An Unusual Case of Triangular Fibrocartilage Complex Tear After a Wrist-Lock Restraint
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
This Student Guide Belongs To
This student guide belongs to Kyu Level Date of Promotion Yellow Belt (6th Kyu) Orange Belt (5th Kyu) Green Belt (4th Kyu) Purple Belt (3rd Kyu) Blue Belt (2nd Kyu) Brown Belt (1st Kyu) 1st Degree Black Belt (Shodan) 2nd Degree Black Belt (Nidan) 3rd Degree Black Belt (Sandan) 4th Degree Black Belt (Yondan) 5th Degree Black Belt (Godan) Dojo Address: Unit 140, 12811 Clarke Place, Richmond, BC Phone: 604.724.5278 Email: [email protected] Website: www.pacificwavejj.com Dojo Rules and Etiquette he student must constantly be guided by a deep respect for the dojo, other students, instructors and for the purpose of the practice. Good manners, politeness, courteous T behaviour, and a degree of etiquette are part of a student’s training, and important for safety and for developing a proper attitude toward the art. Rules Uniforms & Personal Hygiene The uniform consists of a plain white karate or judo-style gi with a belt and our dojo crest. Students, both men and women, are also required to wear groin protection for safety. An official dojo t-shirt may be worn without the gi top for the first half of class before breakfalls, after which the gi-top must be worn. Personal hygiene is essential as students work closely with others. Fingernails and toenails should be kept clean and trimmed. They should also be filed if cut soon before class as freshly cut nails can be quite sharp. Bodies should be clean and students should use antiperspirant or deodorant. Uniforms should be washed on a regular basis. Long hair must be tied back. -
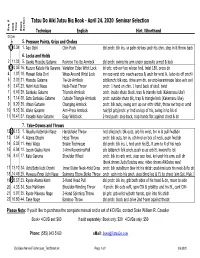
Big Book Named Techniques Testsheet.Xls Page 1 of 1 3/6/2020
Tatsu Do Aiki Jutsu Big Book - April 24, 2020 Seminar Selection Seq. # Seq. DVD Time Book Section Technique English Hint /Shorthand DVD # 5. Pressure Points, Grips and Chokes 11 0.34 1. Ago Oshi Chin Push dbl pnch: blk ins, yr palm strikes undr his chin, step in & throw back 6. Locks and Holds 2 11.33 5. Gyaku Musubu Gatame Reverse Tie-Up Armlock dbl pnch: swing his arm under opposite armpt & lock 32 0.05 16. Kuzure Katate-Ha Garame Variation Edge Wrist Lock lpl grb: grb ovr top w/opp hnd, twist 180, press dn 4 1.07 18. Mawari Kote Dori Wrap-Around Wrist Lock inv opp wrst grb: reach across & undr for wrst lk. (also do off pnch) 5 2.32 21. Musubu Gatame Tie-Up Armlock grb&pnch: blk opp, drive arm dn, sw grip-karaminage (also w/o sw) 6 3.47 23. Nejiri Kubi Nage Neck-Twist Throw pnch: 1 hand on chin, 1 hand back of skull, twist 7 6.49 29. Sankaku Gatame Triangle Armlock pnch: inside shuto block, trap & triangle lock (Kakemasu Uke) 8 7.14 30. Soto Sankaku Gatame Outside Triangle Armlock pnch: outside shuto blk, trap & triangle lock (Kakemasu Uke) 9 9.20 35. Utsuri Gatame Changing Armlock pnch: blk outs, swing arm up ovr eithr shldr, throw ovr top or arnd 10 9.53 36. Wake Gatame Arm-Press Armlock hair/lpl grb/pnch: yr hnd on top of his, swing in to lck el 11 10.41 37. Yasashi Kote Gatame Easy Wristlock 2-hnd push: step back, trap hands flat against chest & dn 7. -

Graderingsbestammelser Jujutsu Vuxn a Ronin Do Fight Gym 2018 07 15
1 Ronin Do Fight Gym Graderingsbestämmelser vuxna JU JUTSU 2018-07-15 Ronin Do Fight Gym Graderingsbestämmelser vuxna 2018-07-15 Ju Jutsu 2 Ronin Do Fight Gym Graderingsbestämmelser vuxna JU JUTSU 2018-07-15 Yellow Belt 5 Kyu Ju jutsu 10 push ups 10 sit ups 55 cm front split and side split Tai Sabaki (Body shifting / Body control) Tai Sabaki 1 – 8 Ukemi Waza (falling techniques) Mae Ukemi Ushiro Ukemi Nage Waza (throwing techniques) Ikkyo /Ude Gatame Nikkyo/ Kote Mawashi O soto Gari Kesa Gatame Jigo Waza (escape techniques) Uke ends up on the floor after each technique. Double wristlock frontal attack. Single wristlock frontal attack. Double wristlock attack from behind. 3 Ronin Do Fight Gym Graderingsbestämmelser vuxna JU JUTSU 2018-07-15 Orange Belt 4 Kyu Ju jutsu 15 push ups 15 sit ups 50 cm front split and side split Tai Sabaki (body shifting) Tai Sabaki 1 – 16 Dashi Waza (standing positions) Shiko Dashi Neko Ashi Dashi Ukemi Waza (falling techniques) Mae Ukemi above 2 people standing on their hands and knees. Daisharin. Nage Waza (throwing techniques) Aiki Otoshi Sankyo/ Kote Hineri Kibusa Gaeshi Kata Gatame 4 Ronin Do Fight Gym Graderingsbestämmelser vuxna JU JUTSU 2018-07-15 Jigo Waza (escape techniques) Uke ends up on the floor after each technique. Double wristlock frontal attack 2 different sets. Single wristlock frontal attack 2 different sets. Double wristlock attack from behind 2 different sets. Defense against 1 Geri. Defense against 1 Tzuki. Randori (sparring with grips, punches and kicks) 1 time x 2 minutes Ne Waza (ground wrestling). -

BJJY Technique Cross-Index Chart
BUDOSHIN JU-JITSU KATA (Professor Kirby's JB=Budoshin Jujitsu Basic Book , JI=Budoshin Jujitsu Intermediate Book, JN=Budoshin Jujitsu Nerve Techniques, V= Budoshin Jujitsu DVD Series) Attack Defense Falls & Rolls Basic Side Fall (Yoko Ukemi) JB-36/V1 Falls & Rolls Basic Back Roll/Fall (Ushiro Ukemi) JB-38/V1 Falls & Rolls Basic Forward Roll (Mae Ukemi) JB-40/V1 Falls & Rolls Basic Forward Fall (Mae Ukemi) JB-42/V1 1 Round Strike Outer Rear Sweeping Throw (Osoto Gari)-Knee Drop Body Strike (Karada Tatake) JB-70/V2-4 2 Cross Wrist Grab Wristlock Takedown (Tekubi Shimi Waza) JI-166/JI-164 3 Double Lapel Grab Double Strike Turning Throw (Ude No Tatake) With Elbow Roll Submission (Hiji Tatake Shimi Waza) JI-84 4 Aggressive Handshake Thumb Tip Press Side Throw (Ube Shioku Waza Yoko Nage) JN-180/V1-12 5 2 Hand Front Choke Throat (Trachea) Attack (Nodo Shioku Waza) JB-54/V1-6 6 Front Bear Hug (Under Arms) Nerve Wheel Throw (Karada Shioku Waza) JB-92/V2-11 7 Rear Bear Hug (Over/Under) Leg Lift (Ashi Ushiro Nage) With Groin Stomp Submission (Kinteki Tatake) JB-50/V1-8 8 Side Sleeve Grab Elbow Lift (Hiji Waza) JB-114/V4-12 9 Straight Knife Lunge Basic Hand Throw (Te Nage) With Wrist or Elbow-Snap Submission (Te/Hiji Maki) JB-58/V1-5, JI-128 Participate in The Weekly Pad Drills/Fundamental Karate & Ju-Jitsu Self-Defense Techniques (10 Week Rotation) 1 Round Strike Basic Drop Throw (Tai-Otoshi) With Wrist-Press Knee-Drop Submission (Tekubi Shimi Waza/Shioku Waza) JB-48/V1-3 2 Double Front Wrist Grab Wrist Side Throw (Haiai Nage or Tekubi Yoko Nage) -

2016 /2017 NFHS Wrestling Rules
2016 /2017 NFHS wrestling Rules The OHSAA and the OWOA wish to thank the National Federation of State High School Associations for the permission to use the photographs to illustrate and better visually explain situations shown in the back of the 2016/17 rule book. © Copyright 2016 by OHSAA and OWOA Falls And Nearfalls—Inbounds—Starting Positions— Technical Violations—Illegal Holds—Potentially Dangerous (5-11-2) A fall or nearfall is scored when (5-11-2) A near fall may be scored when the any part of both scapula are inbounds and the defensive wrestler is held in a high bridge shoulders are over or outside the boundary or on both elbows. line. Hand over nose and mouth that restricts breathing (5-11-2) A near fall may be scored when the (5-14-2) When the defensive wrestler in a wrestler is held in a high bridge or on both pinning situation, illegally puts pressure over elbows the opponents’s mouth, nose, or neck, it shall be penalized. Hand over nose and mouth Out-of-bounds that restricts Inbounds breathing Out-of-bounds Out-of-bounds Inbounds (5-15-1) Contestants are considered to be (5-14-2) Any hold/maneuver over the inbounds if the supporting points of either opponent’s mouth, nose throat or neck which wrestler are inside or on but not beyond the restricts breathing or circulation is illegal boundary 2 Starting Position Legal Neutral Starting Position (5-19-4) Both wrestlers must have one foot on the Legal green or red area of the starting lines and the other foot on line extended, or behind the foot on the line. -

Judo Forum Feb 98
. judo forum tremendous knowledge of the history of February 1998 Welcome the Kodokan prior to 1938. A must read Volume 1, Issue 1 piece about Classical Judo. Vernon Borgen Then Nels Erickson tells tales of a dojo After a stirring conversation on Steve outdoors and in an unheated garage - in Cunningham’s Judo List and years of Minneapolis, Minnesota. Brrrrrrrrr! complaining about the lack of a judo magazine I decided to start one. The third article is by Keo Cavalcanti, Inside this Issue Executive Director of Zen Judo in This past summer “The Judo Athlete” America. Keo shares with us the was born. All too early it died. Taking What is Classical Judo? importance of getting together with our this as a bad omen, “that profitable judo an interview with Steve judo friends on a regular basis for 2 magazines are entirely too unique,” this Cunningham practice and fellowship. magazine will be published for free. The Everywhere Dojo. 11 And finally Jana Seaborn shares with us Feel free to make copies of the the struggle and the courage to fight a magazine “as-a-whole” for free Crossing the Pond, river. This is a great story about Sei distribution (you can charge for Making Connections Ryoku Zen Yo. 12 printing expenses) and for the purpose expressed, i.e. to educate We are looking for good stories, Fargo Judoka Join Flood about judo. Any other use is research, interesting pictures and Fight 14 prohibited and subject to written cartoons. Feel free to contribute. request. The entire contents of this Atemi-Waza magazine are copyrighted. -

Sag E Arts Unlimited Martial Arts & Fitness Training
Sag e Arts Unlimited Martial Arts & Fitness Training Grappling Intensive Program - Basic Course - Sage Arts Unlimited Grappling Intensive Program - Basic Course Goals for this class: - To introduce and acclimate students to the rigors of Grappling. - To prepare students’ technical arsenal and conceptual understanding of various formats of Grappling. - To develop efficient movement skills and defensive awareness in students. - To introduce students to the techniques of submission wrestling both with and without gi’s. - To introduce students to the striking aspects of Vale Tudo and Shoot Wrestling (Shooto) and their relationship to self-defense, and methods for training these aspects. - To help students begin to think tactically and strategically regarding the opponent’s base, relative position and the opportunities that these create. - To give students a base of effective throws and breakfalls, transitioning from a standing format to a grounded one. Class Rules 1. No Injuries 2. Respect your training partner, when they tap, let up. 3. You are 50% responsible for your safety, tap when it hurts. 4. An open mind is not only encouraged, it is mandatory. 5. Take Notes. 6. No Whining 7. No Ego 8. No Issues. Bring Every Class Optional Equipment Notebook or 3-ring binder for handouts and class notes. Long or Short-sleeved Rashguard Judo or JiuJitsu Gi and Belt Ear Guards T-shirt to train in (nothing too valuable - may get stretched out) Knee Pads Wrestling shoes (optional) Bag Gloves or Vale Tudo Striking Gloves Mouthguard Focus Mitts or Thai Pads Smiling Enthusiasm and Open-mindedness 1 Introduction Grappling Arts from around the World Nearly every culture has its own method of grappling with a unique emphasis of tactic, technique and training mindset. -

Hapkido 1St Gup Requirement Paperwork
Hayme Serrato’s Martial Arts Hapkido 1st Gup (Black Belt with White Stripe) Testing Requirements Two Hand Lapel Grab 5. Double slap and trap takedown and strike: Left hand slap face and trap attacker’s left hand Right hand slap face and position forearm on attacker’s radial nerve At the same time: • Step back right • Right press down on radial nerve to bring attacker to his knees Shoot out both hands to strike face 6. Throat choke head twist throw: Right scoop kick At the same time: • Step down forward • Right hand tiger mouth to attacker’s throat Left grab attacker’s hair on the back of his head Twist head to the left to takedown Finish with punch 1st Gup (Black Belt with White Stripe) - 1 January 2, 2014 Belt Grab (Palm Up) (Attacker’s right hand grabs your belt) 3. Under strike elbow, collar grab throw: Right hand (palm up) grab attacker’s right wrist to trap it on your belt At the same time: • Left foot slide in slightly • Left forearm strike up on attacker’s right elbow to hyper extend it Slide your left hand through to grab attacker’s lapel Armbar takedown: • Right push down on attacker’s wrist • Left push against attacker’s elbow • Step back right to takedown 4. Outside wrist lock throw: At the same time: • Right palm heel to face • Left hand inverted grip attacker’s right wrist (tiger mouth towards you) Right grab attacker’s forearm on top so the back of both of your palms are facing down Wristlock takedown: • Turn attacker’s wrist to left to apply wristlock • Step back left to takedown Pull attacker’s hand off belt, finish with arm lock Full Nelson (Non-Prevented) 3. -

Ryukyukai Jujutsu Curriculum 2018
Ryukyukai jujutsu curriculum 2018 WHITE BELT TO YELLOW BELT (ROKKYU/6th KYU): STANCES- Basic, Cat, Front, Back, Kumite, Crouch BREAKFALLS- Front, Rear, Side , Roll [Front, back & Side], (Kneeling) BASIC STRIKES- Front punch, Reverse Punch, Knifehand, Backfist BASIC KICKS- Front Kick, Side Kick, Round House, Back Snap BASIC HAND ESCAPES- Pull from thumb/ forefinger, minimum 3 simple wrist & gi grab defenses for 1 &2 hand each. WARMING UPS & STRETCHING – Comprehensive- includes full upper /lower body & joint flexibility & rolls/breakfalls. REIGI (ETIQUETTE) Per Sensei- Opening & Closing Salute, Basic Dojo/Uke& Tori Ettiquette, etc. YELLOW BELT TO ORANGE BELT (GOKKYU/5th KYU) INTERMEDIATE BREAKFALLS - Front, Rear, Side , Roll [Front, back & Side], (Standing) INTERMEDIATE STRIKES- Multiple angle knife, back & hammerfist, introductory vital (pressure point/nerve) strikes INTERMEDIATE KICKS- Back Kick ( Hook), Reverse Roundhouse, INTERMEDIATE HAND ESCAPES- Crossing, pinning & trapping escapes BASIC BODY ESCAPES- Minimum 3 each front, rear & side bearhug. ORANGE BELT TO GREEN BELT (YONKYU/4th KYU): ADVANCED BREAKFALLS - Front, Rear, Side , Roll [Front, back & Side], (over crouched person) ADVANCED STRIKES- Comprehensive nerve & pressure point strikes, blocks as strikes & vice versa. ADVANCED KICKS- Combination & Turning Kicks, Kick Takedowns, Double Kicks, etc. BASIC FOOTWORK, BLOCKS AND EVASION- Tai Sabaki- fighting angles (front, side & diagonals), Standard Side, Low, Middle, High & Elbow Protecting Head Block. BASIC TAKEDOWNS- Sweep, Inner/Outer Reap, Single/Double Leg, Knee Tackle INTERMEDIATE BODY ESCAPES- Minimum 3 more front, rear & side bearhug. GREEN BELT TO PURPLE BELT (SANKYU/3rd KYU): INTERMEDIATE FOOTWORK, BLOCKS AND EVASION- Sweeping Steps, Shooting in , Barely Dodging (Pivoting to Evade), Stomp Kick Back/Side of Knee, Knee to knee, Ridge Blocks, Scooping kick Blocks, Cross Blocks (Low Middle & High) Catch & Grab Blocks, Soft Blocks(Snake Blocks), Palm Blocks w/catch & pressure point grab, Circling 2 Hand Block. -

Black Belt Guide to All Techniques in Budoshin Jujitsu Forms from White Belt Through Tenth-Degree Black Belt
BLACK BELT GUIDE TO ALL TECHNIQUES IN BUDOSHIN JUJITSU FORMS FROM WHITE BELT THROUGH TENTH-DEGREE BLACK BELT ALPHABETIZED PROMPTS SENSEI DAVE CLARK, SANDAN No matter how educated, talented, rich or cool you are, how you treat people ultimately tells all. Integrity is important. – Author Unknown OTHER BOOKS By DAVE CLARK : PIANO COMPANION A COMPREHENSIVE APPROACH TO LEARNING HOW TO PLAy THE PIANO By NOTE, CHORD SyMBOL, AND EAR 1985 DAVE CLARK JIU-JITSU CONSORTIUM INTEGRITy, HUMILITy, RESPECT 2007 BALANCE THE ART OF TEACHING THE GENTLE ART DIRECTED POSITIVE ACTION FOR EVERyDAy LIVING 2010 PIANO STUDENT’S TOOL KIT EASy WAyS TO LEARN ALL THE GOOD STUFF 2016 COMPLETE GUIDE TO ALL BUDOSHIN JUJITSU TECHNIQUES FROM WHITE BELT THROUGH TENTH-DEGREE BLACK BELT QUICK CROSS-REFERENCE STUDy GUIDES, PROMPTS, TEST STUDy GUIDES 2017 CONTACT : [email protected] BUSINESS : 813 685 9118 CELL : 813 514 3016 ADDITIONAL RESOURCES: WWW.KATAGUIDE.yOLASITE.COM Table of Contents Page Introduction 1 Budoshin Jujitsu Belt Levels 3 A Creative Teaching Approach – The Power of Compound Instruction 4 Technique versus Form – The Waza in Kata 7 Budoshin Jujitsu’s Use of Japanese Terminology – Loquacious Linguistics 9 Suggested Reading and Viewing – Seek and Ye Shall Search 11 How to Use This Black Belt Guide – Dissecting the Moving Parts 12 Explanation of Acronyms – Answers Afore Anyone Asks 14 Table of Terms – Perceiving Parameters 15 Table of Prompts – Sixty Study Sessions 16 Alphabetized Prompts 19 A 21 B 25 E 26 G 27 H 29 I 40 J 41 K 42 M 53 N 63 O 66 S 67 T 81 U -
Defensive Tactics During Their Breaks, but Mostly It’S in Preparation for an Upcoming Test
Table of Contents Introduction 15 SECTION 1: THE FOUNDATION: NUTS AND BOLTS 19 Chapter 1: Thinking Ahead 21 Adrenaline Response 21 The Power Of Combat Breathing 23 How to do it 24 The Importance Of Visualizing 25 Visualize the confrontation 26 Chapter 2: The Value of Reps 27 It’s All About Reps 27 Line Drill: Attack And Response 28 Monkey Line Drill 31 Chapter 3: The Elements of Balance 35 The Tripod Concept 35 The invisible third leg 36 Be cognizant of your position 41 Using the tripod to your advantage 42 Kuzushi 47 Handcuffing 51 Mental Kuzushi 55 Developing self-awareness 57 Chapter 4: Crossing the Gap 59 Moving into Range 59 A potentially dangerous moment 59 His body language 59 Your stance 60 Timing the move 61 Where to move 62 How to grab 63 Chapter 5: Blocking 65 Blocking and Shielding 65 Shielding 68 Chapter 6: Weight Training and Aerobics 71 Fast-twitch muscle fibers 72 Aerobic and anaerobic 75 SECTION 2: JOINT MANIPULATION AND LEVERAGE CONTROL 77 Chapter 7: Finger Techniques 79 Elements of Applying Finger Techniques 80 Applications 82 Chapter 8: The Versatile Wristlock 93 Elements of the Wristlock 93 Standing Suspect 95 Downed Suspect 104 Wristlock takedowns 112 When the suspect resists your grab 119 Wristlock Pickups 120 Elements of the Wrist Twist 127 Applications 129 Inverted Wrist Flex 134 Elements of inverted wrist flex 134 Applications 135 Chapter 9: Wrist Crank 139 Elements of the Wrist Crank 139 Applications 140 Handcuffing from the wrist crank position 146 Chapter 10: Elbow Techniques 149 Armbar 149 Elements of the -
Heroes Fundamentals Workbook V 1.01 Thank You for Downloading the Heroes Fundamentals Workbook
Heroes Fundamentals Workbook v 1.01 Thank you for downloading the Heroes Fundamentals Workbook. This workbook is designed to help you track your own progress and make an honest assessment of your abilities in Jiu Jitsu. This workbook is specifically designed with White/Blue belt level in mind, but anyone could benefit from this. HOW TO USE THIS WORKBOOK: Fill out the Heroes Fundamentals Worksheet to the best of your abilities. Only fill out the worksheet with techniques that are actually in your current arsenal. If you don’t have a technique for a particular position, leave that slot blank. At the Fundamental level there should be NO MORE than two (2) techniques per box. The exercise is to list two techniques that you have at each position that would be your first and second choices when in the particular position. Ideally each of these positions should be complimentary to each other. After filling out the worksheet with techniques, give a rating between 1-5 on how comfortable you are with each technique: 1. I have learned the technique in Fundamentals and I don’t really get it 2. I have drilled the technique in Fundamentals and it makes sense, but I haven’t had to chance to use it in drilling and sparring much. 3. I have drilled the technique and I feel I can use it against someone at a lower overall level than me. 4. I have drilled the technique and I feel that I can use it against someone at the same overall level as me.