Situation Report on Cholera in Zimbabwe Issue Number 9 6 January 2009
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Conference Paper Series
POLITICAL ECONOMY RESEARCH INSTITUTE University of Massachusetts Amherst Community Rights, Costs, and Benefits: The Question of Natural Resource Stewardship and Community Benefits in Zimbabwe’s CAMPFIRE Program James C. Murombedzi January 2003 CONFERENCE PAPER SERIES No. 16 Committees, Rights, Costs and Benefits: The Question of Natural Resource Stewardship and Community Benefits in Zimbabwe’s CAMPFIRE Program James C. Murombedzi The Ford Foundation Johannesburg, South Africa 1 In the CAMPFIRE formulation, the resource management problems obtaining in the communal areas of Zimbabwe are the result of the absence of both the institutional capacity as well as the incentives to manage the resources in question. The CAMPFIRE solution, therefore, was to introduce new systems of group ownership and territorial rights to natural resources to communities, and provide the appropriate institutions for legitimate resource management for the benefit of these communities (Martin 1986). The implementation of this solution was attained through the enactment of an amendment to the Parks and Wild Life Act of 1975, which enables the government to delegate appropriate authority over the wildlife to the ‘communal representatives’. The CAMPFIRE program in fact constitutes a transfer of the notion of ownership, successfully implemented with regard to individual landowners, to communal landowners (Farquharson 1993). This chapter tests the extent to which CAMPFIRE has in fact been able to devolve ownership over wildlife to communities in the communal areas, and thereby promoted stewardship of wildlife through the production of benefits for the participating communities. To achieve this, I will proceed by first evaluating the extent to which CAMPFIRE has succeeded in eliciting stewardship of the wildlife resource by participating communities through the devolution of clear and unambiguous rights to wildlife to these communities. -
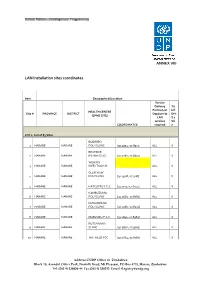
LAN Installation Sites Coordinates
ANNEX VIII LAN Installation sites coordinates Item Geographical/Location Service Delivery Tic Points (List k if HEALTH CENTRE Site # PROVINCE DISTRICT Dept/umits DHI (EPMS SITE) LAN S 2 services Sit COORDINATES required e LOT 1: List of 83 Sites BUDIRIRO 1 HARARE HARARE POLYCLINIC [30.9354,-17.8912] ALL X BEATRICE 2 HARARE HARARE RD.INFECTIO [31.0282,-17.8601] ALL X WILKINS 3 HARARE HARARE INFECTIOUS H ALL X GLEN VIEW 4 HARARE HARARE POLYCLINIC [30.9508,-17.908] ALL X 5 HARARE HARARE HATCLIFFE P.C.C. [31.1075,-17.6974] ALL X KAMBUZUMA 6 HARARE HARARE POLYCLINIC [30.9683,-17.8581] ALL X KUWADZANA 7 HARARE HARARE POLYCLINIC [30.9285,-17.8323] ALL X 8 HARARE HARARE MABVUKU P.C.C. [31.1841,-17.8389] ALL X RUTSANANA 9 HARARE HARARE CLINIC [30.9861,-17.9065] ALL X 10 HARARE HARARE HATFIELD PCC [31.0864,-17.8787] ALL X Address UNDP Office in Zimbabwe Block 10, Arundel Office Park, Norfolk Road, Mt Pleasant, PO Box 4775, Harare, Zimbabwe Tel: (263 4) 338836-44 Fax:(263 4) 338292 Email: [email protected] NEWLANDS 11 HARARE HARARE CLINIC ALL X SEKE SOUTH 12 HARARE CHITUNGWIZA CLINIC [31.0763,-18.0314] ALL X SEKE NORTH 13 HARARE CHITUNGWIZA CLINIC [31.0943,-18.0152] ALL X 14 HARARE CHITUNGWIZA ST.MARYS CLINIC [31.0427,-17.9947] ALL X 15 HARARE CHITUNGWIZA ZENGEZA CLINIC [31.0582,-18.0066] ALL X CHITUNGWIZA CENTRAL 16 HARARE CHITUNGWIZA HOSPITAL [31.0628,-18.0176] ALL X HARARE CENTRAL 17 HARARE HARARE HOSPITAL [31.0128,-17.8609] ALL X PARIRENYATWA CENTRAL 18 HARARE HARARE HOSPITAL [30.0433,-17.8122] ALL X MURAMBINDA [31.65555953980,- 19 MANICALAND -

THE HISTORY of the TONGA and FISHING COOPERATIVES in BINGA DISTRICT 1950S-2015
FACULTY OF ARTS DEPARTMENT OF HISTORY EMPOWERMENT OR CONTROL? : THE HISTORY OF THE TONGA AND FISHING COOPERATIVES IN BINGA DISTRICT 1950s-2015 BY HONOUR M.M. SINAMPANDE R131722P DISSERTATION SUBMITTED TO THE FACULTY OF ARTS IN PARTIAL FULLFILMENT OF THE REQUIREMENTS OF THE HONOURS DEGREE IN HISTORY AT MIDLANDS STATE UNIVERSITY. NOVEMBER 2016 ZVISHAVANE: ZIMBABWE SUPERVISOR DR. T.M. MASHINGAIDZE APPROVAL FORM The undersigned certify that they have supervised the student Honour M.M Sinampande (R131722P) dissertation entitled Empowerment or Control? : The history of the Tonga and fishing cooperatives in Binga District 1950-210 submitted in partial fulfillment of the requirements of the Bachelor of Arts in History Honours Degree offered by Midlands State University. Dr. T.M Mashingaidze ……………………… SUPERVISOR DATE …….……………………………………… …………………………….. CHAIRPERSON DATE ….………………………………………… …………………………….. EXTERNAL EXAMINER DATE DECLARATION I, Honour M.M Sinampande declare that, Empowerment or Control? : The history of the Tonga and fishing cooperatives in Binga District 1950s-2015 is my own work and it has never been submitted before any degree or examination in any other university. I declare that all sources which have been used have been acknowledged. I authorize the Midlands State University to lend this to other institution or individuals for purposes of academic research only. Honour M.M Sinampande …………………………………………… 2016 DEDICATION This work is dedicated to my father Mr. H.M Sinampande and my mother Ms. J. Muleya for their inspiration, love and financial support throughout my four year degree programme. ABSTRACT The history of the Tonga have it that, the introduction of the fishing villages initially and then later the cooperative system in Binga District from the 1950s-2015 saw the Zambezi Tonga lose their fishing rights. -

SOCIAL ENTERPRISE AS the GAME-CHANGER: EMBRACING INNOVATION and DYNAMISM in CONTEMPORARY SOCIAL WORK PRACTICE in ZIMBABWE Rangarirai Franka & Zororo Murandab
________________________________________________________________________________________________________________ AJSW, Volume 6 Number 1 2016 Frank, R. & Muranda, Z. Publisher African Journal of Social Work Afri. j. soc. work © National Association of Social Workers-Zimbabwe/Author(s) ISSN Print 1563-3934 ISSN Online 2409-5605 Licensed under a Creative Commons Attribution-Non-commercial 4.0 International License SOCIAL ENTERPRISE AS THE GAME-CHANGER: EMBRACING INNOVATION AND DYNAMISM IN CONTEMPORARY SOCIAL WORK PRACTICE IN ZIMBABWE Rangarirai Franka & Zororo Murandab ABSTRACT The integration of economic and social value creation through social entrepreneurship has become a global phenomenon. Only recently, social work practitioners, researchers, and academics have begun to explore social entrepreneurship including its significance to social work practice. This paper discusses social enterprise as an innovative and dynamic approach to social work practice which addresses complex societal challenges within a constrained but constantly changing environment. Since social entrepreneurship embraces the application of business acumen to raise income for the purposes of supporting a social mission, its application to social work practice in Zimbabwe’s voluntary sector has become indispensable, given the dwindling state and donor funds to support and sustain social services delivery. The paper underscores that since social enterprise is premised on a culture of innovation, openness and adaption, it represents a hands-on approach to sustainable -

The Political Ecology of Poverty Alleviation in Zimbabwe's Communal Areas Management Programme for Indigenous Resources CAMPFIRE) B
Geoforum 33 2002) 1±14 www.elsevier.com/locate/geoforum The political ecology of poverty alleviation in Zimbabwe's Communal Areas Management Programme for Indigenous Resources CAMPFIRE) B. Ikubolajeh Logan a, William G. Moseley b a Department of Geography, University of Georgia, Athens, GA 30602-2502, USA b Department of Geography, Northern Illinois University, Dekalb, IL 60115-2854, USA Received 13 November 2000; in revised form 25 June 2001 Abstract The CAMPFIRE program in Zimbabwe is one of a `new breed' of strategies designed to tackle environmental management at the grassroots level. CAMPFIRE aims to help rural communities to manage their resources, especially wildlife, for their own local development. The program's central objective is to alleviate rural poverty by giving rural communities autonomy over resource management and to demonstrate to them that wildlife is not necessarily a hindrance to arable agriculture, ``but a resource that could be managed and `cultivated' to provide income and food''. In this paper, we assess two important elements of CAMPFIRE: poverty alleviation and local empowerment and comment on the program's performance in achieving these highly interconnected objectives. We analyze the program's achievements in poverty alleviation by exploring tenurial patterns, resource ownership and the allocation of proceeds from resource exploitation; and its progress in local empowerment by examining its administrative and decision making structures. We conclude that the program cannot eectively achieve the goal of poverty alleviation without ®rst addressing the administrative and legal structures that underlie the country's political ecology. Ó 2001 Elsevier Science Ltd. All rights reserved. Keywords: Political ecology; Poverty alleviation; Community-empowerment; CAMPFIRE 1. -

Case Studies on Successful Southern African NRM Initiatives and Their
CASE STUDIES ON SUCCESSFUL SOUTHERN AFRICAN NRM INITIATIVES AND THEIR IMPACTS ON POVERTY AND GOVERNANCE CASE STUDY: CAMPFIRE (COMMUNAL AREAS MANAGEMENT PROGRAMME FOR INDIGENOUS RESOURCES), ZIMBABWE April 2006 This publication was produced for review by the United States Agency for International Development. It was prepared by RD Taylor for International Resources Group (IRG). CASE STUDIES ON SUCCESSFUL SOUTHERN AFRICAN NRM INITIATIVES AND THEIR IMPACTS ON POVERTY AND GOVERNANCE CASE STUDY: CAMPFIRE (COMMUNAL AREAS MANAGEMENT PROGRAMME FOR INDIGENOUS RESOURCES), ZIMBABWE This project was funded by USAID-FRAME and implemented by the IUCN-TPARI (Trans-boundary Protected Areas Research Initiative). IUCN-TPARI is funded through the Centre for Integrated Study of the Human Dimensions of Global Change, by way of a cooperative agreement with the National Science Foundation (I-9521914). International Resources Group IUCN South Africa Country 1211 Connecticut Avenue, NW, Office Suite 700 P.O. Box 11536, Hatfield Washington, DC 20036 Pretoria, 0028 202-289-0100 Fax 202-289-7601 Tel: +27 12 342-8304/5/6 www.irgltd.com Fax: +27 12 342-8289 www.iucnsa.org.za DISCLAIMER The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. ACRONYMS AA Appropriate Authority CAMPFIRE Communal Areas Management Programme for Indigenous Resources CA CAMPFIRE Association CASS Centre for Applied Social Sciences CBNRM Community Based Natural Resource Management -

ZIMBABWEAN GOVERNMENT GAZETTE Published by Authority
ZIMBABWEAN GOVERNMENT GAZETTE Published by Authority Vol. XCIX, No. 60 21st MAY, 2021 Price RTGS$155,00 General Notice 974 of 2021. Bidding documents are available at Chipinge Town Council offices upon payment of a non-refundable tender fee of CHAMINUKA RURAL DISTRICT COUNCIL ZW$800,00, for each document. Tenders in sealed envelopes clearly marked with tender number Invitation to Competitive Bidding must be hand delivered or couriered to the undermentioned address before the closing date and time shown. TENDERS are invited from reputable and registered companies for the supply of the following: The Acting Town Secretary, Chipinge Town Council, Tender number Stand No. 281, Emmerson Dambudzo Mnangagwa Street, CRDC.06/2021. Supply and delivery of building materials. Closing PO. Box 90, date: 1st June, 2021. Chipinge. CRDC.07/2021. Supply and delivery of a borehole drilling rig. Tel: 027-2653/2734/2858/3239/3321 Quantity: 1. Closing date: 1st June, 2021. Email: [email protected] CRDC.08/2021. Supply, installation and configuration of wide area General Notice 976 of 2021. network. Site visit date: 2nd June, 2021. Closing date: 10th June, 2021. NYANGA RURAL DISTRICT COUNCIL Tender conditions Invitation to Competitive Bidding 1. Tender document must be obtained upon payment of a non-refundable fee of ZWL$800,00, from Chaminuka Rural District Council, Adams Plot Offices, Shamva or NYANGA Rural District Council is inviting bids from reputable bidders registered with Procurement Regulatory Authority of upon written request to pmu.chaminukardc@gmail. Zimbabwe to participate in the following tender: com Tender number 2. Tenders must be enclosed in sealed envelopes and endorsed on the outside with advertised tender number NRDC.02/2021. -

ADRA Zimbabwe News Flash March 2013 6.Pdf
Number 1, 2013 ADRA Zimbabwe N e w s F l a s h FOOD SECURITY PROJECT IN PARTNERSHIP WITH FOOD AND AGRICULTURE ORGANIZATION ADRA Zimbabwe Launched a food security project on the 5th of October, 2012 in Binga and Bulilima Districts. The project at improving agricultural production, food and nutri- tion and income security for 5000 vulnerable and emerging smallholder farmers in Zimbabwe. This is being achieved through the distribution of agricultural input (both crop and livestock) and output market, capacity building for the farmers and extension support. This project is funded by Australia Aid, UKAID and Department for International Department (DFID) through Food and Agriculture Organization (FAO) to the tune of $915,000 including commodities. ADRA Inter- national is also co-financing some elements of the project to the total of $5500. From the 29th January to the 6th of Feb- The bigger livestock that was being sold at the livestock fair ruary 2013 livestock fairs have been held in Binga and Bu- in Bulilima District lilima to enable farmers to buy livestock as a way of restock- ing as most of the livestock had died from the drought or were sold to purchase food and pay school fees. Livestock is also preferred in this semi- “...Am very arid part of the country as it mitigates impacts happy I now of crop failure on vulnerable households. own Beneficiaries contributed US$32 and the pro- livestock...” gram provided US$128 to the farmers in form of vouchers for agricultural input and livestock. In Bulilima District farmers put their vouchers together to purchase bigger livestock like donkeys and cattle. -

Zimbabwe Livelihood Zone Profiles. December 2010
Zimbabwe Livelihoods Zone VAC ZIMBABWE Profiles Vulnerability Assessment Committee 15 February 2010 The Zimbabwe Vulnerability Assessment Committee (ZimVac) is Chaired by the Food and Nutrition Council (FNC) which is housed at the Scientific Industrial Research and Developing Council (SIRDC), Harare, Zimbabwe. Acknowledgements The Zimbabwe Vulnerability Assessment Committee (ZimVac) would like to express its appreciation for the financial, technical and logistical support that the following agencies provided towards the data collection, analysis and writing-up of the Revised Livelihoods profiles for Zimbabwe; Ministry of Agriculture, Irrigation Development and Mechanizations’ Department of Agricultural Extension Services (AGRITEX) Ministry of Labour and Social Welfare’s Department of Social Welfare Ministry of Finance’s Central Statistical Office (CSO) Ministry of Education’s Curriculum Development Ministry of Transport’s Department of Meteorological Services United Nations’ World Food Programme (WFP) United Nations’ Food and Agriculture Organization (FAO) United Nations’ Office of Coordination of Humanitarian Affairs (OCHA) World Vision (WV) OXFAM ACTIONAID Save the Children United Kingdom (SC-UK) Southern Africa Development Community Regional Vulnerability Assessment Committee (RVAC) United States of America International Development Agency (USAID) Department for International Development (DFID) The European Commission (EC) FEG (The Food Economy Group) The Famine Early Warning Systems Network (FEWSNET) The revision -

Rebirth of Bukalanga: a Manifesto for the Liberation of a Great People with a Proud History Part I
THE REBIRTH OF BUKALANGA A Manifesto for the Liberation of a Great People with a Proud History Part I NDZIMU-UNAMI EMMANUEL 2 The Rebirth of Bukalanga: A Manifesto for the Liberation of a Great People with a Proud History Part I ISBN: 978 0 7974 4968 8 ©Ndzimu-unami Emmanuel, 2012 Facebook: Ndzimu-unami Emmanuel Email: [email protected] Twitter: NdzimuEmmanuel Website: http://www.ndzimuunami.blogspot.com Published by Maphungubgwe News Corporation Language Editing and Proof-reading Pathisa Nyathi Bheki J. Ncube Cover Design Greg Sibanda, Tadbagn Designs All rights reserved. Not more than one chapter of this publication maybe reproduced, stored in a retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopying, recording, or otherwise without prior permission in writing of the author or publisher, nor be otherwise circulated in any form of binding or cover other than that in which it is published and without a similar condition including this condition being imposed on the subsequent purchaser. 3 About the author Born on 29 March 1982 in Bulawayo and raised by his grandparents in the District of Bulilima-Mangwe, Ndzimu-unami Emmanuel Moyo completed his primary and secondary education at Tokwana Primary and Secondary Schools. He later completed a Diploma in Personnel Management graduating with Distinction with the Institute of People Management (IPMZ). Moyo later entered the Theological College of Zimbabwe (TCZ) in Bulawayo where he majored in reading Theology and Philosophy, dropping out of the College after one-and-a-half- years. Between the time of his finishing of the GCE Ordinary Level in 1999 and publishing this book in 2012, Moyo worked for the Zimbabwe postal service, Zimbabwe Posts, and the National Oil Company of Zimbabwe (Noczim) in his home town of Plumtree. -

IN "CAMPFIRE" Steve J. Thomas. Paper Prepared for the Second
THE LEGACY OP DUALISM AND DECISION —MAKING: THE PROSPECTS FOR LOCAL INSTITUTIONAL DEVELOPMENT IN "CAMPFIRE" Steve J. Thomas. Paper prepared for the Second Annual Conference of the International Association for the Study of Common Property (IASCP) held at University of Manitoba, Winnipeg, Canada. September 26 - 29, 1991. THE LEGACY Of DUALISM AND DECISION—MAKING: the prospects for local institutional development in "CAMPFIRE". Steve J. Thomas. Abstract 'CAMPFIRE' is Zimbabwe's 'Communal Areas Management Programme for Indigenous Resources'. It seeks to place the management of the wildlife in communal lands into the hands of those communities intimately affected by it. Much of the communal lands is a marginal environment to which the majority of the African population was relocated under divisive legislation introduced by the colonial powers. Parallels are drawn between the colonial and post-colonial periods; the legacy of dualism providing the context within which the prospects for institutional development are discussed. The fugitive nature of the resource suggests the determination of jurisdictional boundaries within which appropriate institutions might function is problematical. Moreover, the 'costs' incurred in 'producing' wildlife must be more than compensated by the benefits accruing from its utilisation. How these benefits are distributed must be decided by 'producer communities' themselves. The success of 'CAMPFIRE' will hinge on the will of central government to decentralise decision-making and control over wildlife resources to local communities, and the willingness and capacity of rural communities to adopt and further this concept of devolution. The legitimacy of the local institutional arrangements which develop will be critical to this success. * Institutional Development Manager with the Zimbabwe Trust, P.O.Box 4027, 4 Lanark Road, Harare, Zimbabwe. -

Health Cluster Bulletin 11Ver2
Zimbabwe Health Cluster bulletin Bulletin No 11 1-15 April 2009 Highlights: Cholera outbreak situation update • About 96, 473 cases and 4,204 deaths, CFR 4.4% Following a 9 week decline trend in cholera cases, an upsurge was reported during epidemi- • Sustained decline of ological week 15. Batch reporting in three districts may have contributed to this slight in- the outbreak crease. • Cholera hotspots in The cumulative number of Mashonaland west, Cholera in Zimbabwe reported cholera cases was Harare and Chitungwiza 17 Aug 08 to 11th April 09 96, 473 and 4204 deaths with 10,000 cities cumulative Case Fatality Rate 8,000 Cases Deaths (CFR) as of 4.4 as of 15 April. During week 15, a 17% de- 6,000 crease in cases and 5% in- 4,000 crease in deaths was re- Number ported. The crude CFR is 2.7% 2,000 compared to 2.9% of week 14 0 while the I-CFR is 1.8% com- pared to 2.7% of week 14. The w2 w4 w6 w8 w36 w38 w40 w42 w44 w46 w48 w50 w52 w10 w12 w14 CFR has been steadily de- weeks clined although the proportion of deaths in health facilities has increased compared to Cholera in Zimbabw e from 16 Nov 08 to 11th A pril 09 those reported in the commu- W eekly c rude and institutional c ase-fatality ratios 10 nity. CFR 9 This is probably an indication Inside this issue: 8 iCFR 7 of more people accessing 6 treatment and/or the increas- Cholera situation 1 5 ing role of other co- 4 morbidities presenting along- ORPs in cholera 2 3 management percent side cholera.