Chemical Terrorismterrorism • Chemical Agents Act Quickly
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Disaster Response and Biological/Chemical Terrorism
Disaster Response and Biological/Chemical Terrorism Information Packet Prepared by: Emergency Medical Services Department October 2001 Disaster Response and Biological/Chemical Terrorism Clearinghouse Information The College has been very active in disaster planning and response as well as biological/chemical terrorism preparation for a number of years. The membership section, Disaster Medicine, was the first membership section organized in 1989. They have been one of the largest in membership and one of the most active. The EMS Department maintains information for members and the public on disaster response and biological/chemical terrorism topics in a variety of formats and publications. POLICY STATEMENTS The College has current policies addressing the following: · Disaster Data Collection (Oct. 2000) · Disaster Medical Service (June 2000) · Support for National Disaster Medical System-NDMS (Mar. 1999) · Handling of Hazardous Materials (June 1999) TEXT BOOKS The College developed and published the text: Community Medical Disaster Planning and Evaluation Guide through a section grant with the Disaster Medicine Section. This is an excellent guide for developing or updating a hospital or city/county disaster plan. While biological or chemical agents are not specifically mentioned, many of the same disaster planning and response issues remain the same. This text can be ordered through the College bookstore at 1-800-798- 1822, ext. 6for $69.00, item number 513000-1020. NBC TASK FORCE The College’s nuclear, biological and chemical (NBC) Task Force recently completed a grant with the Department of Health and Human Services (HHS), Office of Emergency Preparedness (OEP) to develop objectives, content and competencies for the training of emergency medical technicians, emergency physicians, and emergency nurses to care for casualties resulting from nuclear, biological, or chemical (NBC) incidents. -

Thiosulfate De Sodium Sterop
Thiosulfate de Sodium Sterop 1. DENOMINATION DU MEDICAMENT THIOSULFATE DE SODIUM STEROP 1g/5ml solution injectable 2. COMPOSITION QUALITATIVE ET QUANTITATIVE Substance active : Une ampoule de 5ml contient 1g de thiosulfate de sodium dans de l’eau pour préparations injectables. 1 ml de solution contient 200mg de thiosulfate de sodium. Pour la liste complète des excipients, voir rubrique 6.1. 3. FORME PHARMACEUTIQUE Solution injectable. 4. DONNEES CLINIQUES 4.1 Indications thérapeutiques - Antidote dans le traitement des intoxications par les cyanures ainsi que par le nitroprussiate de sodium. - Prévention des effets néphrotoxiques du cisplatine. Thiosulfate de Sodium Sterop © Pharma.be Pagina 1 van 6 4.2 Posologie et mode d’administration Mode d'administration Pour voie intraveineuse lente. Posologie Intoxications par les cyanures: Adultes: La posologie habituelle est de 12,5 g de thiosulfate de sodium, administré par voie I.V. sur une période de 5 à 10 minutes. Enfants: La posologie habituelle est de 412,5 mg de thiosulfate de sodium par kg, administré par voie I.V. à la vitesse de 0,625 à 1,25 g/minute sur une période de 5 à 10 minutes. Si les symptômes persistent ou réapparaissent dans la demi-heure ou dans l’heure ayant suivi la première injection, une seconde injection de thiosulfate de sodium est nécessaire avec comme posologie la moitié de celle de la première injection. En prévention des effets néphrotoxiques du cisplatine: Chez l'adulte, la posologie initiale est de 9 g de thiosulfate de sodium par m2 de surface corporelle, administré par voie I.V. Elle est suivie par l'injection de 1,2 g de thiosulfate de sodium par m2 de surface corporelle par heure, en perfusion I.V. -

High-Threat Chemical Agents: Characteristics, Effects, and Policy Implications
Order Code RL31861 CRS Report for Congress Received through the CRS Web High-Threat Chemical Agents: Characteristics, Effects, and Policy Implications Updated September 9, 2003 Dana A. Shea Analyst in Science and Technology Policy Resources, Science, and Industry Division Congressional Research Service ˜ The Library of Congress High-Threat Chemical Agents: Characteristics, Effects, and Policy Implications Summary Terrorist use of chemical agents has been a noted concern, highlighted after the Tokyo Sarin gas attacks of 1995. The events of September 11, 2001, increased Congressional attention towards reducing the vulnerability of the United States to such attacks. High-threat chemical agents, which include chemical weapons and some toxic industrial chemicals, are normally organized by military planners into four groups: nerve agents, blister agents, choking agents, and blood agents. While the relative military threat posed by the various chemical types has varied over time, use of these chemicals against civilian targets is viewed as a low probability, high consequence event. High-threat chemical agents, depending on the type of agent used, cause a variety of symptoms in their victims. Some cause death by interfering with the nervous system. Some inhibit breathing and lead to asphyxiation. Others have caustic effects on contact. As a result, chemical attack treatment may be complicated by the need to identify at least the type of chemical used. Differences in treatment protocols for the various high-threat agents may also strain the resources of the public health system, especially in the case of mass casualties. Additionally, chemical agents trapped on the body or clothes of victims may place first responders and medical professionals at risk. -

How States Respond to Terrorist Attacks: an Analysis of the Variance in Responses
How States Respond to Terrorist Attacks: An Analysis of the Variance in Responses A Thesis Submitted to The University of Michigan In partial fulfillment of the requirements for the degree of Honors Bachelor of Arts Department of Political Science Lauren A Bondarenko March 2014 Advisor: Allan Stam Table of Contents Acknowledgements………………………………………………………………………………………… i Acronyms/Abbreviations………………………………………………………………………………... ii Preface…………………………………………………………………………………………………………… 1 Chapter 1: Introduction Conceptualizations………………………………………………………………………………. 4 National Security…………………………………………………………………………….. 4 Terrorism……………………………………………………………………………………….. 6 Literature Review………………………………………………………………………………… 8 Institutions……………………………………………………………………………………... 8 National Security as a Collective Action Problem……………………………… 11 American Institutional Reform………………………………………………………… 12 European Institutional Reform………………………………………………………… 15 Applying the Balance of Threat Theory…………………………………………….. 18 What the Literature is Missing…………………………………………………………. 21 Hypotheses…………………………………………………………………………………………... 22 Chapter Previews…………………………………………………………………………………. 23 Chapter 2: Methodology Use of the Global Terrorism Database…………………………………………………… 25 Reason for Database Selection…………………………………………………………. 25 Information Missing in the Database………………………………………………... 25 Creation of My Dataset…………………………………………………………………………. 27 Using GTD………………………………………………………………………………………. 27 Coding System………………………………………………………………………………… 28 Case Selection……………………………………………………………………………………… 29 A Note on Style……………………………………………………………………………………. -

Adult BLS Standing Orders • Ensure EMS Provider Safety, Consider HAZMAT Activation
Imperial County Public Health Department Emergency Medical Services Agency Policy/Procedure/Protocol Manual Treatment Protocols Date: 07/01/2021 Poisoning/Intoxication/Envenomation - Adult Policy #9160A Adult BLS Standing Orders • Ensure EMS provider safety, consider HAZMAT activation. Recognize, Notify, Isolate • Universal Patient Protocol • Do not approach patient or location if scene safety is in question • Obtain accurate history of incident: o Name of product or substance o Quantity ingested, and/or duration of exposure o Time elapsed since exposure o If safe and accessible, bring medications or bottles to hospital • Move victim(s) to safe environment • Externally decontaminate - PRN • Continuously monitor ECG, blood pressure, pulse oximetry, and capnography (if ALS present) PRN • Give oxygen and provide airway support per Airway Policy • Contact Poison Control Center as needed 1 (800) 222-1222 Suspected Opioid Overdose with Respirations <12 RPM • If possible, avoid the use of a supraglottic device prior to the administration of naloxone • Administer naloxone 0.1 mg/kg, max of 2 mg IN. May repeat up to three (3) times, q5min • May assist family/friends on-scene with administration of patient’s own naloxone • NOTE - Use with caution in opioid dependent pain management patients • Assess vitals, with specific attention to respiratory rate and respiratory drive • Note pupil exam • Note drug paraphernalia or medication bottles near patient Suspected Stimulant Overdose with Sudden Hypoventilation, Oxygen Desaturation, or Apnea • High flow -

Hydrogen Sulfide Metabolite, Sodium Thiosulfate
International Journal of Molecular Sciences Review Hydrogen Sulfide Metabolite, Sodium Thiosulfate: Clinical Applications and Underlying Molecular Mechanisms Max Y. Zhang 1,2, George J. Dugbartey 1,2,3, Smriti Juriasingani 1,3 and Alp Sener 1,2,3,4,* 1 Matthew Mailing Center for Translational Transplant Studies, London Health Sciences Center, Western University, London, ON N6A 5A5, Canada; [email protected] (M.Y.Z.); [email protected] (G.J.D.); [email protected] (S.J.) 2 London Health Sciences Center, Multi-Organ Transplant Program, Western University, London, ON N6A 5A5, Canada 3 London Health Sciences Center, Department of Surgery, Division of Urology, Western University, London, ON N6A 5A5, Canada 4 Department of Microbiology & Immunology, Schulich School of Medicine & Dentistry, University of Western Ontario, London, ON N6A 3K7, Canada * Correspondence: [email protected]; Tel.: +1(519) 6633352 Abstract: Thiosulfate in the form of sodium thiosulfate (STS) is a major oxidation product of hydrogen sulfide (H2S), an endogenous signaling molecule and the third member of the gasotransmitter family. STS is currently used in the clinical treatment of acute cyanide poisoning, cisplatin toxicities in cancer therapy, and calciphylaxis in dialysis patients. Burgeoning evidence show that STS has antioxidant and anti-inflammatory properties, making it a potential therapeutic candidate molecule that can target multiple molecular pathways in various diseases and drug-induced toxicities. This review Citation: Zhang, M.Y.; Dugbartey, discusses the biochemical and molecular pathways in the generation of STS from H2S, its clinical G.J.; Juriasingani, S.; Sener, A. usefulness, and potential clinical applications, as well as the molecular mechanisms underlying these Hydrogen Sulfide Metabolite, clinical applications and a future perspective in kidney transplantation. -

Ingestions, Intoxications, and the Critically Ill Child Poisoning in Children
Ingestions, Intoxications, and the Critically Ill Child Poisoning in Children • 1 million cases of exposure to toxins in children younger than 6 years reported in the U.S. In 1993 • estimated that another 1 million exposures to toxins not reported • 1% have moderate or major life-threatening symptoms • 60-100 deaths annually in the U.S Poisoning in Children Less Than 5 Years Old • accounts for 85-90% of pediatric poisoning • is generally accidental • secondary to exploratory behavior and lack of supervision • tend to involve single agent ingestions Poisoning in Children Over 5 Years Old • accounts for 10-15% of pediatric poisoning • is generally intentional • secondary to suicide attempts or gestures, or to intoxications and inadvertent overdose • tend to involve multiple agent ingestions General Concepts for Pediatric Poisoning • Prevention • Initial Stabilization • Diagnosis • Specific Antidotes Management of the Poisoned Child • Treat the Patient, Not the Poison --patient-specific treatment is safer, less expensive, and more effective Management of the Poisoned Child • Stabilization --Airway --Breathing --Circulation --Disability (neurologic) Management of the Poisoned Child • Respiratory Failure --airway obstruction from secretions, refluxed gastric contents, airway muscle relaxation --respiratory muscle rigidity --loss of respiratory drive --pulmonary edema Management of the Poisoned Child • Cardiovascular Collapse --arteriolar dilation --venous dilation --myocardial depression --dysrhythmias Management of the Poisoned Child • Neurologic -
Antidote List
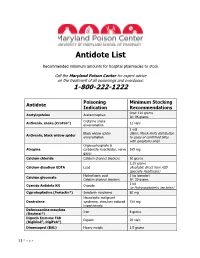
Antidote List Recommended minimum amounts for hospital pharmacies to stock Call the Maryland Poison Center for expert advice on the treatment of all poisonings and overdoses: 1-800-222-1222 Poisoning Minimum Stocking Antidote Indication Recommendations Oral: 120 grams Acetylcysteine Acetaminophen IV: 96 grams Crotaline snake Antivenin, snake (CroFab®) 12 vials envenomation 1 vial Black widow spider (Note: Merck limits distribution Antivenin, black widow spider envenomation to cases of confirmed bites with symptoms only) Organophosphate & Atropine carbamate insecticides, nerve 165 mg gases Calcium chloride Calcium channel blockers 10 grams 2.25 grams Calcium disodium EDTA Lead (Available direct from ASD Specialty Healthcare) Hydrofluoric acid 1 kg (powder) Calcium gluconate Calcium channel blockers IV: 30 grams 1 kit Cyanide Antidote Kit Cyanide (or Hydroxocobalamin, see below) Cyproheptadine (Periactin®) Serotonin syndrome 80 mg Neuroleptic malignant Dantrolene syndrome, stimulant-induced 720 mg hyperthermia Deferoxamine mesylate Iron 8 grams (Desferal®) Digoxin Immune FAB Digoxin 20 vials (Digibind®, DigiFab®) Dimercaprol (BAL) Heavy metals 1.5 grams 1 | P a g e Maryland Poison Center Antidote List – continued Poisoning Minimum Stocking Antidote Indication Recommendations DMSA (Succimer, Chemet®) Heavy metals 2000 mg Folic acid Methanol IV: 150 mg Flumazenil (Romazicon®) Benzodiazepines 10 mg Fomepizole (Antizol®) Ethylene glycol, methanol 12 grams Beta blockers, Glucagon 50 mg calcium channel blockers Hydroxocobalamin (Cyanokit®) Cyanide -
Antidote Stocking Tier C
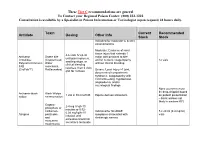
These Tier C recommendations are general To Contact your Regional Poison Center: (800) 222-1222 Consultation is available by a Specialist in Poison Information or Toxicologist (upon request) 24 hours daily. Toxin Current Recommended Antidote Dosing Other Info Stock Stock Indicated for moderate to severe envenomations Moderate: Evidence of local tissue injury that extends 1 4-6 vials IV q2-4h Antivenin Snake bite major joint proximal to bite until pain improves, Crotalidae (Copperhead, and/or numeric coagulopathy 12 vials swelling stops, or Polyvalent Immune Water without clinical bleeding clinical bleeding FAB moccasins, resolves, then 2 vials (CroFab™) Rattlesnakes) Severe: Local injury >1 joint, q6h for 3 doses documented compartment syndrome, coagulopathy with clinical bleeding, hypotension, angioedema, and/or neurological findings None (currently must be drop-shipped based Antivenin-black Black Widow 1 vial in 50 ml of NS Equine derived antivenom on patient presentation widow envenomation – black widows not likely in western KY) Organo- 2-4 mg IV q5-10 phosphate or minutes or 0.02- carbamate Indicated for SLUDGE 5 x 20 ml (0.4 mg/ml) 0.08 mg/kg/hr IV Atropine pesticides symptoms associated with vials infusion until and cholinergic excess excessive bronchial muscarine secretions terminate mushrooms These Tier C recommendations are general To Contact your Regional Poison Center: (800) 222-1222 Consultation is available by a Specialist in Poison Information or Toxicologist (upon request) 24 hours daily. Antidote Current Recommended Toxin -

Non-Military Security and Global Order the Impact of Extremism, Violence and Chaos on National and International Security
Non-Military Security and Global Order The Impact of Extremism, Violence and Chaos on National and International Security Peter Chalk Non-Military Security and Global Order Also by Peter Chalk WEST EUROPEAN TERRORISM AND COUNTER-TERRORISM: The Evolving Dynamic Non-Military Security and Global Order The Impact of Extremism, Violence and Chaos on National and International Security Peter Chalk National Security Research Division RAND Corporation Arlington, Virginia First published in Great Britain 2000 by MACMILLAN PRESS LTD Houndmills, Basingstoke, Hampshire RG21 6XS and London Companies and representatives throughout the world A catalogue record for this book is available from the British Library. ISBN 0–333–77373–X First published in the United States of America 2000 by ST. MARTIN’S PRESS, LLC, Scholarly and Reference Division, 175 Fifth Avenue, New York, N.Y. 10010 ISBN 0–312–23167–9 Library of Congress Cataloging-in-Publication Data Chalk, Peter. Non-military security and global order : the impact of extremism, violence, and chaos on national and international security / Peter Chalk. p. cm. Includes bibliographical references and index. ISBN 0–312–23167–9 (cloth) 1. Internal security. 2. Security, International. I. Title. HV6419 .C53 2000 363.3'2—dc21 00–021169 © Peter Chalk 2000 All rights reserved. No reproduction, copy or transmission of this publication may be made without written permission. No paragraph of this publication may be reproduced, copied or transmitted save with written permission or in accordance with the provisions of the Copyright, Designs and Patents Act 1988, or under the terms of any licence permitting limited copying issued by the Copyright Licensing Agency, 90 Tottenham Court Road, London W1P 0LP. -

Assessing Al-Qaeda's Chemical Threat
ISSN 1988-5237 AthenaIntelligence.org Assessing al-Qaeda’s Chemical T hreat René Pita Athena Paper, Vol. 2, No 2 Article 3/5 April 17, 2007 www.athenaintelligence.org 27 ISSN 1988-5237 AthenaIntelligence.org Introduction After the 11 September 2001 (9/11) terrorist attacks in the United States, there is a high perception of risk of possible attacks with chemical weapons (CW ), especially by groups affiliated or associated with the al-Qaeda terrorist network. Earlier, in 1994 and 1995, Aum Shinrikyo, a religious organization in Japan, used sarin, a nerve chemical warfare agent, in attacks in Matsumoto City and on the Tokyo subway, causing a large number of casualties. These terrorist attacks had a big impact on the chemical defence and intelligence communities but not on other circles, perhaps because a chemical attack by a religious organization in Japan seemed something far removed from the reality of the rest of the world. But this changed after 9/11 when the mailing of letters containing anthrax spores, accompanied by images of the attacks on the W orld Trade Center towers, increased the concern about weapons of mass destruction (W MD) attacks, including by CW . As a religious terrorist group, al-Qaeda does not fit the assumption made by Brian Jenkins in 1975 that “terrorists want a lot of people watching and a lot of people listening, and not a lot of people dead.”1 This statement fits better with secular terrorist groups. But for religious terrorist groups like al-Qaeda, “divine duty” results in disappearance of moral restraints that would justify “a lot of people dead” in their terrorist attacks,2 such as the 9/11 ones. -

Dialyzability of Medications During Intermittent Hemodialysis
DialyzeIHD: Dialyzability of Medications During Intermittent Hemodialysis % Dialyzed % Dialyzed % Dialyzed % Dialyzed IHD Dosing; Administration IHD Dosing; Administration IHD Dosing; Administration IHD Dosing; Administration Timing Drug (Type of Drug (Type of Drug (Type of Drug (Type of Timing Around HD Session Timing Around HD Session Around HD Session Dialyzer) Timing Around HD Session Dialyzer) Dialyzer) Dialyzer) 0.25-0.5mg PO Q8H PRN, Insulin Aspart, Pentamidine 0 4mg/kg IV Q24-36H, Not recommended for use, Clonazepam N/A Reduce to 25-50% of normal dose Acarbose N/A Administer anytime during HD Insulin Detemir, Isethionate (N/A) Administer anytime during HD Administer anytime during HD N/A and titrate, Administer anytime Insulin Glargine, 0.1-0.4mg PO Q8-12H, during HD Normal dose and titrate based on 100-150mg PO Q12-24H, <5 Insulin Lispro Acebutolol N/A Clonidine Administer anytime during HD; No target free or corrected total Administer post-HD (Low Flux) Phenytoin Dose post-HD if hypotensive 75-300mg PO Q24H, (Low Flux) phenytoin level, Normal dose based on indication, 0 Administer anytime during HD Acetaminophen N/A 75mg PO Q24H, Irbesartan Administer anytime during HD; Dose Administer anytime during HD Clopidogrel N/A (N/A) Administer anytime during HD post-HD if hypotensive No 15-45mg PO Q24H, Pioglitazone 2.5-5mg/kg IV/PO Q24H, (N/A) Administer anytime during HD 40-60 250-500mg PO Q6H or 1-2g IV Q4- 100mg IV weekly to monthly, Acyclovir Administer post-HD over 60 Cloxacillin N/A Iron Dextran N/A (N/A) 6H, Administer anytime