Vaccinia Virus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Smallpox ( Variola )
Division of Disease Control What Do I Need to Know? Smallpox ( Variola ) What is Smallpox? Smallpox is a serious contagious disease that can be fatal. It is caused by the variola virus, a member of the Poxviridae family. The World Health Organization declared smallpox eliminated from the world in 1980. Who is at risk for Smallpox? Because smallpox has been eliminated, no one will be exposed to a naturally occurring case of smallpox. Smallpox is considered one of the viruses that maybe used in an attack by bioterrorists. Anyone who has not received smallpox vaccine is at risk if exposed to the virus. Also, people who received the vaccine may be at risk if exposed to smallpox because the protection declines five to ten years after one dose and possibly longer after two or more doses. The United States stopped routine childhood vaccination against smallpox in 1972. The last case of smallpox in the United States was in 1949 and the last naturally occurring case occurred in 1977 in Somalia. What are the symptoms of Smallpox? The first stage of the illness lasts two to five days with symptoms that include a high fever of 102˚F – 104˚F, a general feeling of discomfort, severe headache, backache, abdominal pain, and weakness. Most people will be severely ill and bedridden during this stage. By the third or fourth day of this stage, the fever usually drops. Following this stage, soars appear in the mouth and throat, but they may not be noticed by the infected person. The rash begins less than 24 hours after the sores in the mouth and throat appear. -

Poxviruses: Smallpox Vaccine, Its Complications and Chemotherapy
Virus Adaptation and Treatment Dovepress open access to scientific and medical research Open Access Full Text Article R E V IEW Poxviruses: smallpox vaccine, its complications and chemotherapy Mimi Remichkova Abstract: The threat of bioterrorism in the recent years has once again posed to mankind the unresolved problems of contagious diseases, well forgotten in the past. Smallpox (variola) is Department of Pathogenic Bacteria, The Stephan Angeloff Institute among the most dangerous and highly contagious viral infections affecting humans. The last of Microbiology, Bulgarian Academy natural case in Somalia marked the end of a successful World Health Organization campaign of Sciences, Sofia, Bulgaria for smallpox eradication by vaccination on worldwide scale. Smallpox virus still exists today in some laboratories, specially designated for that purpose. The contemporary response in the treatment of the post-vaccine complications, which would occur upon enforcing new programs for mass-scale smallpox immunization, includes application of effective chemotherapeutics and their combinations. The goals are to provide the highest possible level of protection and safety of For personal use only. the population in case of eventual terrorist attack. This review describes the characteristic features of the poxviruses, smallpox vaccination, its adverse reactions, and poxvirus chemotherapy. Keywords: poxvirus, smallpox vaccine, post vaccine complications, inhibitors Characteristics of poxviruses Smallpox (variola) infection is caused by the smallpox virus. This virus belongs to the genus of Orthopoxvirus included in the Poxviridae family. Poxviruses are one of the largest and most complexly structured viruses, known so far. The genome of poxviruses consists of a linear two-chained DNA and its replication takes place in the cytoplasm of the infected cell. -

Vaccinia Belongs to a Family of Viruses That Is Closely Related to the Smallpox Virus
VACCINIA INFECTION What is it? Vaccinia belongs to a family of viruses that is closely related to the smallpox virus. Because of the similarities between the smallpox and vaccinia viruses, the vaccinia virus is used in the smallpox vaccine. When this virus is used as a vaccine, it allows our immune systems to develop immunity against smallpox. The smallpox vaccine does not actually contain smallpox virus and cannot cause smallpox. Vaccination usually prevents smallpox infection for at least ten years. The vaccinia vaccine against smallpox was used to successfully eradicate smallpox from the human population. More recently, this virus has also become of interest due to concerns about smallpox being used as an agent of bioterrorism. How is the virus spread? Vaccinia can be spread by touching the vaccination site before it has fully healed or by touching clothing or bandages that have been contaminated with the live virus during vaccination. In this manner, vaccinia can spread to other parts of the body and to other individuals. It cannot be spread through the air. What are the symptoms of vaccinia? Vaccinia virus symptoms are similar to smallpox, but milder. Vaccinia may cause rash, fever, headache and body aches. In certain individuals, such as those with weak immune systems, the symptoms can be more severe. What are the potential side effects of the vaccinia vaccine for smallpox? Normal reactions are mild and go away without any treatment.These include: Soreness and redness in the arm where the vaccine was given Slightly swollen, sore glands in the armpits Low grade fever One in approximately three people will feel badly enough to miss school, work or recreational activities Trouble sleeping Serious reactions are not very common but can occur in about 1,000 in every 1 million people who are vaccinated for the first time. -

Smallpox Overview
SMALLPOX FACT SHEET Smallpox Overview The Disease Smallpox is a serious, contagious, and sometimes fatal infectious disease. There is no specific treatment for smallpox disease, and the only prevention is vaccination. The name smallpox is derived from the Latin word for “spotted” and refers to the raised bumps that appear on the face and body of an infected person. There are two clinical forms of smallpox. Variola major is the severe and most common form of smallpox, with a more extensive rash and higher fever. There are four types of variola major smallpox: ordinary (the most frequent type, accounting for 90% or more of cases); modified (mild and occurring in previously vaccinated persons); flat; and hemorrhagic (both rare and very severe). Historically, variola major has an overall fatality rate of about 30%; however, flat and hemorrhagic smallpox usually are fatal. Variola minor is a less common presentation of smallpox, and a much less severe disease, with death rates historically of 1% or less. Smallpox outbreaks have occurred from time to time for thousands of years, but the disease is now eradicated after a successful worldwide vaccination program. The last case of smallpox in the United States was in 1949. The last naturally occurring case in the world was in Somalia in 1977. After the disease was eliminated from the world, routine vaccination against smallpox among the general public was stopped because it was no longer necessary for prevention. Where Smallpox Comes From Smallpox is caused by the variola virus that emerged in human populations thousands of years ago. Except for laboratory stockpiles, the variola virus has been eliminated. -
Generalized Vaccinia After Smallpox Vaccination with Concomitant Primary Epstein Barr Virus Infection
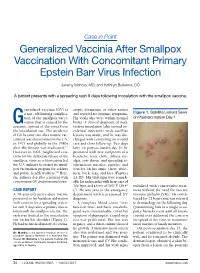
Case in Point Generalized Vaccinia After Smallpox Vaccination With Concomitant Primary Epstein Barr Virus Infection Jeremy Mandia, MD; and Kathryn Buikema, DO A patient presents with a spreading rash 9 days following inoculation with the smallpox vaccine. eneralized vaccinia (GV) is atopic dermatitis, or other rashes a rare, self-limiting complica- and reported no systemic symptoms. Figure 1. Satellite Lesions Seen tion of the smallpox vacci- His vitals also were within normal on Postvaccination Day 1 Gnation that is caused by the limits. A clinical diagnosis of inad- systemic spread of the virus from vertent inoculation (also termed ac- the inoculation site. The incidence cidental infection) with satellite of GV became rare after routine vac- lesions was made, and he was dis- cination was discontinued in the U.S. charged with counseling on wound in 1971 and globally in the 1980s care and close follow-up. Two days after the disease was eradicated.1,2 later, on postvaccination day 11, he However in 2002, heightened con- presented with new symptoms of a cerns for the deliberate release of the headache, fever, chills, diffuse my- smallpox virus as a bioweapon led algia, sore throat, and spreading er- the U.S. military to restart its small- ythematous macules, papules, and pox vaccination program for soldiers vesicles on his arms, chest, abdo- and public health workers.3,4 Here, men, back, legs, and face (Figures the authors describe a patient with 2A-2D). His vital signs were remark- concomitant GV and mononucleosis. able for tachycardia with heart rate of 100 bpm and a fever of 103º F (39.4º stabilized with conservative treat- CASE REPORT C). -
A Guide to Vaccinations for Parents
A GUIDE TO VACCINATIONS FOR PARENTS What are vaccines? When should my child be vaccinated? Why does my child need the HPV vaccine? HISTORY OF VACCINATIONS Smallpox is a serious infectious disease that causes fever and a distinctive, progressive 600 1796 skin rash. years ago Edward Jenner developed Variolation, intentionally a vaccine against smallpox. Cases of paralysis from polio in the U.S. exposing an individual to Almost 200 years later, in 1980, in the early 1950s: smallpox material, traces back the World Health Organization more than to 16th-century China. This declared that smallpox process resulted in a milder had been eradicated, 15,000 form of the disease. or wiped out. In the year 2017: Childhood vaccines can prevent 14 potentially serious 0 diseases or conditions throughout your child’s lifetime. 1955 1940s 1885 Jonas Salk’s polio vaccine The routine immunization Louis Pasteur developed a was proven safe and effective. schedule included vaccines vaccine against rabies. The Polio has now been eliminated against four potentially serious rabies vaccine series, which in the U.S., and organizations diseases (smallpox, diphtheria, can be given to people who are currently working tetanus, and pertussis). may have been exposed to to eradicate polio Now the schedule includes the virus, has made rabies worldwide. vaccines to prevent a total infection very rare in the of 14 conditions. United States. In the U.S., vaccines go through three phases of clinical trials to make sure they are safe and effective before they are licensed. 2006 Today The HPV vaccine was Vaccine research licensed in the U.S. -

Vaccinia Viruses As Vectors for Vaccine Antigens Vaccinia Viruses As Vectors for Vaccine Antigens
Vaccinia Viruses as Vectors for Vaccine Antigens Vaccinia Viruses as Vectors for Vaccine Antigens Proceedings of the Workshop on Vaccinia Viruses as Vectors for Vaccine Antigens, held November 13-14, 1984, in Chevy Chase, Maryland, U. S.A. Editor: GeraldV.Quinnan,Jr.,M.D. Director, Division of Virology Center for Drugs and Biologics Food and Drug Administration Bethesda, Maryland Elsevier New York • Amsterdam. Oxford .... i © 1985 by Elsevier Science Publishing Co., Inc. All rights reserved. This book has been registered with the Copyright Clearance Center, Inc. For further information, please contact the Copyright Clearance Center, Salem, Massachusetts. Published by: Elsevier Science Publishing Co., Inc. 52 Vanderbilt Avenue, New York, New York 10017 Sole distributors outside the United States and Canada: Elsevier Science Publishers B.V. P.O. Box 211, 1000 AE Amsterdam, the Netherlands Library of Congress Cataloging in Publication Data Workshop in Vaccinia Viruses as Vectors for Vaccine Antigens (1984: Chevy Chase, Md.) Vaccinia viruses as vectors for vaccine antigens. Includes index. I. Vaccines--Congresses. 2. Vaccinia--Congresses. 3. Viralantigens-- Congresses. 4. Smallpox--Congresses. I. Quinnan, Gerald V. 1I. Title. [DNLM: 1. Antigens, Viral--immunology--Congresses. 2. VacciniaVirus-- genetics--congresses. 3. VacciniaVirus--immunology--congresses. 4. Viral Vaccines--immunology--congresses. QW 165.5.P6 W926v 1984] QR189.W674 1984 615'.372 85-12960 ISBN 0-444-00984-1 Manufactured in the United States of America CONTENTS Preface ..... ..... ° . ............... ix Participants .............................. xi Part I: BIOLOGY OF VACCINIA AND OTHER ORTHOPOX VIRUSES I Chairpersons: G. Schild and J. Nakano Vaccinia Virus ...................... 3 D. Baxby Aspects of the Biology of Orthopox Viruses Relevant to the Use of Recombinant Vaccines as Field Vaccines ..... -

Medical Management of Biological Casualties Handbook
USAMRIID’s MEDICAL MANAGEMENT OF BIOLOGICAL CASUALTIES HANDBOOK Sixth Edition April 2005 U.S. ARMY MEDICAL RESEARCH INSTITUTE OF INFECTIOUS DISEASES FORT DETRICK FREDERICK, MARYLAND Emergency Response Numbers National Response Center: 1-800-424-8802 or (for chem/bio hazards & terrorist events) 1-202-267-2675 National Domestic Preparedness Office: 1-202-324-9025 (for civilian use) Domestic Preparedness Chem/Bio Helpline: 1-410-436-4484 or (Edgewood Ops Center – for military use) DSN 584-4484 USAMRIID’s Emergency Response Line: 1-888-872-7443 CDC'S Emergency Response Line: 1-770-488-7100 Handbook Download Site An Adobe Acrobat Reader (pdf file) version of this handbook can be downloaded from the internet at the following url: http://www.usamriid.army.mil USAMRIID’s MEDICAL MANAGEMENT OF BIOLOGICAL CASUALTIES HANDBOOK Sixth Edition April 2005 Lead Editor Lt Col Jon B. Woods, MC, USAF Contributing Editors CAPT Robert G. Darling, MC, USN LTC Zygmunt F. Dembek, MS, USAR Lt Col Bridget K. Carr, MSC, USAF COL Ted J. Cieslak, MC, USA LCDR James V. Lawler, MC, USN MAJ Anthony C. Littrell, MC, USA LTC Mark G. Kortepeter, MC, USA LTC Nelson W. Rebert, MS, USA LTC Scott A. Stanek, MC, USA COL James W. Martin, MC, USA Comments and suggestions are appreciated and should be addressed to: Operational Medicine Department Attn: MCMR-UIM-O U.S. Army Medical Research Institute of Infectious Diseases (USAMRIID) Fort Detrick, Maryland 21702-5011 PREFACE TO THE SIXTH EDITION The Medical Management of Biological Casualties Handbook, which has become affectionately known as the "Blue Book," has been enormously successful - far beyond our expectations. -

Smallpox.Pdf
Variola DISTRICT OF COLUMBIA DEPARTMENT OF HEALTH Division of Epidemiology, Disease Surveillance and Investigation 899 N. Capitol Street, NE, Suite 580 Washington, D.C. 20002 202-442-9371 Fax 202-442-8060 * www.dchealth.dc.gov What is Smallpox? • On rare occasions, the virus has spread through the air Smallpox is a serious, contagious, and sometimes fatal viral infectious in enclosed places such as buildings, buses, and disease. There are two clinical forms of smallpox. Variola major is the trains. severe and most common form of smallpox with a more extensive rash Smallpox is not known to be spread by insects or animals. and higher fever. Variola minor is a less common presentation of The smallpox virus is not strong and is killed by sunlight smallpox and a much less severe disease. and heat. Who gets Smallpox? How soon do symptoms appear? Smallpox is no longer seen as a disease anywhere in the world. This The symptoms can appear between seven and seventeen days, disease has been eradicated because of successful worldwide the average time is twelve to fourteen days, after coming in vaccination. The last case of smallpox in the United States was in contact with the virus that causes smallpox. During this time, 1949. The last naturally occurring case in the world was in 1977. After the infected person feels fine and is not contagious. the disease was eliminated from the world, routine vaccination against smallpox among the general public was stopped because it was no Is a person with Smallpox contagious? longer necessary for prevention. Yes, a person with smallpox is contagious. -

Evaluation of Recombinant Vaccinia Virus—Measles Vaccines in Infant Rhesus Macaques with Preexisting Measles Antibody
Virology 276, 202–213 (2000) doi:10.1006/viro.2000.0564, available online at http://www.idealibrary.com on Evaluation of Recombinant Vaccinia Virus—Measles Vaccines in Infant Rhesus Macaques with Preexisting Measles Antibody Yong-de Zhu,*,1 Paul Rota,† Linda Wyatt,‡ Azaibi Tamin,† Shmuel Rozenblatt,‡,2 Nicholas Lerche,* Bernard Moss,‡ William Bellini,† and Michael McChesney*,§,3 *The California Regional Primate Research Center and §Department of Pathology, School of Medicine, University of California, Davis, California 95616; †Measles Virus Section, Respiratory and Enteric Viruses Branch, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia 30333; and ‡Laboratory of Viral Diseases, National Institute of Allergy and Infectious Diseases, National Institutes of Health, Bethesda, Maryland 20892 Received June 20, 2000; returned to author for revision July 28, 2000; accepted August 1, 2000 Immunization of newborn infants with standard measles vaccines is not effective because of the presence of maternal antibody. In this study, newborn rhesus macaques were immunized with recombinant vaccinia viruses expressing measles virus hemagglutinin (H) and fusion (F) proteins, using the replication-competent WR strain of vaccinia virus or the replication- defective MVA strain. The infants were boosted at 2 months and then challenged intranasally with measles virus at 5 months of age. Some of the newborn monkeys received measles immune globulin (MIG) prior to the first immunization, and these infants were compared to additional infants that had maternal measles-neutralizing antibody. In the absence of measles antibody, vaccination with either vector induced neutralizing antibody, cytotoxic T cell (CTL) responses to measles virus and protection from systemic measles infection and skin rash. -

(ACIP) General Best Guidance for Immunization
Appendix 1: Glossary Adverse event. An undesirable medical condition that occurs following vaccination which might be truly caused by a vaccine, or it might be pure coincidence. Adverse reaction. An undesirable medical condition that has been demonstrated to be caused by a vaccine. Evidence for the causal relation is usually obtained through randomized clinical trials, controlled epidemiologic studies, isolation of the vaccine strain from the pathogenic site, or recurrence of the condition with repeated vaccination (i.e., rechallenge); synonyms include side effect and adverse effect. Adjuvant. A vaccine component distinct from the antigen that enhances the immune response to the antigen. Antitoxin. A solution of antibodies against a toxin. Antitoxin can be derived from either human (e.g., tetanus immune globulin) or animal (usually equine) sources (e.g., diphtheria and botulism antitoxin). Antitoxins are used to confer passive immunity and for treatment. Hyperimmune globulin (specific). Special preparations obtained from blood plasma from donor pools preselected for a high antibody content against a specific antigen (e.g., hepatitis B immune globulin, varicella-zoster immune globulin, rabies immune globulin, tetanus immune globulin, vaccinia immune globulin, cytomegalovirus immune globulin, botulism immune globulin). Immune globulin. A sterile solution containing antibodies, which are usually obtained from human blood. It is obtained by cold ethanol fractionation of large pools of blood plasma and contains 15%-18% protein. Intended for intramuscular administration, immune globulin is primarily indicated for routine maintenance of immunity among certain immunodeficient persons and for passive protection against measles and hepatitis A. General Best Practice Guidelines for Immunization: Appendix 1: Glossary 189 Immunobiologic. Antigenic substances (e.g., vaccines and toxoids) or antibody- containing preparations (e.g., globulins and antitoxins) from human or animal donors. -

(12) Patent Application Publication (10) Pub. No.: US 2009/0221523 A1 Tseng Et Al
US 2009.022 1523A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2009/0221523 A1 Tseng et al. (43) Pub. Date: Sep. 3, 2009 (54) NORTH-2'-DEOXY-METHANO- (86). PCT No.: PCT/US2O06/02O894 CARBATHYMIDNES AS ANTIVIRAL AGENTS AGAINST POXVIRUSES S371 (c)(1), (2), (4) Date: Apr. 3, 2009 (76) Inventors: Christopher K. Tseng, Related U.S. Application Data Burtonsville, MD (US); Victor E. (60) Provisional application No. 60/684.811, filed on May Marquez, Montgomery Village, 25, 2005. MD (US) Publication Classification (51) Int. Cl. Correspondence Address: A 6LX 3L/7072 (2006.01) KNOBBE, MARTENS, OLSON & BEAR, LLP A6IP3L/20 (2006.01) 2040 MAINSTREET, FOURTEENTH FLOOR (52) U.S. Cl. .......................................................... S14/SO IRVINE, CA 92.614 (US) (57) ABSTRACT (21) Appl. No.: 11/920,881 A method for the prevention or treatment of poxvirus infec tion by administering an effective amount of an antiviral agent comprising cyclopropanated carbocyclic 2'-deoxy (22) PCT Filed: May 25, 2006 nucleoside to an individual in need thereof is provided. Patent Application Publication Sep. 3, 2009 Sheet 2 of 3 US 2009/022 1523 A1 HSV-2 TK Goalpox TK humonl TK VV TK VOriod TK monkeypox TK fowlpox TK HSV-1 K african swine fever virus TK VZV TK EBV TK FIF2 Patent Application Publication Sep. 3, 2009 Sheet 3 of 3 US 2009/022 1523 A1 CC (N)-MCT CDV VC – -2 48.61 site - 2322 2027 . US 2009/022 1523 A1 Sep. 3, 2009 NORTH-2-DEOXY. breaks depended on the isolation of infected individuals and METHANOCARBATHYMIDNES AS the vaccination of close contacts.