Embryology of Branchial Region
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Download PDF Version
FIG. 4–1 Dorsal aspect of the 10-somite embryo. 24 IV the fourth week of life somite and neural tube period I. EMBRYO PROPER caudal openings of the tube are called neuropores. The rostral neuropore closes between 18 and 20 somites. The caudal neuro- A. EXTERNAL APPEARANCE pore closes at 25 somites. Figs. 4–1, 4–2 1. The specimens measure approximately 1 to 3.5 mm in length Brain and have 1 to 29 pairs of somites. Three brain subdivisions are present in the cranial portion of the 2. The head and tail folds move the attachment of the amnion tube and are named, from cranial to caudal, the prosencephalon, to the ventral side of the head and tail regions, respectively. mesencephalon and rhombencephalon. The boundary between the The lateral body folds move the amnion attachment to the pros- and mesencephalon is demarcated by a ventral bend, called ventrolateral surface in the midportion of the embryo. the cephalic flexure. An external groove and a prominent swelling 3. The head region is elevated above the yolk sac by the large on the medial surface of the neural plate may also demarcate the pericardial sac, the midportion lies upon the yolk sac and the boundary. The boundary between the mes- and rhombencephalon caudal region is curved toward the yolk sac. is distinguished by a groove on the medial and lateral surfaces of 4. The embryo possesses somites, which are apparent through the neural plate or tube. the ectoderm. 5. The neural tube develops from the neural plate and remains Prosencephalon open at each end for 2 to 4 days. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

Insect Digestion
INSECT DIGESTION Zoo 514 Dr. Reem Alajmi Insect digestive system The alimentary canal is concerned with digestion and absorption of food stuffs. Different parts of the gut are concerned with different aspects of these functions. In fluid feeding insects digestion begin before the food is ingested through the injection or regurgitation of enzymes on to the food . In general it occurs in the mid gut (most of the enzymes are produced). The enzymes break down the complex substances in the food into simple substances which can be absorbed and assimilated. Enzymes function optimally only within limited range of pH and temperature. Absorption is passive process in some cases , but in others active transport occurs. Absorption of water is important in terrestrial insects , rectum remove water from faeces. • Insects of different groups consume astonishing variety of foods, including watery xylem sap, vertebrate blood, dry wood, bacteria and algae and the internal tissues of other insects. • Types of mouth parts correlates with the diets of insect. Also gut structure and function affected by nutrient composition of the food eaten by insect. • Insects that take solid food typically have a wide, straight, short gut with strong musculature and obvious protection from abrasion (especially in the midgut, which has no cuticular lining). • These features are most obvious in solid-feeders with rapid throughput of food, as in many insects and plant-feeding caterpillars In contrast, insects feeding on blood, sap or nectar usually have long, narrow, convoluted guts to allow maximal contact with the liquid food; here, protection from abrasion is unnecessary. The most obvious gut specialization of liquid-feeders is a mechanism for removing excess water to concentrate nutrient substances prior to digestion, as seen in hemipterans. -
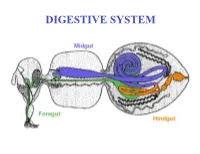
DIGESTIVE SYSTEM Generalized Insect Alimentary Tract the Digestive System Is Just a Tube Within a Surrounding Tube Called the Body
DIGESTIVE SYSTEM Generalized insect alimentary tract The digestive system is just a tube within a surrounding tube called the body. It starts with a mouth and ends with the anus. What goes on in between depends on the insect, its life stage and what it eats. The origin of the digestive tract. At the anterior pole of the embryo an indentation forms that will be the foregut or stomodeum. At the other end a similar thing occurs and the proctodeum or hindgut is formed. Both are lined by cuticle. They both are of ectodermal origin while the midgut is of mesodermal origin and is also called the mesenteron. This different origin of the midgut from the endoderm and not the ecotoderm probably explains why it is not lined with cuticle Anterior midgut invagination. In the bottom photo note the invagination starting forming the ventral furrow lumen (VF) MIDGUT FORMATION IN THE EMBRYO PMG in the above embryo shows the posterior midgut invagination cup where the posterior invagination shown in the drawing on the right will take place. Photo of Drosophila embryo. Hindgut invagination DIGESTIVE SYSTEM The digestive tract not only aids in obtaining, processing and digesting food molecules - It is the largest endocrine tissue in both humans and insects. The digestive system is involved in: 1. Obtaining food 2. Mechanically breaking it down into smaller particles that facilitate digestive enzymes acting on them 3. Enzymatic breakdown of larger food molecules into molecules that can pass through the digestive tract (midgut) and enter the hemolymph 4. Produces molecules or MESSENGERS (eg. -

Syndromes of the First and Second Branchial Arches, Part 1: Embryology and Characteristic REVIEW ARTICLE Defects
Syndromes of the First and Second Branchial Arches, Part 1: Embryology and Characteristic REVIEW ARTICLE Defects J.M. Johnson SUMMARY: A variety of congenital syndromes affecting the face occur due to defects involving the G. Moonis first and second BAs. Radiographic evaluation of craniofacial deformities is necessary to define aberrant anatomy, plan surgical procedures, and evaluate the effects of craniofacial growth and G.E. Green surgical reconstructions. High-resolution CT has proved vital in determining the nature and extent of R. Carmody these syndromes. The radiologic evaluation of syndromes of the first and second BAs should begin H.N. Burbank first by studying a series of isolated defects: CL with or without CP, micrognathia, and EAC atresia, which compose the major features of these syndromes and allow more specific diagnosis. After discussion of these defects and the associated embryology, we proceed to discuss the VCFS, PRS, ACS, TCS, Stickler syndrome, and HFM. ABBREVIATIONS: ACS ϭ auriculocondylar syndrome; BA ϭ branchial arch; CL ϭ cleft lip; CL/P ϭ cleft lip/palate; CP ϭ cleft palate; EAC ϭ external auditory canal; HFM ϭ hemifacial microsomia; MDCT ϭ multidetector CT; PRS ϭ Pierre Robin sequence; TCS ϭ Treacher Collins syndrome; VCFS ϭ velocardiofacial syndrome adiographic evaluation of craniofacial deformities is nec- major features of the syndromes of the first and second BAs. Ressary to define aberrant anatomy, plan surgical proce- Part 2 of this review discusses the syndromes and their radio- dures, and evaluate the effects of craniofacial growth and sur- graphic features: PRS, HFM, ACS, TCS, Stickler syndrome, gical reconstructions.1 The recent rapid proliferation of and VCFS. -

Branchial and Thyroglossal Cysts and Fistulae
University of Nebraska Medical Center DigitalCommons@UNMC MD Theses Special Collections 5-1-1942 Branchial and thyroglossal cysts and fistulae George G. Johnson University of Nebraska Medical Center This manuscript is historical in nature and may not reflect current medical research and practice. Search PubMed for current research. Follow this and additional works at: https://digitalcommons.unmc.edu/mdtheses Part of the Medical Education Commons Recommended Citation Johnson, George G., "Branchial and thyroglossal cysts and fistulae" (1942). MD Theses. 929. https://digitalcommons.unmc.edu/mdtheses/929 This Thesis is brought to you for free and open access by the Special Collections at DigitalCommons@UNMC. It has been accepted for inclusion in MD Theses by an authorized administrator of DigitalCommons@UNMC. For more information, please contact [email protected]. BRANCHIAL & THYROGLOSSAL CYSTS & FISTULAE GEORGE N. JOHNSON SENIOR THESIS PRESENTED TO THE COLLEGE OF MEDICINE APRIL 6, 1942 INDEX BRANCHIAL CYSTS AND FISTULAE Page Introduction l Historical background 1 Embryological background 10 Wenglowski's embryology of the Branehia.l apparatus 14 Arey 1 s embryology of the Branchial apparatus 16 Symptoms 22 Age incidence 23 Diagnosis 24 Treatment 27 ------THYROGLOSSAL --DUCT CYSTS AND ----FISTULAE Historical background 32 Embryological history 34 Weller's embryology of the Thyroid 35 Arey's embryology of the Thyroid 39 Clinical features 40 Location 45 Age incidence 46 Pathology 47 Symptoms & Diagnosis 48 Treatment 51 481309 INTRODUCTION This thesis will be confined entirely to branch- ial and thyroglossal duct cysts and fistulas with the purpose of covering the two separate disease entities in one paper. It is also important to mention that because of the close similarity of these two patho- . -
![The Pharyngeal Arches [PDF]](https://docslib.b-cdn.net/cover/8257/the-pharyngeal-arches-pdf-1328257.webp)
The Pharyngeal Arches [PDF]
24.3.2015 The Pharyngeal Arches Dr. Archana Rani Associate Professor Department of Anatomy KGMU UP, Lucknow What is Pharyngeal Arch? • Rod-like thickenings of mesoderm present in the wall of the foregut. • They appear in 4th-5th weeks of development. • Contribute to the characteristic external appearance of the embryo. • As its development resembles with gills (branchia: Greek word) in fishes & amphibians, therefore also called as branchial arch. Formation of Pharyngeal Arches Lens N Pharyngeal Apparatus Pharyngeal apparatus consists of: • Pharyngeal arches • Pharyngeal pouches • Pharyngeal grooves/clefts • Pharyngeal membrane Pharyngeal Arches • Pharyngeal arches begin to develop early in the fourth week as neural crest cells migrate into the head and neck region. • The first pair of pharyngeal arches (primordium of jaws) appears as a surface elevations lateral to the developing pharynx. • Soon other arches appear as obliquely disposed, rounded ridges on each side of the future head and neck regions. Le N Pharyngeal Arches • By the end of the fourth week, four pairs of pharyngeal arches are visible externally. • The fifth and sixth arches are rudimentary and are not visible on the surface of the embryo. • The pharyngeal arches are separated from each other by fissures called pharyngeal grooves/clefts. • They are numbered in craniocaudal sequence. Pharyngeal Arch Components • Each pharyngeal arch consists of a core of mesenchyme. • Is covered externally by ectoderm and internally by endoderm. • In the third week, the original mesenchyme is derived from mesoderm. • During the fourth week, most of the mesenchyme is derived from neural crest cells that migrate into the pharyngeal arches. Structures in a Pharyngeal Arch Arrangement of nerves supplying the pharyngeal arch (in lower animals) Fate of Pharyngeal Arches A typical pharyngeal arch contains: • An aortic arch, an artery that arises from the truncus arteriosus of the primordial heart. -

BGD B Lecture Notes Docx
BGD B Lecture notes Lecture 1: GIT Development Mark Hill Trilaminar contributions • Overview: o A simple tube is converted into a complex muscular, glandular and duct network that is associated with many organs • Contributions: o Endoderm – epithelium of the tract, glands, organs such as the liver/pancreas/lungs o Mesoderm (splanchnic) – muscular wall, connective tissue o Ectoderm (neural crest – muscular wall neural plexus Gastrulation • Process of cell migration from the epiblast through the primitive streak o Primitive streak forms on the bilaminar disk o Primitive streak contains the primitive groove, the primitive pit and the primitive node o Primitive streak defines the body axis, the rostral caudal ends, and left and right sides Thus forms the trilaminar embryo – ectoderm, mesoderm, endoderm • Germ cell layers: o ectoderm – forms the nervous system and the epidermis epithelia 2 main parts • midline neural plate – columnar epithelium • lateral surface ectoderm – cuboidal, containing sensory placodes and skin/hair/glands/enamel/anterior pituitary epidermis o mesoderm – forms the muscle, skeleton, and connective tissue cells migrate second migrate laterally, caudally, rostrally until week 4 o endoderm – forms the gastrointestinal tract epithelia, the respiratory tract and the endocrine system cells migrate first and overtake the hypoblast layer line the primary yolk sac to form the secondary yolk sac • Membranes: o Rostrocaudal axis Ectoderm and endoderm form ends of the gut tube, no mesoderm At each end, form the buccopharyngeal -

Development Of, Tongue, Thyroid, Sinus and Salivary Glands
Development of, tongue, thyroid, sinus and salivary glands Development of tongue • 1st ,2nd, 3rd, 4th pharyngeal arches • Median swelling- tuberculum impar • Two lateral swellings –lingual • Caudal medial swelling- hypobrachial eminence Anterior 2/3 of the tongue: • Formation: median and lateral tongue buds that arise from the floor of the 1st pharyngeal arch and then grow rostrally. • thus it is formed by fusion of -- • tuberculum impar , • two lingual swellings • The tongue buds are then invaded by occipital myoblasts that form the intrinsic muscles of the tongue. • Thus anterior 2/3rd of tonguer is supplied by lingual branch of mandibular nerve ,(post trematic nerve of this arch) and chorda tympani nerve( pretrematic nerve of arch) • posterior 1/3rd of tongue is supplied by glossopharyngeal nerve ( nerve of 3rd arch) • Most posterior 1/3rd of tongue is supplied by superior laryngeal nerve ( nerve of 4th arch) • Musculature of tongue is derived from occipital myotomes --explains nerve supply by hypoglossal nerve, nerve of these myotomes. Posterior 1/3rd of tongue • formed from cranial part of hypobranchial eminence ( copula) • the second arch mesoderm gets buried below the surface . • the third arch mesoderm grows over it to fuse with mesoderm of first arch . • posterior one third of tongue thus formed by third arch mesoderm. • posterior most part of tongue is derived from fourth arch • Thus swellings from the floor of the 3rd and 4th pharyngeal arches overgrow the 2nd arch and fuse with the anterior 2/3 of the tongue. • posterior 1/3 of the tongue is derived from the 3rd and 4th arches • Intrinsic musculature is also derived from occipital myoblasts. -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -

Resecting Branchial Cysts, Fistulae and Sinuses
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY RESECTING BRANCHIAL FISTULAE, SINUSES AND CYSTS Johan Fagan Failure of a branchial cleft to involute may thymus and parathyroid (Figures 3, 4). The manifest as an epithelial-lined cyst, sinus 1st branchial cleft evolves into the external or fistula. Sinuses open either onto the auditory meatus (Figure 3). skin, or into the oro- or hypopharynx. Branchial anomalies may be diagnosed at any age but present most commonly in infancy and childhood as a cutaneous sinus, a cyst or an abscess. The differential diagnosis of a cystic lateral neck mass in- cludes thymic, parathyroid and thyroid cysts, cystic metastases (papillary thyroid carcinoma, oropharyngeal squamous cell carcinoma, skin cancer), tuberculous cold abscess, lymphatic malformation, plunging ranula, and laryngocoele. The existence of branchiogenic carcinoma is controversial. Cystic metastases to cervical lymph nodes originating from oropharyngeal squamous cell carcinoma occur far more commonly and should be suspected particularly in adult patients presenting with cystic masses in Levels 2 or 3 of the neck. Surgical excision is the standard of care. An understanding of the embryology of the Figure 1: Branchial arches 1 - 4 with branchial apparatus is required to diagnose intervening branchial clefts http://php.med. and operate on such patients. unsw edu.au/embryology/index.php?title=2010 _Lecture_11 Embryology The branchial apparatus develops during the 2nd - 6th weeks of life. At this stage the neck of the foetus is shaped like a hollow tube with circumferential ridges called branchial arches which are separated inter- nally by branchial pouches and externally by clefts (Figure 1).