VOL 20 NO4 Oct-Dec 2013
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

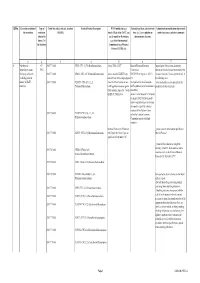
Summary of Offerings in the PBS Bulb Exchange, Dec 2012- Nov 2019
Summary of offerings in the PBS Bulb Exchange, Dec 2012- Nov 2019 3841 Number of items in BX 301 thru BX 463 1815 Number of unique text strings used as taxa 990 Taxa offered as bulbs 1056 Taxa offered as seeds 308 Number of genera This does not include the SXs. Top 20 Most Oft Listed: BULBS Times listed SEEDS Times listed Oxalis obtusa 53 Zephyranthes primulina 20 Oxalis flava 36 Rhodophiala bifida 14 Oxalis hirta 25 Habranthus tubispathus 13 Oxalis bowiei 22 Moraea villosa 13 Ferraria crispa 20 Veltheimia bracteata 13 Oxalis sp. 20 Clivia miniata 12 Oxalis purpurea 18 Zephyranthes drummondii 12 Lachenalia mutabilis 17 Zephyranthes reginae 11 Moraea sp. 17 Amaryllis belladonna 10 Amaryllis belladonna 14 Calochortus venustus 10 Oxalis luteola 14 Zephyranthes fosteri 10 Albuca sp. 13 Calochortus luteus 9 Moraea villosa 13 Crinum bulbispermum 9 Oxalis caprina 13 Habranthus robustus 9 Oxalis imbricata 12 Haemanthus albiflos 9 Oxalis namaquana 12 Nerine bowdenii 9 Oxalis engleriana 11 Cyclamen graecum 8 Oxalis melanosticta 'Ken Aslet'11 Fritillaria affinis 8 Moraea ciliata 10 Habranthus brachyandrus 8 Oxalis commutata 10 Zephyranthes 'Pink Beauty' 8 Summary of offerings in the PBS Bulb Exchange, Dec 2012- Nov 2019 Most taxa specify to species level. 34 taxa were listed as Genus sp. for bulbs 23 taxa were listed as Genus sp. for seeds 141 taxa were listed with quoted 'Variety' Top 20 Most often listed Genera BULBS SEEDS Genus N items BXs Genus N items BXs Oxalis 450 64 Zephyranthes 202 35 Lachenalia 125 47 Calochortus 94 15 Moraea 99 31 Moraea -

Survey for Special-Status Vascular Plant Species
SURVEY FOR SPECIAL-STATUS VASCULAR PLANT SPECIES For the proposed Eagle Canyon Fish Passage Project Tehama and Shasta Counties, California Prepared for: Tehama Environmental Solutions 910 Main Street, Suite D Red Bluff, California 96080 Prepared by: Dittes & Guardino Consulting P.O. Box 6 Los Molinos, California 96055 (530) 384-1774 [email protected] Eagle Canyon Fish Passage Improvement Project - Botany Report Sept. 12, 2018 Prepared by: Dittes & Guardino Consulting 1 SURVEY FOR SPECIAL-STATUS VASCULAR PLANT SPECIES Eagle Canyon Fish Passage Project Shasta & Tehama Counties, California T30N, R1W, SE 1/4 Sec. 25, SE1/4 Sec. 24, NE ¼ Sec. 36 of the Shingletown 7.5’ USGS Topographic Quadrangle TABLE OF CONTENTS I. Executive Summary ................................................................................................................................................. 4 II. Introduction ............................................................................................................................................................ 4 III. Project Description ............................................................................................................................................... 4 IV. Location .................................................................................................................................................................. 5 V. Methods .................................................................................................................................................................. -
Qrno. 1 2 3 4 5 6 7 1 CP 2903 77 100 0 Cfcl3
QRNo. General description of Type of Tariff line code(s) affected, based on Detailed Product Description WTO Justification (e.g. National legal basis and entry into Administration, modification of previously the restriction restriction HS(2012) Article XX(g) of the GATT, etc.) force (i.e. Law, regulation or notified measures, and other comments (Symbol in and Grounds for Restriction, administrative decision) Annex 2 of e.g., Other International the Decision) Commitments (e.g. Montreal Protocol, CITES, etc) 12 3 4 5 6 7 1 Prohibition to CP 2903 77 100 0 CFCl3 (CFC-11) Trichlorofluoromethane Article XX(h) GATT Board of Eurasian Economic Import/export of these ozone destroying import/export ozone CP-X Commission substances from/to the customs territory of the destroying substances 2903 77 200 0 CF2Cl2 (CFC-12) Dichlorodifluoromethane Article 46 of the EAEU Treaty DECISION on August 16, 2012 N Eurasian Economic Union is permitted only in (excluding goods in dated 29 may 2014 and paragraphs 134 the following cases: transit) (all EAEU 2903 77 300 0 C2F3Cl3 (CFC-113) 1,1,2- 4 and 37 of the Protocol on non- On legal acts in the field of non- _to be used solely as a raw material for the countries) Trichlorotrifluoroethane tariff regulation measures against tariff regulation (as last amended at 2 production of other chemicals; third countries Annex No. 7 to the June 2016) EAEU of 29 May 2014 Annex 1 to the Decision N 134 dated 16 August 2012 Unit list of goods subject to prohibitions or restrictions on import or export by countries- members of the -

Conserving Europe's Threatened Plants
Conserving Europe’s threatened plants Progress towards Target 8 of the Global Strategy for Plant Conservation Conserving Europe’s threatened plants Progress towards Target 8 of the Global Strategy for Plant Conservation By Suzanne Sharrock and Meirion Jones May 2009 Recommended citation: Sharrock, S. and Jones, M., 2009. Conserving Europe’s threatened plants: Progress towards Target 8 of the Global Strategy for Plant Conservation Botanic Gardens Conservation International, Richmond, UK ISBN 978-1-905164-30-1 Published by Botanic Gardens Conservation International Descanso House, 199 Kew Road, Richmond, Surrey, TW9 3BW, UK Design: John Morgan, [email protected] Acknowledgements The work of establishing a consolidated list of threatened Photo credits European plants was first initiated by Hugh Synge who developed the original database on which this report is based. All images are credited to BGCI with the exceptions of: We are most grateful to Hugh for providing this database to page 5, Nikos Krigas; page 8. Christophe Libert; page 10, BGCI and advising on further development of the list. The Pawel Kos; page 12 (upper), Nikos Krigas; page 14: James exacting task of inputting data from national Red Lists was Hitchmough; page 16 (lower), Jože Bavcon; page 17 (upper), carried out by Chris Cockel and without his dedicated work, the Nkos Krigas; page 20 (upper), Anca Sarbu; page 21, Nikos list would not have been completed. Thank you for your efforts Krigas; page 22 (upper) Simon Williams; page 22 (lower), RBG Chris. We are grateful to all the members of the European Kew; page 23 (upper), Jo Packet; page 23 (lower), Sandrine Botanic Gardens Consortium and other colleagues from Europe Godefroid; page 24 (upper) Jože Bavcon; page 24 (lower), Frank who provided essential advice, guidance and supplementary Scumacher; page 25 (upper) Michael Burkart; page 25, (lower) information on the species included in the database. -

Genome Annotation of Fritillaria Agrestis Bac Clone
GENOME ANNOTATION OF FRITILLARIA AGRESTIS BAC CLONE ___________________ A University Thesis Presented to the Faculty of California State University, East Bay ___________________ In Partial Fulfillment of the Requirements for the Degree Master of Science in Biological Science ___________________ By Rajhalutshimi Narayanaswamy September 2015 GENOME ANNOTATION OF FRITILLARJA AGRESTIS BAC CLONE By Rajhalutshimi Narayanaswamy Date: A~~u, ~o1s ii Acknowledgments I would like to thank my advisors Dr.Chris Baysdorfer, Dr.Claudia Udhe-Stone and Dr.Kenneth Curr for their support, guidance and encouragement that helped me to complete this project successfully. I would also like to thank my family members who have been supportive during the course of my project. iii Table of Contents Acknowledgments.............................................................................................................. iii List of Figures ................................................................................................................... vii 1 Introduction ...............................................................................................................1 1.1 Genome size variation ...........................................................................................1 1.2 Brief outline of the mechanisms of genome size variation ...................................2 1.3 Repetitious DNA ...................................................................................................3 1.4 Annotation ...........................................................................................................21 -

Tracing History
Comprehensive Summaries of Uppsala Dissertations from the Faculty of Science and Technology 911 Tracing History Phylogenetic, Taxonomic, and Biogeographic Research in the Colchicum Family BY ANNIKA VINNERSTEN ACTA UNIVERSITATIS UPSALIENSIS UPPSALA 2003 Dissertation presented at Uppsala University to be publicly examined in Lindahlsalen, EBC, Uppsala, Friday, December 12, 2003 at 10:00 for the degree of Doctor of Philosophy. The examination will be conducted in English. Abstract Vinnersten, A. 2003. Tracing History. Phylogenetic, Taxonomic and Biogeographic Research in the Colchicum Family. Acta Universitatis Upsaliensis. Comprehensive Summaries of Uppsala Dissertations from the Faculty of Science and Technology 911. 33 pp. Uppsala. ISBN 91-554-5814-9 This thesis concerns the history and the intrafamilial delimitations of the plant family Colchicaceae. A phylogeny of 73 taxa representing all genera of Colchicaceae, except the monotypic Kuntheria, is presented. The molecular analysis based on three plastid regions—the rps16 intron, the atpB- rbcL intergenic spacer, and the trnL-F region—reveal the intrafamilial classification to be in need of revision. The two tribes Iphigenieae and Uvularieae are demonstrated to be paraphyletic. The well-known genus Colchicum is shown to be nested within Androcymbium, Onixotis constitutes a grade between Neodregea and Wurmbea, and Gloriosa is intermixed with species of Littonia. Two new tribes are described, Burchardieae and Tripladenieae, and the two tribes Colchiceae and Uvularieae are emended, leaving four tribes in the family. At generic level new combinations are made in Wurmbea and Gloriosa in order to render them monophyletic. The genus Androcymbium is paraphyletic in relation to Colchicum and the latter genus is therefore expanded. -

Document Converted With
Southwest Turkey A Greentours Trip Report 21st March – 2nd April 2010 Led by Başak Gardner Day 1 Journey to Antalya 21.03.10 I met the group at the airport and directly drove to the hotel. It was around 10 pm. Day 2 Journey to Ibradı 22.03.10 With good news from the meteorology the tour started. Alpine Swifts were flying around and Yellow-vented Bulbuls were singing from the roof as we were having our breakfast by the pool. A very short visit to the bank to change and get some money gave a chance for the group to take some pictures of the castle walls and gate. We even did some botanizing. The walls of the very old houses in the old town were almost covered by Cymbalaria longipes. We were on the road before 10 am and our first stop was by a graveyard where Pyrus serikensis, which is an endangered endemic pear tree, was in full bloom. But the main plant we were looking for was a bit over, however we managed to find some fresh reticulately-patterned Iris masia. Along with these were some Muscari comosum, Anemone coronaria and a single plant of Gladiolus italicus. Val spotted our first butterfly an Eastern Festoon and both Large White and Orange Tip were also seen as well as Danford’s Lizard. We made another stop both to have lunch and to look for some Ophrys. Along an old track by the picnic site we encountered many Ophrys mammosa spikes in good flower. We had a good lunch with some Turkish tea our driver prepared for us among the Bellis annua flowers. -

Assessment of Genetic Fidelity of Fritillaria Dagana (Liliaceae) Regenerated Plants Using ISSR Markers
BIO Web of Conferences 11, 00029 (2018) https://doi.org/10.1051/bioconf/20181100029 Prospects of Development and Challenges of Modern Botany Assessment of genetic fidelity of Fritillaria dagana (Liliaceae) regenerated plants using ISSR markers Dinara S. Muraseva1,*, Elena V. Kobozeva1,2, and Tatyana I. Novikova1 1Central Siberian Botanical Garden, Siberian Branch RAS, 630090 Novosibirsk, Russia 2National Research Tomsk State University, 634050, Tomsk, Lenina pr., 36 Abstract. ISSR analysis of Fritillaria dagana , endangered ornamental geophyte from the Sayan Mountains, regenerated through direct gemmogenesis from bulb scale tissue was performed. More informative electrophoresis profile with clear and distinct bands was obtained at amplification with (CAC)3GC primer at 56 ºC annealing. The genetic fidelity of F.dagana regenerants to maternal plants was confirmed. 1 Introduction The genus Fritillaria L. (Liliaceae) presents ephemeral bulbous plants and comprises more than 150 species distributed within the Northern Hemisphere with a pronounced center of diversity in southwestern and Himalayan Asia [1]. Twelve of fritillaria species occur in the territory of Russia, therewith five of them are listed in the Red Data Book of the Russian Federation [2] with the status of rare species. Since many natural species of the genus Fritillaria are endangered due to irregular gathering the bulbs and flowering shoots, it is necessary to find new effective approaches for their conservation. Previously we developed the protocol of clonal micropropagation of local endemic Fritillaria sonnikovae Schaulo and A. Erst from West Sayan for creation of in vitro Fritillaria collection [3]. Fritillaria dagana Turcz. ex Trautv. is an endemic species listed in the Red Data Book of the Russian Federation [2] with the status of a rare species (3a) which occurs in certain areas of Siberia, East Sayan and Southern Baikal. -
Botanical Resources and Wetlands Technical Report
Chapter 1 Affected Environment Figure 1-3g. Sensitive Biological Resources Between Shasta Dam and Red Bluff Pumping Plant 1-45 Draft – June 2013 Shasta Lake Water Resources Investigation Biological Resources Appendix – Botanical Resources and Wetlands Technical Report This page left blank intentionally. 1-46 Draft – June 2013 Chapter 1 Affected Environment Figure 1-3h. Sensitive Biological Resources Between Shasta Dam and Red Bluff Pumping Plant 1-47 Draft – June 2013 Shasta Lake Water Resources Investigation Biological Resources Appendix – Botanical Resources and Wetlands Technical Report This page left blank intentionally. 1-48 Draft – June 2013 Chapter 1 Affected Environment Figure 1-3i. Sensitive Biological Resources Between Shasta Dam and Red Bluff Pumping Plant 1-49 Draft – June 2013 Shasta Lake Water Resources Investigation Biological Resources Appendix – Botanical Resources and Wetlands Technical Report This page left blank intentionally. 1-50 Draft – June 2013 Chapter 1 Affected Environment Figure 1-3j. Sensitive Biological Resources Between Shasta Dam and Red Bluff Pumping Plant 1-51 Draft – June 2013 Shasta Lake Water Resources Investigation Biological Resources Appendix – Botanical Resources and Wetlands Technical Report This page left blank intentionally. 1-52 Draft – June 2013 Chapter 1 Affected Environment 1 Valley Oak Woodland This habitat type consists of an open savanna of 2 valley oak (Quercus lobata) trees and an annual grassland understory. Valley 3 oak is typically the only tree species present and shrubs are generally absent 4 except for occasional poison oak. Canopy cover rarely exceeds 30–40 percent in 5 valley oak woodland. This community occupies the highest portions of the 6 floodplain terrace where flooding is infrequent and shallow. -
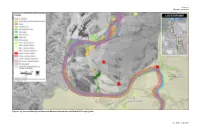
Botanical Priority Guidebook
Botanical Priority Protection Areas Alameda and Contra Costa Counties the East Bay Regional Park District. However, certain BPPAs include Hills have been from residential development. public parcels or properties with other conservation status. These are cases where land has been conserved since the creation of these boundaries or where potential management decisions have the poten- Following this initial mapping effort, the East Bay Chap- \ ntroduction tial to negatively affect an area’s botanical resources. Additionally, ter’s Conservation Committee began to utilize the con- each acre within these BPPAs represents a potential area of high pri- cept in draft form in key local planning efforts. Lech ority. Both urban and natural settings are included within these Naumovich, the chapter’s Conservation Analyst staff The lands that comprise the East Bay Chapter are located at the convergence boundaries, therefore, they are intended to be considered as areas person, showcased the map set in forums such as the of the San Francisco Bay, the North and South Coast Ranges, the Sacra- warranting further scrutiny due to the abundance of nearby sensitive BAOSC’s Upland Habitat Goals Project and the Green mento-San Joaquin Delta, and the San Joaquin Valley. The East Bay Chapter botanical resources supported by high quality habitat within each E A S T B A Y Vision Group (in association with Greenbelt Alliance); area supports a unique congregation of ecological conditions and native BPPA. Although a parcel, available for preservation through fee title C N P S East Bay Regional Park District’s Master Plan Process; plants. Based on historic botanical collections, the pressures from growth- purchase or conservation easement, may be located within the and local municipalities. -

Rock Garden Quarterly
ROCK GARDEN QUARTERLY VOLUME 55 NUMBER 2 SPRING 1997 COVER: Tulipa vvedevenskyi by Dick Van Reyper All Material Copyright © 1997 North American Rock Garden Society Printed by AgPress, 1531 Yuma Street, Manhattan, Kansas 66502 ROCK GARDEN QUARTERLY BULLETIN OF THE NORTH AMERICAN ROCK GARDEN SOCIETY VOLUME 55 NUMBER 2 SPRING 1997 FEATURES Life with Bulbs in an Oregon Garden, by Molly Grothaus 83 Nuts about Bulbs in a Minor Way, by Andrew Osyany 87 Some Spring Crocuses, by John Grimshaw 93 Arisaema bockii: An Attenuata Mystery, by Guy Gusman 101 Arisaemas in the 1990s: An Update on a Modern Fashion, by Jim McClements 105 Spider Lilies, Hardy Native Amaryllids, by Don Hackenberry 109 Specialty Bulbs in the Holland Industry, by Brent and Becky Heath 117 From California to a Holland Bulb Grower, by W.H. de Goede 120 Kniphofia Notes, by Panayoti Kelaidis 123 The Useful Bulb Frame, by Jane McGary 131 Trillium Tricks: How to Germinate a Recalcitrant Seed, by John F. Gyer 137 DEPARTMENTS Seed Exchange 146 Book Reviews 148 82 ROCK GARDEN QUARTERLY VOL. 55(2) LIFE WITH BULBS IN AN OREGON GARDEN by Molly Grothaus Our garden is on the slope of an and a recording thermometer, I began extinct volcano, with an unobstructed, to discover how large the variation in full frontal view of Mt. Hood. We see warmth and light can be in an acre the side of Mt. Hood facing Portland, and a half of garden. with its top-to-bottom 'H' of south tilt• These investigations led to an inter• ed ridges. -

Botany Biological Assessment/ Biological Evaluation
Botany Biological Assessment/ Biological Evaluation for the Lehigh Southwest Land Exchange Shasta-Trinity National Recreation Area Shasta-Trinity National Forest Shasta County, California December 2012 Prepared by: 3/13/13 Leslie Perry, Environmental Analyst/Biologist Date Reviewed by: Martin Lenz, Shasta Lake District Botanist Date Botany BA/BE Lehigh Southwest Land Exchange FINAL I. PROJECT DESCRIPTION The Shasta-Trinity National Forest (STNF) proposes to exchange lands with Lehigh Southwest Cement Company (Lehigh) and approve a non-significant amendment to the STNF Land and Resource Management Plan (U.S. Forest Service 1994). The lands to be exchanged include two Federal parcels managed by the Forest Service near the Gray Rocks quarry on the south side of Shasta Lake east of Interstate 5, encompassing approximately 62.56 acres, and one private parcel owned by Lehigh on the east side of Shasta Lake at the McCloud River arm, encompassing up to approximately 243.94 acres (specific acreage to be determined during land appraisal). Easements on Road 33N99 would also be exchanged as part of the land transfer to maintain access for each party across the lands. The lands and Road 33N99 are in the Shasta Unit of the Whiskeytown-Shasta-Trinity National Recreation Area on the STNF in Shasta County, California. The purpose of the exchange from private to Federal ownership is to consolidate National Forest ownership of lands in the Shasta Unit of the NRA and protect high quality plant and wildlife habitat along the McCloud River arm of Shasta Lake. A complete description of the purpose and need and alternatives can be found in the Environmental Assessment (see project record).