24.50 KG/Kilogram Tongue £6.99 KG/Kilogram T Bone £28.99 KG/Kilogram Rolled Sirloin Joint £28.99 KG/Kilogram Cote De Beof £22.99 KG/Kilogram Skirt £12.99 KG/Kilogram Hanger Steak £19.99 KG/Kilogram Beef Meatballs £9.50 KG/Kilogram Fillet Centre Cut £55.00 KG/Kilogram Lamb Lamb loin chop £14.99 KG/Kilogram B/Rolled Loin Lamb NoiseWe £25.00 KG/Kilogram Fillet End Leg Lamb £16.99 KG/Kilogram Boneless Leg Lamb £14.50 KG/Kilogram Rack Of Lamb £24.00 KG/Kilogram Lamb Leg Shank £13.99 KG/Kilogram Lamb Boned And Rolled Leg £16.99 KG/Kilogram Boned And Rolled Lamb Shoulder £12.99 KG/Kilogram Boned And Rolled Breast £6.99 KG/Kilogram Lamb Cutlets £13.99 KG/Kilogram Lamb Leg Steaks £21.99 KG/Kilogram Lamb Mince £12.99 KG/Kilogram Lean Lamb Dice -

International Benchmarking of the Small Goods Industry M.671
International benchmarking of the small goods industry M.671 Prepared by: Hassall & Associates Pty Ltd Published: December 1995 © 1998 This publication is published by Meat & Livestock Australia Limited ACN 081678364 (MLA). Where possible, care is taken to ensure the accuracy of information in the publication. Reproduction in whole or in part of this publication is prohibited without the prior written consent of MLA. Meat & Livestock Australia acknowledges the matching funds provided by the Australian Government and contributions from the Australian Meat Processor Corporation to support the research and development detailed in this publication. MEAT & LIVESTOCK AUSTRALIA -------------- EXECUTIVE SUMMARY 1. STUDY OBJECTIVES AND APPROACH 1.1 Why Benchmarking 1 1.2 Industry Benchmarking 1 1.3 Why Benchmark the Smallgoods Industry 4 1.4 Methodology 5 I. 5 Studies Related to the Smallgoods Industry 7 2. STRUCTURE OF THE AUSTRALIAN SMALLGOODS INDUSTRY 2.1 Overview of the Australian Smallgoods Industry 10 2.2 Smallgoods Industry Location and Composition II 2.3 Size ofEstablishment 11 2.4 Major Smallgoods Manufacturers 12 2.5 Smallgoods Industry Statistics 14 3. PERFORMANCE INDICATORS FOR SJX MAJOR AUSTRALIAN SMALLGOOD PRODUCERS 3.1 Coverage 29 3.2 Production 29 3.3 Meat and Other Materials Used 31 3.4 Labour 35 3.5 Labour Productivity 37 3.6 Unit Processing Costs 40 3.7 Labour Payments 40 3.8 Unit Material and Processing Costs 43 3.9 Human Resource Management Programs 43 4. SURVEY OF AUSTRALIAN INDUSTRY PERFORMANCE 4.1 Smallgoods Plant 46 4.2 -

Sales@Coldchoicefoods
www.coldchoicefoods.co.uk Coldchoicefoods Ltd [email protected] 0161 223 9157 Sliced Bacon Frozen Sausage Brecondale Sliced Back Bacon each 16s IQF Blakemans Supreme Saus each Sliced Catering Bacon 2kg each 32s IQF Blakemans Supreme Saus each Chefs Choice Sliced Back Bacon each 4s IQF Blakemans Supreme Sausa each Bacon Coldchoice Supertrim 2kg each 8s IQF Blakemans Supreme Sausa each Bacon Rib Free Coldchoice each IQF Value Sausage 8 each Smoked Sl Back Bacon 5lb each CCF Frozen Pork Sausage 8s each Smoked Sl Streaky Bacon 5lb each IQF Cooked Pork 8 each Smoked Prime Bacon 2.27kg each 8s IQF Cumberland Sausage each Stirchley Supertrim Bacon 2kg each IQF Country Park Sausage 8 each Sliced Streaky Bacon 5lb each Cumberland Ring 20x227g each Taylors Sl Back Bacon 2kg each Midland IQF Sausage 8s Case Prime Sliced Back Bacon 2kg each Orchard Farm Pork Sausage 8s each Dry Cure Sliced Back 2kg each Smoked Dry Cure Sliced Back 2k each Fresh Sausage Chipolata Pork & Beef each Fresh Pork Chipolata 6lb each BACON RETAIL PACK Chipolata Traditional Pork Fre each 8oz Gammon Steak PKT x5 each Cumberland Sausage Meat x454gr 300g Dry Cure Back Bacon each Fresh Thin Pork & Chille 6lb each 350g Prime Back Bacon each Fresh Thick Pork & Apple 6lb each 350g Prime Smoked Back Bacon each Fresh Thick Pork & Black Puddi each Fresh Thick Cumberland 6lb each Fresh Thick Pork & Chille 6lb each CURED PRODUCTS Fresh Thick Garlic Sausage 6lb each Shanks each Fresh Thick Lincolshire 6lb each Red Net Coverter Gammon kg Fresh Thick Old English 6lb each Danish -
Changing with the Times
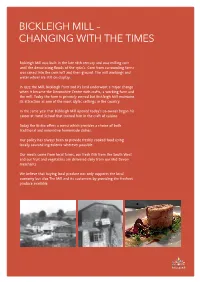
BICKLEIGH MILL – CHANGING WITH THE TIMES Bickleigh Mill was built in the late 18th century and was milling corn until the devastating floods of the 1960’s. Corn from surrounding farms was raised into the corn loft and then ground. The mill workings and water wheel are still on display. In 1973 the Mill, Bickleigh Farm and its land underwent a major change when it became the Devonshire Centre with crafts, a working farm and the mill. Today the farm is privately owned but Bickleigh Mill maintains its attraction as one of the most idyllic settings in the country. In the same year that Bickleigh Mill opened today’s co-owner began his career at Hotel School that trained him in the craft of cuisine. Today the Bistro offers a menu which provides a choice of both traditional and innovative homemade dishes. Our policy has always been to provide freshly cooked food using locally sourced ingredients wherever possible. Our meats come from local farms, our fresh fish from the South West and our fruit and vegetables are delivered daily from our Mid Devon merchants. We believe that buying local produce not only supports the local economy but also The Mill and its customers by providing the freshest produce available. BICKLEIGH BREAKFAST Served Monday to Saturday from 10am to 11.45am Full Bickleigh Breakfast £9.95 2 Rashers of Bacon, Devon Pork Sausage, Fried Egg, Black Pudding, Tomato, Mushrooms, Hash Browns and Baked Beans Vegetarian Full Bickleigh Breakfast £8.95 Vegetarian Sausage, Hash Browns, Beans, Tomato, Mushrooms, Fried Egg, Granary Toast Vegan -

Download Catalogue
(02) 4228 5626 [email protected] 17 Resolution Dr, Unanderra NSW 2526, Australia www.linmick.com.au Proud Distributors of the following Brands Villa POZZA www.linmick.com.au www.linmick.com.au Cold Meats Selection (Gluten Free) (Gluten Free) (Gluten Free) KR Rindless Short KR Rindless Middle KR Shaved Premium Cut Eye Bacon 5kg Rash Bacon 5kg Ham 1kg (Gluten Free) (Gluten Free) Melosi Double Castlemaine Shredded Castlemaine Sliced Smoked Ham Ham 2 x 2.5kg Pepperoni 4 x 1kg Melosi Large Melosi Small Melosi Mortadella Mortadella Mortadella Olives KR Sliced Mild & Hot Thin White Hungarian Calabrese 1kg Sliced Salami KR DON Cold Meats www.linmick.com.au Selection Mettwurst Salami Don Huttons Don Gyulai Devon Chub Don Diced Bacon KR Whole 6 x 2kg Cabanossi 3kg (Gluten Free) (Gluten Free) (Gluten Free) Zammit Rindless Middle Zammit Rind On Middle Zammit Short Cut Rash Bacon 5kg Rash Bacon 5kg Bacon 1kg (Gluten Free) (Gluten Free) (Gluten Free) Zammit Diced Bacon Zammit Short Cut Eye Zammit Praga Leg 3x3kg Bacon 15kg Ham www.linmick.com.au Cold Meats Selection (Gluten Free) (Gluten Free) (Gluten Free) Zammit Zammit Leg Ham Zammit Soccerball Lite Leg Ham Bone Out Ham (Gluten Free) (Gluten Free) (Gluten Free) Zammit Double Zammit Ham Zammit Diced smoked Ham Delux Ham (Gluten Free) (Gluten Free) (Gluten Free) Zammit Sandwich Zammit Fine Zammit Sliced Ham Shredded Ham Peperoni (Gluten Free) (Gluten Free) (Gluten Free) Zammit Flat Zammit Hot Zammit Danish Sopressa Hot & Mild Spanish Salami salami Cold Meats www.linmick.com.au Selection (Gluten Free) -

Food Preferences of Inpatients in an Australian Teaching Hospital—What Has Happened in the Last 12 Years?
Food preferences of inpatients in an Australian teaching hospital—what has happened in the last 12 years? Suzanne Kennewell and Maria Kokkinakos Abstract The aim of this study was to survey the food prefer- Methods ences of patients in a large teaching hospital in Australia and to compare the results to a similar study conducted in 1986. Possi- The survey instrument ble differences between genders also were examined. Five hundred and twenty-four patients completed a food preferences A slightly modified version of the questionnaire used by survey, using a nine-point hedonic scale, to indicate how much Williams was used to gather information on the food pref- they liked or disliked 223 different food items. Fresh fruit, poul- erences of hospital inpatients. The questionnaire consisted try and red meat remained the most popular food classes. Nine of of a list of 223 food names, arranged in random order. the 15 most popular individual food items were fresh fruit. Sig- Respondents were asked to indicate how much they liked nificant differences were found between the food preferences of or disliked a food item using the same nine-point hedonic males and females for a number of food classes and individual scale previously described (6). Alternatively, respondents food items. Compared to the 1986 results there appears to be a could select a ‘never tried’ category. greater preference for nutritionally desirable items, more food from various cultures and more traditionally gourmet or ‘novel’ The list included a number of foods commonly availa- foods. It is hoped that the results of this survey may assist other ble and some ‘luxury’ foods, but excluded items that are nutrition and food service staff plan menus for Australian hospi- routinely available on most menus (including breakfast tal patients. -

1170 West Devon Avenue • Elk Grove Village, IL 60007 847.534.0600
1170 West Devon Avenue • Elk Grove Village, IL 60007 847.534.0600 • www.belvederebanquets.com Breakfast ORDERING INSTRUCTIONS Build Your Own Waffle Bar Call us at 847-534-0600! Choose from our selections or ask about customizing a menu. Fresh + Healthy We accommodate all dietary needs. Preparing local farm to table ingredients whenever possible. We are happy to place your order from 9am – 5pm every day. Dedicated to conserving resources to sustain a healthy environment. It is always helpful to have 48 hours advance notice Lunch but we will do our best within that time frame. Breakfast Platters & Baskets Minimum order for delivery is $150.00 Prices and menu are subject to change By the dozen medium (15) - large (25) Our kitchen reserves the right to notify you of a substitute item due to availability or quality of products – Bagels, organic cream cheese, FRENCH COUNTRY PLATTER sweet butter & fruit preserves $26 hard-boiled eggs, sliced smoked Cancellation within 12 hours may incur a 25% charge. ham, Swiss cheese, brie, tomatoes, – Muffins - freshly baked$32 whole grain mustard, cornichons, All caterings include black disposable serving pieces. flaky croissants, sliced baguette, Black disposable fork, knife, plate & napkin $1pp – Croissants filled & plain, sweet butter, fruit preserves $90/ $165 sweet butter, fruit preserves $36 SMOKED SALMON PLATTER Disposable racks & sternos $8 per set. smoked salmon, red onion, capers, Platters While tips are not required, they are greatly appreciated. cucumber, tomatoes, eggs, bagels, cream cheese $125/ -

Until the Meat Falls Off the Bone
University of Central Florida STARS Electronic Theses and Dissertations, 2004-2019 2009 Until The Meat Falls Off The Bone Holly Kapherr University of Central Florida Part of the Creative Writing Commons Find similar works at: https://stars.library.ucf.edu/etd University of Central Florida Libraries http://library.ucf.edu This Masters Thesis (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Electronic Theses and Dissertations, 2004-2019 by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Kapherr, Holly, "Until The Meat Falls Off The Bone" (2009). Electronic Theses and Dissertations, 2004-2019. 4071. https://stars.library.ucf.edu/etd/4071 UNTIL THE MEAT FALLS OFF THE BONE by HOLLY V. KAPHERR B.S., Brigham Young University, 2005 A.A.S., Culinary and Hospitality Institute of Chicago, 2006 A thesis submitted in partial fulfillment of the requirements for the degree of Master of Fine Arts in the Department of English in the College of Arts and Humanities at the University of Central Florida Orlando, Florida Fall Term 2009 ABSTRACT Though this work started as a formal academic cultural study, it stretched and squirmed and became not only an examination of the cultures themselves, but how I came to fit within those cultures. By combining my experiences travelling as a child and young adult as well as learning the craft of professional cooking, the essays in this work are highly centered around food and what food means both to me and to cultures throughout the world. -
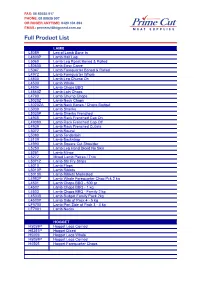
Full Product List
FAX: 08 89535 917 PHONE: 08 89535 907 OR ROGER ANYTIME: 0420 104 394 EMAIL: [email protected] FullCODE ProductPRODUCT List LAMB L5059 Leg of Lamb Bone In L4800P Lamb Half Leg L5060 Lamb Leg Roast Boned & Rolled L5060X Lamb Easy Carve L5047 Lamb Forequarter Boned & Rolled L4972 Lamb Forequarter Whole L4800 Lamb Leg Chump On L4500 Lamb Whole L4504 Lamb Chops BBQ L4860Z Lamb Loin Chops L4790 Lamb Chump Chops L5020Z Lamb Neck Chops L5020ZA Lamb Neck Bones / Chops Budget L5030 Lamb Shanks L5030P Lamb Shanks Frenched L4938 Lamb Rack Frenched Cap On L4938X Lamb Rack Frenched Cap Off L4939 Lamb Rack Frenched Cutlets L5072 Lamb Round L5080 Lamb Tenderloin L5109 Lamb Backstrap L4990 Lamb Square Cut Shoulder L5250 Lamb Leg Hand Diced No Skin L5251 Lamb Mince L5272 Mixed Lamb Pieces / Trim L5071Z Lamb Stir Fry Strips L5010 Lamb Flaps L5010P Lamb Riblets L5010X Lamb Riblets Marinated L4983P Lamb Whole Forequarter Chop Pck 2 kg L4501 Lamb Chops BBQ - 500 gr L4502 Lamb Chops BBQ - 1 kg L4503 Lamb Chops BBQ - Family 2 kg L4503B Lamb Budget Family Pack 2kg L4500P Lamb Side of Pack 4 - 5 kg LF5700 Lamb Part Side of Pack 3 - 4 kg LF7001 Lamb Necks HOGGET H5059P Hogget Legs Corned H5251P Hogget Diced H5059 Hogget Legs Whole H5059P Hogget Legs Corned H4505 Hogget Forequarter Chops CODE PRODUCT LAMB L5059 Leg of Lamb Bone In L4800P Lamb Half Leg L5060 Lamb Leg Roast Boned & Rolled L5060X Lamb Easy Carve L5047 Lamb Forequarter Boned & Rolled L4972 Lamb Forequarter Whole L4800 Lamb Leg Chump On L4500 Lamb Whole L4504 Lamb Chops BBQ L4860Z Lamb Loin Chops -

Beloit Daily News
Weekend Daily News Friday/Saturday/Sunday, September 6-8, 2019 | A1 Weekend SPORTS: Packers shuffl e Bears • B1 COUPON SAVINGS TODAY $202.15 Subscribers of the Beloit Daily News Daily News have enjoyed thousands in coupon www.beloitdailynews.com $2.50 savings over the last 12 months alone! Winnebago starting at $4.8M in red By AUSTIN MONTGOMERY Staff writer ROCKFORD — The full Winnebago County Board saw its first look at budget options for the 2020 budget on Thursday night, with a range of tough choices ahead for county board members. The current fiscal year ends Sept. 30 and a budget deficit looms. So far, the county is facing a $4.8 million deficit in 2020, accord- ing to Finance Committee Chairman Jaime Salgado. The county board was presented options for the upcoming fiscal year’s budget: an increase in the property tax levy combined with an increase in overall net new growth revenue; no change in the property tax levy; an increase in the property tax levy alone. A full rundown of the $4.13 million in pro- posed cuts, according to a memo circulated Austin Montgomery/Beloit Daily News ahead of Thursday’s meeting: Rockford resident Bill Lambert, 99, went scuba diving on his birthday on Thursday at Pearl Lake in South Beloit in a bid • Health insurance employer contribution to set the record of oldest person in the world to scuba dive. reduced by $1 million. • $500,000 shifted to the general fund levy. • Payments of $576,840 from the former City of Rockford 911 intergovernmental At 99, Rockford man still scuba diving agreement removed from the administrative budget. -

Raps Van Hees Gewürzmüller Product List
PRODUCT LIST RAPS▪ VAN HEES ▪ GEWÜRZMÜLLER March 2020 CBS Foodtech Pty Ltd 2/7 Jubilee Avenue Warriewood NSW 2102 . P - 02 9979 6722 F - 02 9979 6511 E - [email protected] W - www.cbsfoodtech.com.au RAPS SEASONINGS & ADDITIVES Simmer Sausage Type Products Code Description Function UOM R39610 Alpini 1kg Pure line no MSG kg R0130 Cabanossi 1kg Kabanos kg R1859 Cooked Pepperoni 1kg kg R0254 Debreziner 1kg kg R39366 Meat Loaf 1kg Pure line no MSG kg R39364 Senator Gold 1kg Pure line no MSG kg R0277 Vienna Gold 1kg Wiener, Frankfurter kg R0287 Vienna Red 1kg Wiener, Frankfurter kg Fresh Sausage Type Products Code Description Function UOM R0541 Bavarian Weisswurst 1kg Weisswurst sausage kg R0547 Cevapcici 1kg kg R39722 Chorizo 1kg no MSG kg R0520 Fresh Bratwurst 1kg fresh & frying sausage kg R0533 Merguez Bratwurst 1kg French style sausage kg R0554 Minced Meat Mix 1kg Mix for Rissoles & Crumb production kg R0530 Nürnberger Bratwurst 1kg fresh & simmer sausage kg R0532 Thüringer Bratwurst 1kg fresh & frying sausage kg Cooked Sausage Type Products Code Description Function UOM R39609 Bloodwurst 1kg Black Pudding no MSG kg R0325 Cristallfix 1.5kg Seasoned Gelatine kg R93875 Cristal Spice 1kg Pureline - Brawn, Presswurst seasoning no MSG kg R94811 Leberwurst NG 1kg Pureline no MSG kg Fermented Sausage Type Products Code Description Function UOM R0010387 Biostart Sprint 25g Starter Culture each R00174 Onion Mettwurst-Soft 1kg Spreadable Onion Mettwurst kg R0170 Pfefferjager 1kg Dry Salami, Green Pepper taste kg R0117 Salami Quick 1kg Dry Salami -
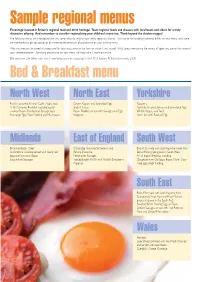
Sample Regional Menus
6476_BFF BuyGuide'05 ƒ WEBv 30/6/05 3:28 pm Page 12 Sample regional menus Encourage interest in Britain’s regional food and drink heritage! Team regional foods and cheeses with local beers and ciders for a truly distinctive offering. And remember to consider regionalising your children’s menu too. Think beyond the chicken nugget! The following menus are intended to give you some ideas for making your menu regionally distinct. This may be by including traditional dishes on your menu (and some are mentioned to get you going) or by increasing the emphasis of provenance on your existing menu. Why not mention the breed of sheep used for your roast lamb or the farm on which it was raised? What about mentioning the variety of apple you use or the name of your cheese producer? Specifying provenance on your menu will help make it more distinctive. Did you know £34 billion each year is now being spent on eating out in the UK? (Horizons FS Limited research, 2005) Bed & Breakfast menu North West North East Yorkshire Freshly squeezed Keswick Codlin Apple Juice. Craster Kippers and Scrambled Eggs. Popovers. A full Cumbrian Breakfast including locally- Singin’ Hinnies. Yo r kshire Smoked Salmon and Scrambled Eggs. smoked Bacon, Cumberland Sausage, local Bacon Floddies served with Sausages and Eggs. Whitby Kippers and Toast. free-range Eggs, Black Pudding and Mushrooms. Kedgeree. Yo rk Ham with Poached Egg. Midlands East of England South West Brummie Bacon Cakes. Cambridge Favourite Strawberry and Bucks Fizz made with sparkling wine made from Staffordshire Oatcake served with locally-laid Banana Smoothie.