Baseline Survey and Pre-KAP (Knowledge, Attitude and Practice) Study in Chitwan, Rupandehi and Banke Districts for One Health Asia Programme (OHAP) in Nepal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Achham, Banke, Chitwan, and Pachthar Districts
Technical Assistance Consultant’s Report Project Number: 44168-012 Capacity Development Technical Assistance (CDTA) October 2013 Nepal: Mainstreaming Climate Change Risk Management in Development (Financed by the Strategic Climate Fund) District Baseline Reports: Department of Roads (DOR) Achham, Banke, Chitwan, and Pachthar Districts Prepared by ICEM – International Centre for Environmental Management This consultant’s report does not necessarily reflect the views of ADB or the Government concerned, and ADB and the Government cannot be held liable for its contents. (For project preparatory technical assistance: All the views expressed herein may not be incorporated into the proposed project’s design. MOSTE | Mainstreaming climate change risk management in development | DoR District Baseline TA – 7984 NEP October, 2013 Mainstreaming Climate Change Risk Management in Development 1 Main Consultancy Package (44768-012) ACHHAM DISTRICT BASELINE: DEPARTMENT OF ROADS (DOR) Prepared by ICEM – International Centre for Environmental Management METCON Consultants APTEC Consulting Prepared for Ministry of Science, Technology and Environment, Government of Nepal Environment Natural Resources and Agriculture Department, South Asia Department, Asian Development Bank Version B i MOSTE | Mainstreaming climate change risk management in development | DoR District Baseline TABLE OF CONTENTS 1 ACHHAM DISTRICT ........................................................................................................... 1 1.1 District Sector Master Plan ............................................................................................ -

Achhame, Banke, Chitwan, Kathmandu, and Panchthar Districts
Technical Assistance Consultant’s Report Project Number: 44168-012 Capacity Development Technical Assistance (CDTA) October 2013 Nepal: Mainstreaming Climate Change Risk Management in Development (Financed by the Strategic Climate Fund) District Baseline Reports: Department of Local Infrastructure Development and Agricultural Roads (DOLIDAR) Achhame, Banke, Chitwan, Kathmandu, and Panchthar Districts Prepared by ICEM – International Centre for Environmental Management This consultant’s report does not necessarily reflect the views of ADB or the Government concerned, and ADB and the Government cannot be held liable for its contents. (For project preparatory technical assistance: All the views expressed herein may not be incorporated into the proposed project’s design. MOSTE | Mainstreaming climate change risk management in development | DoLIDAR District Baseline TA – 7984 NEP October, 2013 Mainstreaming Climate Change Risk Management in Development 1 Main Consultancy Package (44768-012) ACHHAM DISTRICT BASELINE: DEPARTMENT OF LOCAL INFRASTRUCTURE DEVELOPMENT & AGRICULTURAL ROADS (DOLIDAR) Prepared by ICEM – International Centre for Environmental Management METCON Consultants APTEC Consulting Prepared for Ministry of Science, Technology and Environment, Government of Nepal Environment Natural Resources and Agriculture Department, South Asia Department, Asian Development Bank Version B 1 MOSTE | Mainstreaming climate change risk management in development | DoLIDAR District Baseline TABLE OF CONTENTS 1 ACHHAM DISTRICT .......................................................................................................... -

Study Report on "Comminity Based Organizations(Cbos): Landscape
Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 Democratizing civil society at grassroots SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Mukta S. Lama Suresh Dhakal Lagan Rai Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] ii Acknowledgements This report is a result of contribution of many people in multiple ways. Foremost, we extend our deepest and heartfelt gratitude to members of Community Based Organizations across the districts for sharing us with their time, insight and experiences. The study benefited greatly from support and cooperation of the Plan field staff and partner agencies in Sunsari, Morang, Makwanpur, Rautahat, Bara, and Banke districts and the Regional Operational Support Unit teams. We would like to thank Ms. Chhing Lamu Sherpa, Mr. Kalbhan Rai, Dr. Chandra K. Sen, Mr. R. P. Gupta and Krishna Ghimire for their valuable inputs on the study. Dr. Chandi Chapagai, Plan Nepal Country Training Coordinator deserves special thanks for coordinating the whole exercise. We would like to express our deep appreciation to Shobhakar Vaidhya for his keen interest, insightful comments and his enthusiasm for incorporating the learning into the institutional policies and procedures. Thanks are also due to the Ms. Minty Pande, Country Director for her encouragement and comments. Similarly we very much appreciate the support of Mr. -

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -
Nepal's 9 Minimum Characteristics of a Disaster Resilient Community
Flagship 4 Handbook Nepal’s 9 Minimum Characteristics of a Disaster Resilient Community Published July 2013 Flagship 4: Integrated Community Based Disaster Risk Reduction/Management Flagship 4 is led by Government of Nepal’s Ministry of Federal Affairs and Local Development in partnership with the International Federation of Red Cross and Red Crescent Societies Flagship 4 is part of the Nepal Risk Reduction Consortium. An electronic version of this handbook can be downloaded from www.flagship4.nrrc.org.np The handbook is available in both English and Nepali Copies of the handbook and other documents can be obtained from IFRC’s Flagship 4 coordinator i Nepal’s 9 Minimum Characteristics Nepal’s 9 Minimum Characteristics of a Disaster Resilient Community of a Disaster Resilient Community About This Handbook Glossary of Terms Community Based Disaster Risk Reduction / Management Since the inception of the 9 minimum Handbook contents CBDRR/M characteristics of a disaster resilient community CDMC Community Disaster Management Committee in Nepal, there have been many questions Case studies by Government, implementing agencies, One attempt to provide guidance on DDC District Development Committee researchers, and community members on how operationalising the characteristics has DDMC District Disaster Management Committee to operationalise these characteristics. These been to collect a number of case studies questions have led to the formation of this from implementing agencies in Nepal. DDRC District Disaster Response Committee handbook which contains more information Each case study corresponds to a specific DEECC District Energy, Environment and Climate Change Division about each characteristic and examples of how characteristic and outlines how the they can be applied in interventions. -

Ltzt Ul/Alsf Uxgtf -K|Ltzt Affs Nifd0fk'/, G/}Gfk'/, S7s'oof, Sfnfkmf6f
1 2 lhNnfx?sf] ul/aLsf] b/, ul/aLsf] ljifdtf / ul/aLsf] uxgtf @)^* lhNnf uf=lj=;=sf gfd ul/aLsf b/ ul/aLsf ljifdtf ul/aLsf uxgtf -k|ltzt_ -k|ltzt_ -k|ltzt_ afFs nIfd0fk'/, g/}gfk'/, s7s'Oof, sfnfkmf6f 56.46(10.17) 16.88(4.71) 6.8(2.36) afFs kmQ]k'/, lagf}gf 39.35(10.08) 9.88(3.57) 3.53(1.55) afFs d6]lxof, u+ufk'/ 57.98(9.77) 17.65(4.76) 7.2(2.47) afFs a}hfk'/, vf;s'Zdf 33.01(9.93) 7.52(3.07) 2.49(1.22) afFs sGrgk'/ 25.26(8.58) 5.33(2.37) 1.67(0.88) afFs dxfb]jk'/L 18.17(7.47) 3.62(1.9) 1.1(0.67) afFs sf]xnk'/ 12.48(4.8) 2.59(1.25) 0.81(0.45) afFs /em]gf 10.56(4.91) 2.02(1.17) 0.59(0.4) afFs zD;]/u~h 28.96(8.92) 6.92(2.92) 2.4(1.23) afFs u+ufk'/ 41.53(10.17) 10.8(3.7) 3.96(1.64) afFs sDbL 37.03(9.74) 9.65(3.48) 3.57(1.54) afFs dlgsfk'/ 21.98(6.69) 5.21(2.09) 1.8(0.86) afFs ags66L 47.84(9.58) 13.46(4.05) 5.2(1.94) afFs a]txgL 58.1(10.14) 17.37(4.79) 6.98(2.42) afFs xf]lnof 66.99(9.02) 22.33(5.27) 9.66(2.96) afFs k'/}gL, pbok'/ k'/}gf 40.52(9.93) 10.57(3.7) 3.88(1.66) afFs a;'b]jk'/ 23.52(7.13) 5.36(2.11) 1.79(0.83) afFs vf;sf/sf+bf] 9.42(3.62) 1.97(0.96) 0.62(0.35) afFs lkk/xjf, ejfgLk'/ 34.43(9.16) 8.42(3.11) 2.96(1.32) afFs lxl/ldlgof 42.28(10.72) 10.85(3.92) 3.93(1.73) afFs ags6jf 19.47(7.35) 4.12(2.01) 1.31(0.76) afFs lr;fkfgL 18.44(6.32) 3.93(1.72) 1.26(0.65) afFs gf}j:tf 22.23(7.75) 4.8(2.18) 1.55(0.83) afFs l6l6lx/Lof 23.97(8.41) 5.15(2.4) 1.65(0.92) afFs /lgofk'/ 36.22(9.38) 9.01(3.39) 3.2(1.49) afFs l;tfk'/ 11.86(5.22) 2.34(1.28) 0.71(0.45) afFs ;f]gk'/ 36.36(9.79) 8.96(3.35) 3.16(1.43) afFs p9/fk'/ 37.83(10.01) 9.42(3.46) 3.35(1.48) afFs a]nef/, ;fOufpF 45.89(9.99) 12.47(4.01) 4.71(1.87) afFs k/;k'/ 27.7(8.75) 6.62(2.82) 2.3(1.18) afFs /fwfk'/ 5.57(3.21) 0.95(0.63) 0.26(0.2) afFs afu]Zj/L 8.67(3.98) 1.62(0.9) 0.47(0.3) afFs sh'/fv'b{, OGb|k'/, a]nx/L 34.1(8.42) 8.57(2.95) 3.08(1.28) afFs g]kfnu+h gu/kflnsf 9.65(3.35) 2.17(0.93) 0.73(0.36) gf]6 M sf]i7s -_ leq /x]sf] c+sn] ;DalGwt ;"rssf] e|dfz+ -k|ltzt_ nfO{ hgfpF5 . -
Draft IEE: Nepal
Draft Initial Environmental Examination September 2011 NEP: Integrated Urban Development Project- Nepalganj Municipality Prepared by the Government of Nepal, Ministry of Physical Planning and Works for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 5 August 2011) Currency unit – Nepalese rupee (NRs/NRe) NRs1.00 = $0.01391 $1.00 = NRs 71.874 ABBREVIATIONS ADB - Asian Development Bank AIDS - Acquired Immune Deficiency Syndrome CITES - Convention on International Trade in Endangered Species of Wild Fauna and Flora DOR - Department of Roads DSC - Design and Supervision Consultants DSWSS - Department of Water Supply and Sewerage DUDBC - Department of Urban Development and Building Construction DWEC - District Wage Evaluation Committee EARF - Environmental Assessment and Review Framework EIA - Environmental Impact Assessments EIA - environmental impact assessment EMEP - Environmental Mitigation Execution Plan EMP - Environmental Management Plan EPA - Environment Protection Act EPR - Environment Protection Rules GRC - Grievance Redress Mechanism HIV - Human Immunodeficiency Virus IEE - Initial Environmental Examination MLD - Ministry of Local Development MOE - Ministry of Environment MOE - Ministry of Environment MOF - Ministry of Finance MPMC - Municipal Project Management Committee MPPW - Ministry of Physical Planning and Works NDWQS - National Drinking Water Quality Standards NGO - Non-Government Oranization NTFP - non-timber forest products NWSC - Nepal Water Supply Corporation OHS - Occupational Health and Safety PCO - project coordination -

Hariyo Ban Program Ii Threats and Vulnerabilities
HARIYO BAN PROGRAM II (2016-2021) THREATS AND VULNERABILITIES ASSESSMENT OF PARKS AND CORRIDORS OF TERAI ARC LANDSCAPE Prepared by: WWF in partnership with CARE, FECOFUN and NTNC P.O. Box 7660 Kathmandu, Nepal 21 April 2017 © WWF 2017 All rights reserved Any reproduction of this publication in full or in part must mention the title and credit WWF. Published by WWF Nepal PO Box: 7660 Baluwatar, Kathmandu, Nepal T: +977 1 4434820, F: +977 1 4438458 [email protected] , www.wwfnepal.org/hariyobanprogram Disclaimer This Threats and Vulnerabilities Assessment of Parks and Corridors in Terai Arc Landscape is made possible by the generous support of the American people through the United States Agency for International Development (USAID). The contents are the responsibility of the authors and do not necessarily reflect the views of USAID or the United States Government. Contents INTRODUCTION ........................................................................................................................................................5 METHODOLOGY ........................................................................................................................................................6 Chitwan National Park and Buffer Zone ...................................................................................................................7 Threat Ratings of Chitwan National Park and Buffer Zone...................................................................................8 Barandabhar Corridor ........................................................................................................................................... -

POPULATION STATUS and HABITAT SUITABILITY of SARUS CRANE (Antigone Antigone, Linnaeus, 1758) in BANKE DISTRICT, NEPAL
POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus, 1758) IN BANKE DISTRICT, NEPAL SHRADDHA TIWARI T.U. Registration No. 5-1-33-471-2005 T.U. Examination Roll No: 050 Batch: 2070/2071 A thesis submitted in partial fulfillment of the requirements for the award of the degree of Master of Science in Zoology with special paper Ecology and Environment. Submitted to Central Department of Zoology Institute of Science and Technology Tribhuvan University Kirtipur, Kathmandu Nepal December, 2016 DECLARATION I hereby declare that the work presented in this thesis has been done by myself, and has not been submitted elsewhere for the award of any degree. All sources of information have been specifically acknowledged by references to the author(s) or institution(s). ……………………… Date: ................................. Ms. Shraddha Tiwari i TRIBHUVAN UNIVERSITY CENTRAL DEPARTMENT OF ZOOLOGY Kirtipur, Kathmandu, Nepal RECOMMENDATION This is to recommend that the thesis entitled “POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus 1758) IN BANKE DISTRICT, NEPAL” has been carried out by Ms. Shraddha Tiwari for the partial fulfillment of Master’s Degree of Science in Zoology with special paper Ecology and Environment. This is her original work and has been carried out under my supervision. To the best of our knowledge, this thesis work has not been submitted for any other degree in any institutions. Date:-………………………………. ………………………………….. Supervisor Nanda Bahadur Singh, PhD Professor Central Department of Zoology Tribhuvan University ii TRIBHUVAN UNIVERSITY CENTRAL DEPARTMENT OF ZOOLOGY Kirtipur, Kathmandu, Nepal RECOMMENDATION This is to recommend that the thesis entitled “POPULATION STATUS AND HABITAT SUITABILITY OF SARUS CRANE (Antigone antigone, Linnaeus 1758) IN BANKE DISTRICT, NEPAL” has been carried out by Ms. -

Nepal EGRP-RFP-FY19-P006
Request for Proposal (RFP) - Nepal EGRP-RFP-FY19-P006 Amendment #1 Commodity/Service Required: Endline Assessment of Early Grade Reading Program (EGRP) Type of Procurement: One Time Purchase Order Type of Contract: Firm Fixed Price Term of Contract: December 01, 2019- April 15, 2020 Contract Funding: AID-367-TO-15-00002 This Procurement supports: USAID’s Early Grade Reading Program (EGRP) Submit Proposal to: The Selection Committee RTI- USAID Early Grade Reading Program House no. 46/64, Uttar Dhoka, Lazimpat, Kathmandu, Nepal Original Date of Issue of RFP: Tuesday, July 23, 2019 Date Questions from Supplier Due: Wednesday, July 31, 2019 11:00 a.m. Nepal Standard Time email [email protected] Note:- Q&A will be posted on RTI website Pre-submission conference on RFP Thursday, August 01, 2019, 10:00 to 11:00 AM at EGRP meeting hall, Lazimpat. Date Proposal Due: Thursday, August 22, 2019, 11:00 a.m. Nepal Standard Time Approximate Purchase Order effective date to December 01, 2019 Successful Bidder(s): Method of Submittal: Hard Copy of proposal along with the soft copy in a CD or pen drive. Proposal documents should be submitted in a closed envelope with wax seal (laah chhap) and clearly marked with the solicitation number to the following address: The Selection Committee RTI-USAID Early Grade Reading Program House no. 46/64, Uttar Dhoka, Lazimpat, Kathmandu, Nepal. Bidder’s quote must be printed on the organization’s letterhead, signed, stamped, dated and must include all items and/or services. In addition, each and every pages of the proposal documents needs to be signed and stamped by the authorized person in order to be considered for evaluation. -
NEPAL, YEAR 2016: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 9 February 2017
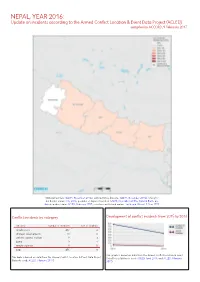
NEPAL, YEAR 2016: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 9 February 2017 National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; China/In- dia border status: CIA, 2006; geodata of disputed borders: GADM, November 2015a; Natural Earth, un- dated; incident data: ACLED, February 2017; coastlines and inland waters: Smith and Wessel, 1 May 2015 Conflict incidents by category Development of conflict incidents from 2015 to 2016 category number of incidents sum of fatalities riots/protests 432 4 strategic developments 11 0 violence against civilians 9 3 battle 3 1 remote violence 1 0 total 456 8 This graph is based on data from the Armed Conflict Location & Event This table is based on data from the Armed Conflict Location & Event Data Project Data Project (datasets used: ACLED, April 2016, and ACLED, February (datasets used: ACLED, February 2017). 2017). NEPAL, YEAR 2016: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 9 FEBRUARY 2017 LOCALIZATION OF CONFLICT INCIDENTS Note: The following list is an overview of the incident data included in the ACLED dataset. More details are available in the actual dataset (date, location data, event type, involved actors, information sources, etc.). In the following list, the names of event locations are taken from ACLED, while the administrative region names are taken from GADM data which serves as the basis for the map above. In Central, 207 incidents killing 1 person were reported. The following locations were affected: Bhaktapur, Bharatpur, Bidur, Birganj, Bishrampur, Brahmapuri, Chandranigahapur, Chandrapur, Charikot, Chautara, Dharhari, Dhulikhel, Dhunche, Gamhariya Birta, Gaur, Gokarneshwar, Jaleswar, Janakpur, Kalaiya, Kamalamai, Kathmandu, Kirtipur, Kritipur, Madi, Mahottari, Malangwa, Patan, Rasuwa Ghadhi, Sanepa. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome