Tracking Violence in Timor-Leste a Sample of Emergency Room Data, 2006–08
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Socio-Economic Impact Assessment of COVID-19 in Timor-Leste
Socio-Economic Impact Assessment of COVID-19 in Timor-Leste United Nations Timor-Leste 2020 with technical lead from UNDP Socio-economic impact assessment of COVID-19 in Timor-Leste Research Team Dolgion Aldar (UNDP SEIA and Livelihoods Consultant), Noelle Poulson (UNDP MSME Consultant), Ricardo Santos (UNDP Social Protection Consultant), Frank Eelens (UNFPA Sampling and Data Analysis Consultant), Guido Peraccini (UNFPA Database Consultant), Carol Boender (UN Women Gender Consultant), Nicholas McTurk (UNFPA), Sunita Caminha (UN Women), Scott Whoolery (UNICEF), Munkhtuya Altangerel (UNDP) and Ronny Lindstrom (UNFPA). Acknowledgements This Socio-Economic Impact Assessment of COVID-19 in Timor-Leste was led by UNDP and conducted in collaboration with UNFPA, UN Women and UNICEF. This study benefited from comments and feedback from all UN agencies in Timor-Leste including FAO (Solal Lehec, who provided valuable inputs to the sections related to food security in this report), ILO, IOM, WFP, WHO, the UN Human Rights Adviser Unit and UN Volunteers. SEIA team expresses its gratitude to the UN Resident Coordinator, Roy Trivedy, and the entire UN Country Team in Timor-Leste for providing overall guidance and support. We would like to sincerely thank all of the community members in Baucau, Bobonaro, Dili, Oecusse and Viqueque who participated in the SEIA questionnaires and interviews for being open and willing to share their stories and experiences for the development of this report. We would also like to thank the numerous individuals in government offices, institutions and organizations around the country who shared their time, expertise and insights to strengthen our understanding of the broader socio- economic context of Timor-Leste. -

Timor-Leste Building Agribusiness Capacity in East Timor
Timor-Leste Building Agribusiness Capacity in East Timor (BACET) Cooperative Agreement 486-A-00-06-00011-00 Quarterly Report July 01 - September 30, 2010 Submitted to: USAID/Timor-Leste Dili, Timor-Leste Angela Rodrigues Lopes da Cruz, Agreement Officer Technical Representative Submitted by: Land O’Lakes, Inc. International Development Division P. O. Box 64281 St. Paul, MN 55164-0281 U.S.A. October 2010 © Copyright 2010 by Land O'Lakes, Inc. All rights reserved. Building Agribusiness Capacity in East Timor CA # 486-A-00-06-00011-00 BUILDING AGRIBUSINESS CAPACITY IN EAST TIMOR USAID CA# 486-A-00-06-00011-00 Quarterly Report July - September 2010 Name of Project: Building Agribusiness Capacity in East Timor Locations: Fuiloro, Lautem District Maliana, Bobonaro District Natarbora, Manatutu District Dates of project: September 22, 2006 – September 30, 2011 Total estimated federal funding: $6,000,000 Total federal funding obligated: $6,000,000 Total project funds spent to September 30, 2010: $5,150,425 Contact in Timor-Leste: Michael J. Parr, Chief of Party Telephone: +670 331-2719 Mobile: +670 735-4382 E-mail: [email protected] Summary: BACET directly contributes to USAID/Timor- Leste’s agriculture and workforce development strategies for economic growth. though categorized as a capacity building and workforce development activity, many of the key activities of BACET have included infrastructure improvements, which are longer-term in nature. Similarly, teacher training and changed teaching methods have long-term impact. Quarterly Report July - September 2010 Land O'Lakes, Inc. Building Agribusiness Capacity in East Timor CA # 486-A-00-06-00011-00 Table of Contents 1. -

Dili to Baucau Highway Project Project Administration Manual
Project Administration Manual Project Number: 50211-001 Loan Number: LXXXX October 2016 Democratic Republic of Timor-Leste: Dili to Baucau Highway Project ABBREVIATIONS ADB = Asian Development Bank ADF = Asian Development Fund APFS = audited project financial statements CQS = consultant qualification selection DMF = design and monitoring framework EARF = environmental assessment and review framework EIA = environmental impact assessment EMP = environmental management plan ESMS = environmental and social management system GACAP = governance and anticorruption action plan GDP = gross domestic product ICB = international competitive bidding IEE = initial environmental examination IPP = indigenous people plan IPPF = indigenous people planning framework LAR = land acquisition and resettlement LIBOR = London interbank offered rate NCB = national competitive bidding NGOs = nongovernment organizations PAI = project administration instructions PAM = project administration manual PIU = project implementation unit QBS = quality based selection QCBS = quality- and cost based selection RRP = report and recommendation of the President to the Board SBD = standard bidding documents SGIA = second generation imprest accounts SOE = statement of expenditure SPS = Safeguard Policy Statement SPRSS = summary poverty reduction and social strategy TOR = terms of reference CONTENTS _Toc460943453 I. PROJECT DESCRIPTION 1 II. IMPLEMENTATION PLANS 2 A. Project Readiness Activities 2 B. Overall Project Implementation Plan 3 III. PROJECT MANAGEMENT ARRANGEMENTS 4 A. Project Implementation Organizations – Roles and Responsibilities 4 B. Key Persons Involved in Implementation 5 C. Project Organization Structure 6 IV. COSTS AND FINANCING 7 A. Detailed Cost Estimates by Expenditure Category 8 B. Allocation and Withdrawal of Loan Proceeds 9 C. Detailed Cost Estimates by Financier 10 D. Detailed Cost Estimates by Outputs/Components 11 E. Detailed Cost Estimates by Year 12 F. Contract and Disbursement S-curve 13 G. -
Dili to Baucau Highway Project
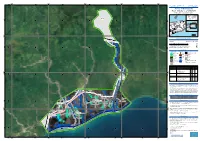
Updated Corrective Action Plan Project Number: 50211-001 May 2018 TIM: Dili to Baucau Highway Project Prepared by Ministry of Development and Institutional Reform for the Asian Development Bank. The Updated Corrective Action Plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB’s Board of Directors, Management or staff, and may be preliminary in nature. In preparing any country programme or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Democratic Republic of Timor-Leste Ministry of Development and of Institutional Reform Dili to Baucau Highway Project CORRECTIVE ACTION PLAN (CAP) Completion Report Package A01-02 (Manatuto-Baucau) May 2018 Democratic Republic of Timor-Leste Corrective Action Plan (CAP) Ministry of Development and of Institutional Reform Completion Report Dili to Baucau Highway Project Table of Contents List of Tables ii List of Figures iii Acronyms iv List of Appendices v 1 INTRODUCTION 1 1.1 Objectives 1 1.2 Methodology 2 2 THE PROJECT 3 2.1 Overview of the Project 3 2.2 Project Location 3 3 LEGAL AND POLICY FRAMEWORK 5 3.1 Scope of Land Acquisition and Resettlement 5 3.2 Definition of Terms Use in this Report 5 4 RESETTLEMENT POLICY FRAMEWORK 0 5 THE RAP PROCESS 0 5.1 RAP Preparation 0 5.1.1 RAP of 2013 0 5.1.2 RAP Validation in 2015 0 5.1.3 Revalidation -

Unfulfilled Expectations Victims’ Perceptions of Justice and Reparations in Timor-Leste
InternationalInternational Center Center Center for“These Transitional MedalsUnfulfilled Don’t Expectations: Feed Justice Us”: Victims’ Victims’ perceptions perceptions of of justice justice and and reparations reparations inin Timor-LesteTimor-Leste for Transitionalfor Transitional Justice Justice Unfulfilled Expectations Victims’ perceptions of justice and reparations in Timor-Leste February 2010 Picture/ Photo www.ictj.org 1 INISIATIVA ne’e HETAN APOIU HUSI UNIAUN EUROPEIA International Center Unfulfilled Expectations: Victims’ perceptions of justice and reparations in Timor-Leste for Transitional Justice Women victims resting in front of the CAVR office during a victims’ healing workshop, 2004. Photo by Poriaman Sitanggang for CAVR. www.ictj.org 2 International Center Unfulfilled Expectations: Victims’ perceptions of justice and reparations in Timor-Leste for Transitional Justice February 2010 Unfulfilled Expectations Victims’ perceptions of justice and reparations in Timor-Leste www.ictj.org 3 International Center Unfulfilled Expectations: Victims’ perceptions of justice and reparations in Timor-Leste for Transitional Justice ICTJ Brussels 11 Bischoffsheim Boulevard, 8th floor Brussels, 1000, Belgium Tel + 322 227 6140 Fax + 322 227 6148 Acknowledgement The ICTJ would like to thank the victims of the 1975 – 1999 conflict who participated in discussions and provided the ideas, opinions and information necessary for producing this research paper. ICTJ also thanks the organizations that facilitated the victims consultation workshops in the 13 districts in 2008, namely East Timor Women’s Communication Forum (Fokupers), HAK (Human Rights and Law Association) and the Commission for Justice and Peace of Baucau, and the Post-CAVR Technical Secretariat. ICTJ would like to acknowledge the primary authors of this paper, Naomi Kinsella and Manuela Leong Pereira. -
2018 Timor-Leste Study Tour Report
1 Table of Contents About the Tour ...................................................................................................................... 4 Timor-Leste Overview .......................................................................................................... 6 History ................................................................................................................................. 7 Politics ............................................................................................................................... 10 The Economy .................................................................................................................... 13 Society and Culture……………………………………………………………………………16 Health and Education ....................................................................................................... 17 Australia-Timor Relations .................................................................................................. 21 Appendixes .......................................................................................................................... 23 i) Participants……………………………………………………………………………………23 ii) Participant Reflections ................................................................................................... 24 iii) Study Tour Itinerary with Map ...................................................................................... 28 Bibliography ....................................................................................................................... -
Timor-Leste DHS 2009-10 Fact Sheet
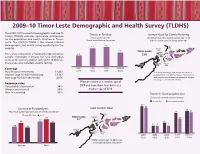
2009–10 Timor-Leste Demographic and Health Survey (TLDHS) The 2009–10 Timor-Leste Demographic and Health Trends in Fertility Unmet Need for Family Planning Survey (TLDHS) provides up-to-date information TFR for women for the Percent of currently married women age 15-49 on the population and health situation in Timor- 3-year period before the survey with an unmet need for family planning* Leste. The 2009–10 TLDHS is the second national demographic and health survey conducted in the 7.4 7.8 Dili 29% country. Liquiçá Lautem 5.7 Timor-Leste 29% Baucau 28% Aileu Manatuto 35% 27% The survey is based on a nationally representative 4.4 31% Ermera 30% Viqueque sample. It provides estimates for rural and urban 23% 31% Bobonaro Manufahi areas of the country and for each of the 13 districts. 42% 22% The survey also included anemia testing. Oecussi Covalima Ainaro 40% 17% 43% Coverage 1997 2002 2003 2009-10 IDHS MICS DHS TLDHS Households interviewed 11,463 *Currently married fecund women who want to Women (age 15–49) interviewed 13,137 postpone their next birth for two or more years or Men (age 15–54) interviewed 4,076 who want to stop childbearing altogether but are not using a contraceptive method Women marry at a median age of Response rates Households interviewed 98% 20.9 and have their first birth at a Women interviewed 95% median age of 22.4. Men interviewed 92% Trends in Contraceptive Use Percent of currently married women Any method Any modern method 27 25 Literacy of Respondents Total Fertility Rate 22 21 Percent of women and men age 15-49 -

East Timor Delegation Report
The Parliament of the Commonwealth of Australia Parliamentary Delegation to East Timor 3 to 5 September 2003 November 2003 Canberra © Commonwealth of Australia 1999 ISBN 0 642 78446 9 Contents Foreword.............................................................................................................................................vi Membership of the Delegation...........................................................................................................viii Acknowledgements .............................................................................................................................ix List of abbreviations ............................................................................................................................ x 1: Introduction ..............................................................................................................1 Objectives and Scope............................................................................................................... 1 East Timor–background information ...................................................................................... 2 Government and politics ............................................................................................................. 2 Economic overview ..................................................................................................................... 4 Australia’s bilateral relations with East Timor............................................................................. -

The Study on Urgent Improvement Project for Water Supply System in East Timor
JAPAN INTERNATIONAL COOPERATION AGENCY EAST TIMOR TRANSITIONAL ADMINISTRATION THE STUDY ON URGENT IMPROVEMENT PROJECT FOR WATER SUPPLY SYSTEM IN EAST TIMOR FINAL REPORT VolumeⅠ: SUMMARY REPORT FEBRUARY 2001 TOKYO ENGINEERING CONSULTANTS, CO., LTD. PACIFIC CONSULTANTS INTERNATIONAL SSS JR 01-040 THE STUDY ON URGENT IMPROVEMENT PROJECT FOR WATER SUPPLY SYSTEM IN EAST TIMOR FINAL REPORT CONSTITUENT VOLUMES VOLUME Ⅰ SUMMARY REPORT VOLUME Ⅱ MAIN REPORT VOLUME Ⅲ APPENDIX VOLUME Ⅳ QUICK PROJECT IMPLEMENTATION MANUAL Foreign Exchange Rate: USD 1.00 = INDONESIA RUPIAH 9,500 AUD 1.00 = JPY 58.50 USD 1.00 = JPY 111.07 (Status as of the 30 November 2000) PREFACE In response to a request from the United Nations Transitional Administration of East Timor, the Government of Japan decided to conduct The Study on Urgent Improvement Project for Water Supply System in East Timor and entrusted the study to the Japan International Cooperation Agency (JICA). JICA selected and dispatched a study team headed by Mr. Kazufumi Momose of Tokyo Engineering Consultants Co., Ltd. in association with Pacific Consultants International to East Timor, twice between February 2000 and February 2001. The team held discussions with the officials concerned of the East Timor Transitional Administration and Asian Development Bank which is a trustee of East Timor Trust Fund and conducted field surveys in the study area. Based on the field surveys, the Study Team conducted further studies and prepared this final report. I hope that this report will contribute to the promotion of this project and to the enhancement of friendly relationship between Japan and East Timor Finally, I wish to express my sincere appreciation to the officials concerned of the East Timor Transitional Administration for their close cooperation extended to the Study. -

Humanitarian Update Timor-Leste
OCHA/UNMITOCHA/UNMITOCHA/UNMIT Integrated Humanitarian Integrated Integrated Humanitarian Coordination Humanitarian Coordination Team Coordination Team Team HUMANITARIAN UPDATE TIMOR-LESTE PERIOD FROM 16 NOVEMBER TO 7 DECEMBER 2007 THIS WEEK’S HUMANITARIAN ASSISTANCE IN A SNAPSHOT: Food distribution: The General Food Distribution November cycle was completed for 64,493 IDP in 51 IDP Camps in Dili and Tibar (Liquica). The De- cember Distribution cycle started on Tuesday 4 De- cember 2007. Shelter: As of December, the Ministry of Social Solidarity (MSS) and SLS teams have distributed 1700 replacement tents to 22 IDP camps in Dili. Visit of the UN Security Council delegation to the Hospital IDP Camp, Dili Friday 30 November 2007 Photo Martine Perret/UNMIT UN SECURITY COUNCIL VISIT: During its trip to Timor-Leste from 26 to 30 November, a delegation of the UN Security Council visited the Hospital IDP camp (see picture). Camp managers from Airport, Jardim, Metinaro Sional IDP camps also participated in the meeting with the Security Council Members. On 29 November, the UN Security Council visited Baucau and held a meeting with the local District Administrator. The Security Council delegation also visited a joint UNICEF/WFP School Programme at Baucau School (No. 01). The delegation was introduced to Active Learning Principles (UNICEF) as well as the WFP School Feeding Programme. The UN Security Council delegation also exchanged with Catholic Relief Services, the Site Liaison Support of the IDP camps in Baucau. RAINY SEASON UPDATE: Food: WFP has effectively propositioned 1,600 MT food commodities for Mother and Child Health (MCH), School Feed- ing (SF), and Food For Work (FFW) programmes in the districts, particularly Covalima, Suai, Ermera, Oecusse and Liquica, in preparation for the rainy season. -
AINARO, V1 Ainaro - TIMOR-LESTE Flood - Situation As of 07/04/2021 Delineation - Overview Map 01
750000 760000 770000 780000 790000 125°16'0"E 125°20'0"E 125°24'0"E 125°28'0"E 125°32'0"E 125°36'0"E GLIDE number: FF-2021-000032-TMP Activation ID: EMSR507 Int. Charter Act. ID: 701 Product N.: 03AINARO, v1 Ainaro - TIMOR-LESTE Flood - Situation as of 07/04/2021 Delineation - Overview map 01 Banda Sea S Ainaro! " 0 ' 0 ° S " 9 0 ' 0 ° 9 Banda Sea Lautem 01 Dili 02 Baucau Manatuto Liquica Aileu Dil^i ViqSauvue Sqeaue Timor-Leste Ermera Bobonaro Ainaro !( Indonesia Timor Sea 04 Manufahi Ainaro 03 Timor Sea Cova Lima 25 0 0 0 0 km 0 0 0 0 0 0 0 0 9 9 Cartographic Information Plan etSco pe (07 /04/20 21 at 1:65000 Full color A1, 200 dpi resolution 01:34 UTC) 0 1.25 2.5 5 km S " Grid: WGS 1984 UTM Zone 51S map coordinate system 0 ' 4 ° S " 9 Tick marks: WGS 84 geographical coordinate system 0 ' 4 ° ± 9 Legend Crisis Information Placenames Facilities Flooded Area ! Placename Construction for mining or extraction (07/04/2021 01:34 UTC) Flood trace Built-Up Area Transportation General Information Built-Up Area Highway Area of Interest Hydrography Primary Road Coastline Image Footprint Local Road River Not Analysed Cart Track Stream Not Analysed - No data Physiography & Land Use - Land Cover ! Administrative boundaries River Features available in the vector package Region Province Consequences within the AOI Unit of measurement Affected Total in AOI Flood trace ha 520.4 Flooded area ha 39.4 Estimated population Number of inhabitants 318 19 976 Built-up Residential Buildings ha 10.5 909.6 Office buildings ha 0.0 0.7 Industrial buildings ha 0.0 -

Timor-Leste Strategic Development Plan, 2011–2030
SDP 2011-2013 PART 1: INTRODUCTION SDP 2011-2013 PART 1: INTRODUCTION TIMOR-LESTE STRATEGIC DEVELOPMENT PLAN 2011 - 2030 VERSION SUBMITTED TO THE NATIONAL PARLIAMENT 1 SDP 2011-2013 PART 1: INTRODUCTION 2 SDP 2011-2013 TIMOR-LESTESDP 2011-2013 STRATEGIC DEVELOPMENT PLAN 2011 - 2030 PART 1: INTRODUCTION PART 1: INTRODUCTION CONTENTS PART 1 INTRODUCTION 7 OVERVIEW 8 BACKGROUND 9 STRATEGIC DEVELOPMENT PLAN 11 PART 2 SOCIAL CAPITAL 13 EDUCATION AND TRAINING 14 HEALTH 33 SOCIAL INCLUSION 44 ENVIRONMENT 53 CULTURE AND HERITAGE 61 PART 3 INFRASTRUCTURE DEVELOPMENT 69 ROADS AND BRIDGES 70 WATER AND SANITATION 77 ELECTRICITY 85 SEA PORTS 93 AIRPORTS 97 TELECOMMUNICATIONS 99 PART 4 ECONOMIC DEVELOPMENT 105 RURAL DEVELOPMENT 107 AGRICULTURE 118 PETROLEUM 136 TOURISM 141 PRIVATE SECTOR INVESTMENT 151 PART 5 INSTITUTIONAL FRAMEWORK 157 SECURITY 158 DEFENCE 163 FOREIGN AFFAIRS 170 JUSTICE 176 PUBLIC SECTOR MANAGEMENT AND GOOD GOVERNANCE 181 NATIONAL DEVELOPMENT AGENCY AND ECONOMIC POLICY AND INVESTMENT AGENCY 188 PART 6 ECONOMIC CONTEXT AND MACROECONOMIC DIRECTION 192 PART 7 CONCLUSION AND STAGING OF THE STRATEGIC DEVELOPMENT PLAN 215 3 TIMOR-LESTESDP 2011-2013 STRATEGIC DEVELOPMENT PLAN 2011 - 2030 PART 1: INTRODUCTION DISTRICT MAP OF TIMOR-LESTE 2011 Source: UNDP 4 SDP 2011-2013 TIMOR-LESTESDP 2011-2013 STRATEGIC DEVELOPMENT PLAN 2011 - 2030 PART 1: INTRODUCTION PART 1: INTRODUCTION LIST OF TABLES TABLE 1 – ESTIMATED SCHOOL INFRASTRUCTURE NEEDS 15 TABLE 2 – PROGRESS ACHIEVED IN BASIC EDUCATION, 2000 TO 2010 17 TABLE 3 – SECONDARY EDUCATION IN TIMOR-LESTE, 2010 20 TABLE 4 – GRADUATED STUDENTS (CUMULATIVE DATA UP TO 2011) 22 TABLE 5 – SUMMARY OF EXISTING HEALTH FACILITIES IN TIMOR-LESTE 34 TABLE 6 – BENEFITS PAID UNDER DECREE-LAW NO.