Endoscopic Vitreoretinal Surgery: Principles, Applications and New Directions Radwan S
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Wildlife Ophthalmology
Wildlife Ophthalmology DR. HEATHER REID TORONTO WILDLIFE CENTRE TORONTO, ON CANADA Why understand eyes? Wildlife need to have excellent vision to survive in the wild Eye related problems are common in wildlife admitted to rehabilitation centers What we will cover Anatomy of the eye Differences between birds and mammals The eye exam Recognizing common problems Prognosis Treatment options When to see the vet Anatomy Around the Eye: Muscles & nerves Skin Eye lids Nictitating eyelid Conjunctiva & sclera Tear glands & ducts Ossicles (birds) Anatomy Front of the Eye: Cornea Iris Pupil Ciliary body Anterior Chamber Aqueous humor Anatomy Back of the Eye: Lens Retina Optic nerve Choroid Pecten (birds) Posterior Chamber Vitreous humor Fundus of the Eye Mammal Eye Bird Eye The Avian Eye - Differences Small eye size in most birds and small pupil size makes it hard to examine Can control the size of their pupil Lower eyelid more developed The nictitating membrane spreads the tears allowing birds to blink less Moves horizontally across eye The Avian Eye - Differences Eyes are not as protected by skull Less muscles around eye so less eye movement Boney ossicles support the eye Three main eye shapes; flat, globose & tubular The Avian Eye - Differences Four different color receptors compared to the three in mammals means better color detail Can see in the ultraviolet range Higher flicker rate – can detect lights that flicker at more than 100 flashes per second (humans detect at 50) The Avian Eye - Differences In some species the eye -

Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing As Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease
Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing as Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease BRIAN C. TOY, MD,*† DAVID J. MYUNG, MD, PHD,*† LINGMIN HE, MD,*† CAROLYN K. PAN, MD,*† ROBERT T. CHANG, MD,* ALISON POLKINHORNE, MA,‡ DOUGLAS MERRELL, BS,‡ DOUG FOSTER, MBA,‡ MARK S. BLUMENKRANZ, MD* Purpose: To compare clinical assessment of diabetic eye disease by standard dilated examination with data gathered using a smartphone-based store-and-forward teleoph- thalmology platform. Methods: 100 eyes of 50 adult patients with diabetes from a health care safety-net ophthalmology clinic. All patients underwent comprehensive ophthalmic examination. Concurrently, a smartphone was used to estimate near visual acuity and capture anterior and dilated posterior segment photographs, which underwent masked, standardized review. Quantitative comparison of clinic and smartphone-based data using descriptive, kappa, Bland-Altman, and receiver operating characteristic analyses was performed. Results: Smartphone visual acuity was successfully measured in all eyes. Anterior and posterior segment photography was of sufficient quality to grade in 96 and 98 eyes, respectively. There was good correlation between clinical Snellen and smartphone visual acuity measurements (rho = 0.91). Smartphone-acquired fundus photographs demon- strated 91% sensitivity and 99% specificity to detect moderate nonproliferative and worse diabetic retinopathy, with good agreement between clinic and photograph grades (kappa = 0.91 ± 0.1, P , 0.001; AUROC = 0.97, 95% confidence interval, 0.93–1). Conclusion: The authors report a smartphone-based telemedicine system that demon- strated sensitivity and specificity to detect referral-warranted diabetic eye disease as a proof-of-concept. Additional studies are warranted to evaluate this approach to expanding screening for diabetic retinopathy. -

Effects of Nd:YAG Laser Capsulotomy in Posterior Capsular Opacification
Original Research Article Effects of Nd:YAG laser capsulotomy in posterior capsular opacification Praveen Kumar G S1, Lavanya P2*, Raviprakash D3 1Assistant Professor, 2Associate Professor, 3Professor & HOD, Department of Ophthalmology, Shridevi institute of Medical Sciences and Research Hospital, Sira Road, NH-4 Bypass Road, Tumkur- 572106, INDIA. Email: [email protected] Abstract Background: Posterior capsular opacification (PCO) is the most common long-term complication of cataract surgery in both phacoemulsification and extracapsular cataract extraction (ECCE). The overall incidence of PCO and the incidence of neodymium-doped yttrium–aluminum–garnet (Nd:YAG) laser posterior capsulotomy has decreased from 50% in the 1980s and early 1990s to less than 10% today. Reported complications of Nd:YAG laser posterior capsulotomy include elevated intraocular pressure, iritis, corneal damage, intraocular lens (IOL) damage, cystoids macular edema, disruption of the anterior hyaloid surface, increased risk of retinal detachment, and IOL movement or dislocation. In some patients, a refraction change is noticed after Nd:YAG laser posterior capsulotomy, but proving this remains difficult. Materials and Methods: Nd; YAG LASER capsulotomy was performed in 200 eyes of 200 patients, some with pseudophakia and some with aphakia at Kurnool medical college, Kurnool. They were followed up between October 2008 and September 2010. Results: Elevation of IOP has been well documented after anterior segment laser procedures. The IOP rise after YAG laser posterior capsulotomy is of short duration starting about 1 hr after laser procedure and lasting for 24 hrs. In this study, in 1case IOP came down to normal level after 3 days and in another case after 7 days. -

Coding Competencies for Ophthalmic Techs – 2020 Coding Update
3/5/2020 Coding Competencies for Ophthalmic Techs – 2020 Coding Update OAO Ophthalmic Medical Technology Friday, March 13, 2020 Joy Woodke, COE, OCS, OCSR 1 Financial Disclosure Joy Woodke, COE, OCS o This presenter does not have a financial interest or relationship to disclose relative to this activity. o Academy Coding & Practice Management Executive 2 Topics 2020 Coding Updates Coding Competencies Diagnostic testing services Modifiers Tech Takeaways Understanding insurance policies Ongoing coding education Resources 3 1 3/5/2020 2020 Coding Updates Extended Ophthalmoscopy & Cataract Surgery 4 Extended Ophthalmoscopy (EO) • CPT eliminated initial and subsequent codes for EO • New codes for drawing of • Peripheral retina, with scleral depression: 5% in work value over deleted initial EO • Optic nerve or macula: 32% compared to deleted initial EO 5 Extended Ophthalmoscopy (EO) • 92225 Ophthalmoscopy, extended, with retinal drawing (eg, for retinal detachment, melanoma), with interpretation and report; initial • 92226 subsequent 6 2 3/5/2020 Extended Ophthalmoscopy (EO) 92201 Ophthalmoscopy, extended; with retinal drawing and scleral depression of peripheral retinal disease (eg, for retinal tear, retinal detachment, retinal tumor) with interpretation and report, unilateral or bilateral 7 Ophthalmoscopy 92201 8 8 Extended Ophthalmoscopy (EO) 92202 with drawing of optic nerve or macula (eg, for glaucoma, macular pathology, tumor) with interpretation and report, unilateral or bilateral 9 3 3/5/2020 Ophthalmoscopy 92202 10 Extended Ophthalmoscopy (EO) • Payment was unilateral. 2020 is bilateral. 2019 2020 92225 $29.87 per eye 92201 $27.21 Only bill for the eye that has 92202 $17.21 pathology. 92226 $27.63 per eye Only bill for the eye that has pathology 11 Extended Ophthalmoscopy (EO) • Payment is the same whether one or both eyes are examined and pathology is drawn and labeled. -

Diagnosis and Treatment of Neurotrophic Keratopathy
An Evidence-based Approach to the Diagnosis and Treatment of Neurotrophic Keratopathy ACTIVITY DIRECTOR A CME MONOGRAPH Esen K. Akpek, MD This monograph was published by Johns Hopkins School of Medicine in partnership Wilmer Eye Institute with Catalyst Medical Education, LLC. It is Johns Hopkins School of Medicine not affiliated with JAMA medical research Baltimore, Maryland publishing. Visit catalystmeded.com/NK for online testing to earn your CME credit. FACULTY Natalie Afshari, MD Mina Massaro-Giordano, MD Shiley Eye Institute University of Pennsylvania School of Medicine University of California, San Diego Philadelphia, Pennsylvania La Jolla, California Nakul Shekhawat, MD, MPH Sumayya Ahmad, MD Wilmer Eye Institute Mount Sinai School of Medicine Johns Hopkins School of Medicine New York, New York Baltimore, Maryland Pedram Hamrah, MD, FRCS, FARVO Christopher E. Starr, MD Tufts University School of Medicine Weill Cornell Medical College Boston, Massachusetts New York, New York ACTIVITY DIRECTOR FACULTY Esen K. Akpek, MD Natalie Afshari, MD Mina Massaro-Giordano, MD Professor of Ophthalmology Professor of Ophthalmology Professor of Clinical Ophthalmology Director, Ocular Surface Diseases Chief of Cornea and Refractive Surgery University of Pennsylvania School and Dry Eye Clinic Vice Chair of Education of Medicine Wilmer Eye Institute Fellowship Program Director of Cornea Philadelphia, Pennsylvania Johns Hopkins School of Medicine and Refractive Surgery Baltimore, Maryland Shiley Eye Institute Nakul Shekhawat, MD, MPH University of California, -

2Nd Quarter 2001 Medicare Part a Bulletin
In This Issue... From the Intermediary Medical Director Medical Review Progressive Corrective Action ......................................................................... 3 General Information Medical Review Process Revision to Medical Record Requests ................................................ 5 General Coverage New CLIA Waived Tests ............................................................................................................. 8 Outpatient Hospital Services Correction to the Outpatient Services Fee Schedule ................................................................. 9 Skilled Nursing Facility Services Fee Schedule and Consolidated Billing for Skilled Nursing Facility (SNF) Services ............. 12 Fraud and Abuse Justice Recovers Record $1.5 Billion in Fraud Payments - Highest Ever for One Year Period ........................................................................................... 20 Bulletin Medical Policies Use of the American Medical Association’s (AMA’s) Current Procedural Terminology (CPT) Codes on Contractors’ Web Sites ................................................................................. 21 Outpatient Prospective Payment System January 2001 Update: Coding Information for Hospital Outpatient Prospective Payment System (OPPS) ......................................................................................................................... 93 he Medicare A Bulletin Providers Will Be Asked to Register Tshould be shared with all to Receive Medicare Bulletins and health care -

Visual Outcome of Pars Plana Vitrectomy Following Endophthalmitis – a Vitreo-Retinal Surgeon's Experience
Medical Journal of Zambia, Vol. 47 (1): 33 - 38 (2020) Original Article Visual outcome of Pars Plana Vitrectomy following Endophthalmitis – A Vitreo-retinal Surgeon's Experience Sanjoy K. Das1 ,Osayem J. Otabor-Olubor2, Situma P Wanyama1 1Ispahani Islamia Eye Institute and Hospital (IIEIH), Dhaka, Bangladesh 2Ispahani Islamia Eye Institute and Hospital (IIEIH), Dhaka, Bangladesh1 and University of Benin Teaching Hospital (UBTH), Benin City, Nigeria. ABSTRACT (p-value = 0.007). There was an association (although not strong) between age range and post- Purpose: To determine the visual outcome of pars operative visual improvement (p-value = 0.639). plana vitrectomy following endophthalmitis. Conclusion: Pars plana vitrectomy helps to prevent Methods: A retrospective hospital-based study of 20 or minimize ophthalmic complications from eyes of consecutive patients who had pars plana endophthalmitis, thus making it a necessary line of vitrectomy by a particular surgeon following treatment endophthalmitis. Pars plana vitrectomy is endophthalmitis in the Ispahani Islamia Eye therefore a safe and desirable definitive treatment Institute and Hospital, Dhaka, Bangladesh from for endophthalmitis, and it confers a good chance of August – December 2017. Using the Snellen's visual visual improvement. acuity chart, post-operative distant visual acuity improvement was graded 0– 9, with 0 meaning no INTRODUCTION improvement in visual acuity, and 9 meaning nine Pars plana vitrectomy (the intricate surgical removal lines of improvement in visual acuity from of vitreous gel from the vitreous cavity) has seen presenting best corrected visual acuity. remarkable progress in surgical technique and post- Results: Pre-operative corrected distant visual operative outcome in ophthalmic practices all over acuity (CDVA) ranged from perception of light to the world. -
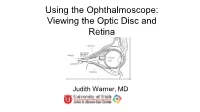
Using the Ophthalmoscope: Viewing the Optic Disc and Retina
Using the Ophthalmoscope: Viewing the Optic Disc and Retina Judith Warner, MD University of Utah THE OPHTHALMOSCOPE DIRECT OPHTHALMOSCOPY • Jan Purkinje 1823 • Hermann von Helmholtz 1851 • Hand held ophthalmoscope • Direct up-right image Dials of the Ophthalmoscope RED-FREE FILTER (GREEN LIGHT) 450 nm monochromatic light nerve fiber layer optic nerve drusen OTHER DIALS • Used for measuring lesion size • Looking for the center of fixation OTHER DIALS: SLIT BEAM The wheel has lenses of power Panoptic-ophthalmoscope Direct type Wider field of view Distance from pt greater Similar apertures Not as easy to carry Slightly dimmer light source Not as magnified view of Disc Clean the rubber cup between patients Photographs: http://panoptic.welchallyn.com/faq.html WHEN EVER POSSIBLE: DILATE THE PATIENT Steps to Direct Ophthalmoscopy • Dimly lit room • Dilating drops • Patient fixates distant target • Align yourself • Red reflex • Dial in HOW TO USE THE DIRECT Ophthalmoscope.avi ophthalmoscope.wmv THE RED REFLEX The layers you will go through to see the optic disc THE OPTIC NERVE WHAT YOU SHOULD OBSERVE IN EVERYONE RIGHT EYE AND LEFT EYE THE NORMAL DISC • The disc is 1.62 mm or 1 million fibers • Central retinal artery and vein • Lamina Cribrosa • The optic cup The Normal Disc Appearance The lamina cribrosa is an important disc structure --Means Sieve --Anatomically present in all discs --Visible in about 1/3 --Shallow in myopia Look at the Cup-to-disc ratio: WHAT IS THE CUP-TO-DISC RATIO? .7 NO CUP 0.1 CUP 0.3 CUP 0.7 CUP 0.9 CUP What is the cup -
The Capsulotomy: from There to Where?
JUNE 2017 # 42 In My View NextGen Profession Sitting Down With Presbyopia correction in Dry eye: how the humble Louis Pasquale believes it’s Innovator extraordinaire, younger patients – what’s best? eyedrop is evolving time to redefine POAG Sean Ianchulev 17 36 – 38 42 – 45 50 – 51 The Capsulotomy: From There to Where? A tale of jealousy, rivalry and pride… The unfolding story of the capsulotomy over time 18 – 27 www.theophthalmologist.com It’s all in CHOOSE A SYSTEM THAT EMPOWERS YOUR EVERY MOVE. Technique is more than just the motions. Purposefully engineered for exceptional versatility and high-quality performance, the WHITESTAR SIGNATURE PRO Phacoemulsification System gives you the clinical flexibility, confidence and control to free your focus for what matters most in each procedure. How do you phaco? Join the conversation. Contact your Phaco Specialist today. Rx Only INDICATIONS: The WHITESTAR SIGNATURE PRO System is a modular ophthalmic microsurgical system that facilitates anterior segment (cataract) surgery. The modular design allows the users to configure the system to meet their surgical requirements. IMPORTANT SAFETY INFORMATION: Risks and complications of cataract surgery may include broken ocular capsule or corneal burn. This device is only to be used by a trained, licensed physician. ATTENTION: Reference the labeling for a complete listing of Indications and Important Safety Information. WHITESTAR SIGNATURE is a trademark owned by or licensed to Abbott Laboratories, its subsidiaries or affiliates. © 2017 Abbott Medical Optics Inc. | PP2017CT0929 Image of the Month In a Micropig’s Eye This Wellcome Image Award winner depicts a 3D model of a healthy mini-pig eye. -

Visual Field Changes After Vitrectomy with Internal Limiting Membrane Peeling for Epiretinal Membrane Or Macular Hole in Glaucomatous Eyes
RESEARCH ARTICLE Visual field changes after vitrectomy with internal limiting membrane peeling for epiretinal membrane or macular hole in glaucomatous eyes Shunsuke Tsuchiya, Tomomi Higashide*, Kazuhisa Sugiyama Department of Ophthalmology, Kanazawa University Graduate School of Medical Science, Kanazawa, Japan * [email protected] a1111111111 a1111111111 a1111111111 Abstract a1111111111 a1111111111 Purpose To investigate visual field changes after vitrectomy for macular diseases in glaucomatous eyes. OPEN ACCESS Citation: Tsuchiya S, Higashide T, Sugiyama K Methods (2017) Visual field changes after vitrectomy with internal limiting membrane peeling for epiretinal A retrospective review of 54 eyes from 54 patients with glaucoma, who underwent vitrectomy membrane or macular hole in glaucomatous eyes. for epiretinal membrane (ERM; 42 eyes) or macular hole (MH; 12 eyes). Standard automated PLoS ONE 12(5): e0177526. https://doi.org/ perimetry (Humphrey visual field 24±2 program) was performed and analyzed preoperatively 10.1371/journal.pone.0177526 and twice postoperatively (1st and 2nd sessions; 4.7 ± 2.5, 10.3 ± 3.7 months after surgery, Editor: Demetrios G. Vavvas, Massachusetts Eye & respectively). Postoperative visual field sensitivity at each test point was compared with the Ear Infirmary, Harvard Medical School, UNITED STATES preoperative value. Longitudinal changes in mean visual field sensitivity (MVFS) of the 12 test points within 10Ê eccentricity (center) and the remaining test points (periphery), best-cor- Received: October 29, 2016 rected visual acuity (BCVA), intraocular pressure (IOP), and ganglion cell complex (GCC) Accepted: April 29, 2017 thickness, and the association of factors with changes in central or peripheral MVFS over Published: May 18, 2017 time were analyzed using linear mixed-effects models. -

Comprehensive Strategies for Unplanned Vitrectomy for the Anterior Segment Surgeon
Supplement to January 2012 When the Room Gets Quiet Comprehensive strategies for unplanned vitrectomy for the anterior segment surgeon. A monograph and DVD based on the live surgery course given by Lisa B. Arbisser, MD. PLUS: A DVD OF SURGICAL VIDEOS AND A DIGITAL VERSION AVAILABLE AT EYETUBE.NET When the Room Gets Quiet An Ounce of Prevention All ophthalmic surgeons must have a comprehensive strategy for managing surgical complications. Many opinions and recommendations exist for handling complicated cataract surgeries. This monograph contains mine. I was trained as a comprehensive ophthalmologist, and for many years I performed scleral buckles, tra- beculectomy, and penetrating keratoplasty before con- centrating on cataract surgery and anterior segment reconstruction. The strategies I have developed for man- aging complex and complicated cataracts over decades of practice are enhanced by close collaboration with retinal surgeons as well as laboratory exploration. I hope this information will help you to organize your thoughts and have a cogent strategy at hand for ‘when the room gets quiet.’ An unplanned vitrectomy. —Lisa B. Arbisser, MD To view a digital version of this monograph with the videos from the accompanying DVD as well as additional materials, visit http://www.Eyetube.net/unplanned-vitrectomy. Table of Contents 3 Preoperative Evaluation of Problematic Eyes 11 Rationale for a Pars Plana Incision 3 Preventing Complications 12 Vitrectomy Goals and Parameters 5 Early Stages of Complications 13 Getting Started 6 Stages of Complications -

Early Retinal Flow Changes After Vitreoretinal Surgery Optical
Journal of Clinical Medicine Article Early Retinal Flow Changes after Vitreoretinal Surgery in Idiopathic Epiretinal Membrane Using Swept Source Optical Coherence Tomography Angiography 1,2, 3, , 3 4 Rodolfo Mastropasqua y, Rossella D’Aloisio * y, Pasquale Viggiano , Enrico Borrelli , Carla Iafigliola 3, Marta Di Nicola 5, Agbéanda Aharrh-Gnama 3, Guido Di Marzio 3, Lisa Toto 3 , Cesare Mariotti 1 and Paolo Carpineto 3 1 Eye Clinic, Polytechnic University of Marche, 60126 Ancona, Italy; [email protected] (R.M.); [email protected] (C.M.) 2 Institute of Ophthalmology, University of Modena and Reggio Emilia, 41121 Modena, Italy 3 Ophthalmology Clinic, Department of Medicine and Science of Ageing, University G. d’Annunzio Chieti-Pescara, 66100 Chieti, Italy; [email protected] (P.V.); carlaiafi[email protected] (C.I.); [email protected] (A.A.-G.); [email protected] (G.D.M.); [email protected] (L.T.); [email protected] (P.C.) 4 Department of Ophthalmology, University Vita Salute, IRCCS Ospedale San Raffaele, 20132 Milan, Italy; [email protected] 5 Laboratory of Biostatistics, Department of Medical, Oral and Biotechnological Sciences, University G. d’Annunzio Chieti-Pescara, 66100 Chieti, Italy; [email protected] * Correspondence: [email protected] These authors contributed equally to this work and should be considered as co-first authors. y Received: 2 October 2019; Accepted: 18 November 2019; Published: 24 November 2019 Abstract: (1) Background: The aim of this observational cross-sectional work was to investigate early retinal vascular changes in patients undergoing idiopathic epiretinal membrane (iERM) surgery using swept source optical coherence tomography angiography (SS-OCTA); (2) Methods: 24 eyes of 24 patients who underwent vitrectomy with internal limiting membrane (ILM) peeling were evaluated pre- and postoperatively using SS-OCTA system (PLEX Elite 9000, Carl Zeiss Meditec Inc., Dublin, CA, USA).