Common Orthopedic Procedures Which Are Frequently Coded Incorrectly
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Utah Eye Centers Now Offers the Latest Advance in Laser Eye Surgery
Mark G. Ballif, M.D. Scott O. Sykes, M.D. Michael B. Wilcox, M.D. John D. Armstrong, M.D. Robert W. Wing, M.D., FACS Keith Linford, O.D. Jed T. Poll, M.D. Claron D. Alldredge, M.D. Devin B. Farr, O.D. Michael L. Bullard, M.D. Court R. Wilkins, O.D. Utah Eye Centers Now Offers the Latest Advance In Laser Eye Surgery The New VICTUS® Femtosecond Laser Platform, from Bausch + Lomb is Designed to Support Positive Patient Experience and Outstanding Visual Results in Cataract and LASIK Procedures FOR RELEASE April 17, 2015 Ogden, Utah— Utah Eye Centers, the leading comprehensive ophthalmology practice in northern Utah, announced today the Mount Ogden facility now offers eye surgery for cataracts and LASIK with an advanced laser system, the VICTUS® femtosecond laser platform. They are the only practice north of Salt Lake City with a fixed site femtosecond laser for cataracts and LASIK. The versatile VICTUS platform is designed to provide greater precision compared to manual cataract and LASIK surgery techniques. According to Scott Sykes, M.D., the Victus laser is the only laser approved to perform treatments for both cataract and LASIK surgeries. "With the VICTUS platform, we are able to automate some of the steps that we have commonly performed manually," said Mark Ballif, M.D. "While we have performed thousands of successful cataract and LASIK surgeries, the VICTUS platform helps us to improve the procedures to give our patients the best outcomes possible." The VICTUS platform features a sophisticated, curved patient interface with computer-monitored pressure sensors designed to provide comfort during the procedure. -

Effectiveness of Distal Tibial Osteotomy
Nozaka et al. BMC Musculoskeletal Disorders (2020) 21:31 https://doi.org/10.1186/s12891-020-3061-7 RESEARCH ARTICLE Open Access Effectiveness of distal tibial osteotomy with distraction arthroplasty in varus ankle osteoarthritis Koji Nozaka* , Naohisa Miyakoshi, Takeshi Kashiwagura, Yuji Kasukawa, Hidetomo Saito, Hiroaki Kijima, Shuichi Chida, Hiroyuki Tsuchie and Yoichi Shimada Abstract Background: In highly active older individuals, end-stage ankle osteoarthritis has traditionally been treated using tibiotalar arthrodesis, which provides considerable pain relief. However, there is a loss of ankle joint movement and a risk of future arthrosis in the adjacent joints. Distraction arthroplasty is a simple method that allows joint cartilage repair; however, the results are currently mixed, with some reports showing improved pain scores and others showing no improvement. Distal tibial osteotomy (DTO) without fibular osteotomy is a type of joint preservation surgery that has garnered attention in recent years. However, to our knowledge, there are no reports on DTO with joint distraction using a circular external fixator. Therefore, the purpose of this study was to examine the effect of DTO with joint distraction using a circular external fixator for treating ankle osteoarthritis. Methods: A total of 21 patients with medial ankle arthritis were examined. Arthroscopic synovectomy and a microfracture procedure were performed, followed by angled osteotomy and correction of the distal tibia; the ankle joint was then stabilized after its condition improved. An external fixator was used in all patients, and joint distraction of approximately 5.8 mm was performed. All patients were allowed full weight-bearing walking immediately after surgery. Results: The anteroposterior and lateral mortise angle during weight-bearing, talar tilt angle, and anterior translation of the talus on ankle stress radiography were improved significantly (P < 0.05). -

Nd:YAG CAPS ULOTOMY AS a PRIMARY TREATMENT
PSEUDOPHAKIC MALIGNANT GLAUCOMA: Nd:YAG CAPS ULOTOMY AS A PRIMARY TREATMENT B. C. LITTLE and R. A. HITCHINGS London SUMMARY anisms of ciliolenticular block of aqueous flow leading to Malignant glaucoma is one of the most serious but rare the misdirection of aqueous posteriorly into or in front of complications of anterior segment surgery. It is best the vitreous gel leading to the characteristic diffuse shal known following trabeculectomy but has been reported lowing of the anterior chamber accompanied by a precipi following a wide variety of anterior segment procedures tous rise in intraocular pressure. The mechanistic including extracapsular cataract extraction with pos understanding of its pathogenesis has led to the use of the terior chamber lens implantation. It is notoriously refrac synonyms 'ciliolenticular block',7 'ciliovitreal block', tory to medical treatment alone and surgical intervention 'iridovitreal block',8 'aqueous misdirection' and 'aqueous has had only limited success. An additional treatment diversion syndrome'. Although probably more precise option in pseudophakic eyes is that of peripheral these are unlikely to succeed the original term 'malignant Nd:YAG posterior capsulotomy, which is minimally glaucoma', which more accurately evokes the fulminant invasive and can re-establish forward flow of posteriorly nature of the condition as well as the justified anxiety asso misdirected aqueous through into the drainage angle of ciated with it. Medical treatment alone is rarely successful the anterior chamber. We report our experience of seven in establishing control of the intraocular pressure.2•8 Pars cases of malignant glaucoma in pseudophakic eyes and of plana vitrectomy has been used in the surgical managment the successful use of Nd:YAG posterior capsulotomy in of malignant glaucoma with some definite but limited suc re-establishing pressure control in' five of these eyes, cess in phakic as well as pseudophakic eyes.9•10 thereby obviating the need for acute surgical However, when malignant glaucoma develops in intervention. -

Outcome of Lens Aspiration and Intraocular Lens Implantation in Children Aged 5 Years and Under
540 Br J Ophthalmol 2001;85:540–542 Outcome of lens aspiration and intraocular lens implantation in children aged 5 years and under Lorraine Cassidy, Jugnoo Rahi, Ken Nischal, Isabelle Russell-Eggitt, David Taylor Abstract However, final refraction is variable, such that Aims—To determine the visual outcome emmetropia in adulthood cannot be guaran- and complications of lens aspiration with teed, as there are insuYcient long term studies. intraocular lens implantation in children There have been many reports of the visual aged 5 years and under. outcome and complications of posterior cham- Methods—The hospital notes of all chil- ber lens implantation in children.4–12 Most of dren aged 5 years and under, who had these have been based on older children, undergone lens aspiration with intraocu- secondary lens implants, a high number of lar lens implantation between January traumatic cataracts, and many have reported 1994 and September 1998, and for whom early outcome. We report visual outcome and follow up data of at least 1 year were avail- complications of primary IOL implantation at able, were reviewed. least 1 year after surgery, in children aged 5 Results—Of 50 children who underwent years and under, with mainly congenital or surgery, 45 were eligible based on the juvenile lens opacities. follow up criteria. 34 children had bilat- eral cataracts and, of these, 30 had surgery Methods on both eyes. Cataract was unilateral in 11 SUBJECTS cases; thus, 75 eyes of 45 children had sur- We reviewed the notes of all children aged 5 gery. Cataracts were congenital in 28 years and under, who had undergone lens aspi- cases, juvenile in 16, and traumatic in one ration with primary posterior chamber in- case. -

Laser Learning Lecture and Lab: YAG Caps, LPI, And
5/9/17 Overview Laser Learning Lecture and Lab: • Why we use lasers YAG caps, LPI, and SLT • YAG capsulotomy • Laser Peripheral Iridotomy (LPI or PI) Aaron McNulty, O.D., F.A.A.O. • Argon Laser Peripheral Iridoplasty (ALPI) Nate Lighthizer, O.D., F.A.A.O. • Argon Laser Trabeculoplasty (ALT) • Selective Laser Trabeculoplasty (SLT) • Other Laser Trabeculoplasty Why do we use lasers? Posterior Capsular Opacification (PCO) • Vision is decreased from PCO following cataract surgery • Lens capsular bag has an anterior and • Narrow angles/angle closure posterior surface • Glaucoma is progressing in a pt on max meds – Anterior surface usually removed w/ capsulorhexis – Something else needs to be done – Surgery not wanted yet • PCO is the formation of a cloudy membrane • Compliance issues on the posterior surface of the capsular bag • Cost issues following ECCE • Convenience issues – AKA: Secondary cataract • Doctor preference PCO YAG Laser • Incidence: • Nd: YAG laser – Most common complication of post ECCE – Neodymium: Yttrium aluminum garnet laser – 10-80% of eyes following cataract surgery – Can form anywhere from a few days to years post surgery • Tissue interaction: Photodisruptive laser – Younger patients higher risk of PCO – High light energy levels cause the tissues to be reduced – IOL’s to plasma, disintegrating the tissue • Silicone > acrylic – A large amount of energy is delivered into very small focal spots in a very brief duration of time • Prevention: • 4 nsec – – Capsulotomy during surgery No thermal reaction/No coagulation when bv’s are hit – Posterior capsular polishing – Pigment independent* 1 5/9/17 YAG Cap Risks, Complications, YAG Cap Pre-op Exam Contraindications • Visual acuity, glare testing, PAM/Heine lambda Contraindications Risks/complications – Vision 20/30 or worse 1. -
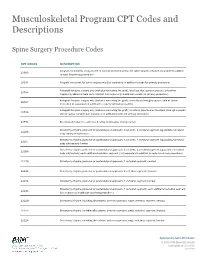
Musculoskeletal Program CPT Codes and Descriptions
Musculoskeletal Program CPT Codes and Descriptions Spine Surgery Procedure Codes CPT CODES DESCRIPTION Allograft, morselized, or placement of osteopromotive material, for spine surgery only (List separately in addition 20930 to code for primary procedure) 20931 Allograft, structural, for spine surgery only (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); local (eg, ribs, spinous process, or laminar 20936 fragments) obtained from same incision (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); morselized (through separate skin or fascial 20937 incision) (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); structural, bicortical or tricortical (through separate 20938 skin or fascial incision) (List separately in addition to code for primary procedure) 20974 Electrical stimulation to aid bone healing; noninvasive (nonoperative) Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22206 body subtraction); thoracic Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22207 body subtraction); lumbar Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22208 body subtraction); each additional vertebral segment (List separately in addition to code for -

Priority Health Spine and Joint Code List
Priority Health Joint Services Code List Category CPT® Code CPT® Code Description Joint Services 23000 Removal of subdeltoid calcareous deposits, open Joint Services 23020 Capsular contracture release (eg, Sever type procedure) Joint Services 23120 Claviculectomy; partial Joint Services 23130 Acromioplasty or acromionectomy, partial, with or without coracoacromial ligament release Joint Services 23410 Repair of ruptured musculotendinous cuff (eg, rotator cuff) open; acute Joint Services 23412 Repair of ruptured musculotendinous cuff (eg, rotator cuff) open;chronic Joint Services 23415 Coracoacromial ligament release, with or without acromioplasty Joint Services 23420 Reconstruction of complete shoulder (rotator) cuff avulsion, chronic (includes acromioplasty) Joint Services 23430 Tenodesis of long tendon of biceps Joint Services 23440 Resection or transplantation of long tendon of biceps Joint Services 23450 Capsulorrhaphy, anterior; Putti-Platt procedure or Magnuson type operation Joint Services 23455 Capsulorrhaphy, anterior;with labral repair (eg, Bankart procedure) Joint Services 23460 Capsulorrhaphy, anterior, any type; with bone block Joint Services 23462 Capsulorrhaphy, anterior, any type;with coracoid process transfer Joint Services 23465 Capsulorrhaphy, glenohumeral joint, posterior, with or without bone block Joint Services 23466 Capsulorrhaphy, glenohumeral joint, any type multi-directional instability Joint Services 23470 ARTHROPLASTY, GLENOHUMERAL JOINT; HEMIARTHROPLASTY ARTHROPLASTY, GLENOHUMERAL JOINT; TOTAL SHOULDER [GLENOID -

Diagnosis and Treatment of Neurotrophic Keratopathy
An Evidence-based Approach to the Diagnosis and Treatment of Neurotrophic Keratopathy ACTIVITY DIRECTOR A CME MONOGRAPH Esen K. Akpek, MD This monograph was published by Johns Hopkins School of Medicine in partnership Wilmer Eye Institute with Catalyst Medical Education, LLC. It is Johns Hopkins School of Medicine not affiliated with JAMA medical research Baltimore, Maryland publishing. Visit catalystmeded.com/NK for online testing to earn your CME credit. FACULTY Natalie Afshari, MD Mina Massaro-Giordano, MD Shiley Eye Institute University of Pennsylvania School of Medicine University of California, San Diego Philadelphia, Pennsylvania La Jolla, California Nakul Shekhawat, MD, MPH Sumayya Ahmad, MD Wilmer Eye Institute Mount Sinai School of Medicine Johns Hopkins School of Medicine New York, New York Baltimore, Maryland Pedram Hamrah, MD, FRCS, FARVO Christopher E. Starr, MD Tufts University School of Medicine Weill Cornell Medical College Boston, Massachusetts New York, New York ACTIVITY DIRECTOR FACULTY Esen K. Akpek, MD Natalie Afshari, MD Mina Massaro-Giordano, MD Professor of Ophthalmology Professor of Ophthalmology Professor of Clinical Ophthalmology Director, Ocular Surface Diseases Chief of Cornea and Refractive Surgery University of Pennsylvania School and Dry Eye Clinic Vice Chair of Education of Medicine Wilmer Eye Institute Fellowship Program Director of Cornea Philadelphia, Pennsylvania Johns Hopkins School of Medicine and Refractive Surgery Baltimore, Maryland Shiley Eye Institute Nakul Shekhawat, MD, MPH University of California, -

Knee Joint Surgery: Open Synovectomy
Musculoskeletal Surgical Services: Open Surgical Procedures; Knee Joint Surgery: Open Synovectomy POLICY INITIATED: 06/30/2019 MOST RECENT REVIEW: 06/30/2019 POLICY # HH-5588 Overview Statement The purpose of these clinical guidelines is to assist healthcare professionals in selecting the medical service that may be appropriate and supported by evidence to improve patient outcomes. These clinical guidelines neither preempt clinical judgment of trained professionals nor advise anyone on how to practice medicine. The healthcare professionals are responsible for all clinical decisions based on their assessment. These clinical guidelines do not provide authorization, certification, explanation of benefits, or guarantee of payment, nor do they substitute for, or constitute, medical advice. Federal and State law, as well as member benefit contract language, including definitions and specific contract provisions/exclusions, take precedence over clinical guidelines and must be considered first when determining eligibility for coverage. All final determinations on coverage and payment are the responsibility of the health plan. Nothing contained within this document can be interpreted to mean otherwise. Medical information is constantly evolving, and HealthHelp reserves the right to review and update these clinical guidelines periodically. No part of this publication may be reproduced, stored in a retrieval system or transmitted, in any form or by any means, electronic, mechanical, photocopying, or otherwise, without permission from HealthHelp. -

Endoscopic Vitreoretinal Surgery: Principles, Applications and New Directions Radwan S
Ajlan et al. Int J Retin Vitr (2019) 5:15 International Journal https://doi.org/10.1186/s40942-019-0165-z of Retina and Vitreous REVIEW Open Access Endoscopic vitreoretinal surgery: principles, applications and new directions Radwan S. Ajlan1*, Aarsh A. Desai2 and Martin A. Mainster1 Abstract Purpose: To analyze endoscopic vitreoretinal surgery principles, applications, challenges and potential technological advances. Background: Microendoscopic imaging permits vitreoretinal surgery for tissues that are not visible using operat- ing microscopy ophthalmoscopy. Evolving instrumentation may overcome some limitations of current endoscopic technology. Analysis: Transfer of the fine detail in endoscopic vitreoretinal images to extraocular video cameras is constrained currently by the caliber limitations of intraocular probes in ophthalmic surgery. Gradient index and Hopkins rod lenses provide high resolution ophthalmoscopy but restrict surgical manipulation. Fiberoptic coherent image guides offer surgical maneuverability but reduce imaging resolution. Coaxial endoscopic illumination can highlight delicate vitreo- retinal structures difficult to image in chandelier or endoilluminator diffuse, side-scattered lighting. Microendoscopy’s ultra-high magnification video monitor images can reveal microscopic tissue details blurred partly by ocular media aberrations in contemporary surgical microscope ophthalmoscopy, thereby providing a lower resolution, invasive alternative to confocal fundus imaging. Endoscopic surgery is particularly useful when ocular -

(YAG) Laser Capsulotomy Reference Number: CP.VP.65 Coding Implications Last Review Date: 12/2020 Revision Log
Clinical Policy: Yttrium Aluminium Garnet (YAG) Laser Capsulotomy Reference Number: CP.VP.65 Coding Implications Last Review Date: 12/2020 Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description This policy describes the medical necessity requirements for yttrium aluminium garnet (YAG) laser capsulotomy. Policy/Criteria I. It is the policy of health plans affiliated with Centene Corporation® (Centene) that YAG laser capsulotomy is medically necessary for the following indications: A. Posterior capsular opacification following cataract surgery resulting in best corrected visual acuity of 20/30 or worse associated with symptoms of blurred vision, visual distortion or glare affecting activities of daily living; B. Contraction of the posterior capsule with resulting displacement of the intraocular lens; C. Posterior capsular opacification resulting in best corrected visual acuity of 20/25 or worse, reducing the ability to evaluate and treat retinal detachment. Background YAG capsulotomy is the incision of an opaque posterior lens capsule in an aphakic or pseudophakic eye. This incision allows the capsule to retract and no longer serve as an obstruction to the passage of light through the media to the retina. The incision is performed with YAG laser. The eye examination must confirm the diagnosis of posterior capsular opacification and excludes other ocular causes of functional impairment by one of the following methods: The eye examination should demonstrate decreased light transmission (visual acuity worse than 20/30 or 20/25 if the procedure is performed to assist in the diagnosis and treatment of retinal detachment). Manifest refraction must be recorded with decrease in best-corrected visual acuity. -

Radiation Synovectomy with 166Ho-Ferric Hydroxide: a First Experience
Radiation Synovectomy with 166Ho-Ferric Hydroxide: A First Experience Sedat Ofluoglu, MD1; Eva Schwameis, MD2; Harald Zehetgruber, MD2; Ernst Havlik, PhD3; Axel Wanivenhaus, MD2; Ingrid Schweeger, MD1; Konrad Weiss, MD4; Helmut Sinzinger, MD1; and Christian Pirich, MD1 1Department of Nuclear Medicine, University of Vienna, Vienna, Austria; 2Department of Orthopedics, University of Vienna, Vienna, Austria; 3Department of Biomedical Engineering and Physics and Ludwig Boltzmann Institute of Nuclear Medicine, Vienna, Austria; and 4Department of Nuclear Medicine, General Hospital of Wiener Neustadt, Wiener Neustadt, Austria lage, leading to the progressive loss of joint function and Radiation synovectomy (RS) is indicated when conventional significant disability. Treatment of chronic synovitis using pharmacologic treatment of chronic synovitis has not relieved radiation synovectomy (RS) aims to stop the inflammatory its symptoms. The use of radionuclides that are bound to ferric process causing pain, disability, and nonreversible structural hydroxide (FH) particles has been shown to be effective and damage to the joint (1–3). RS has been in clinical use for 166 safe for this procedure. Ho-FH macroaggregates offer prom- 50y(4) primarily as an alternative to surgical treatment (5). ising properties for RS but there is a lack of clinical data. We Safety is one of the most important aspects when radionu- investigated the efficacy and safety of 166Ho-FH in a prospective clinical trial in patients suffering from chronic synovitis. Meth- clides are applied therapeutically. The use of ferric hydrox- ods: Twenty-four intraarticular injections were performed in 22 ide (FH) particles as a carrier may offer some advantages patients receiving a mean activity of 1.11 GBq (range, 0.77–1.24 over other carriers with respect to the frequency and degree GBq) 166Ho-FH.