GEOGRAPHICAL ASSOCIATION of ZIMBABWE
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Issue Number 1, 2016
Issue Number 1, 2016 A sub-regional UNESCO-ICH project Supported by the Flanders Government SAICH NEWS Senior officials, consultants and coordinators of the SAICH Platform Prof. David J. Simbi Mr. Damir Dijakovic Dr. Thokozile Chitepo Vice Chancellor, Regional Cultural Advisor, Permanent Secretary, Ministry of Rural Development, Promotion and Preservation Chinhoyi University of UNESCO Regional Office of National Cultural Heritage, Zimbabwe Technology for Southern Africa Mr. Stephen Chifunyise Dr. Marc Jacobs Mr. Lovemore Mazibuko UNESCO ICH Expert/ UNESCO ICH Expert/ UNESCO ICH Expert/ Consultant Flanders Government Consultant Representative Prof. Herbert Chimhundu Prof. Jacob Mapara Dr. Manase K. Chiweshe Coordinator Associate Coordinator Associate Coordinator SAICH Platform SAICH Platform SAICH Platform Editor-in-Chief Cover Page Professor Herbert Chimhundu Event: Great Limpopo Cultural Trade Fair, Location: Boli Muhlanguleni, Editor Chiredzi, Zimbabwe, Photograph by: Mr. Eugene Ncube Professor Jacob Mapara Contacts Contributors SAICH Platform Dr Manase K. Chiweshe Chinhoyi University of Technology Ms Varaidzo Chinokwetu P. Bag 7724, Ms Jacqueline Tanhara Chinhoyi Design Off Harare-Kariba Highway Mr. Eugene Ncube Zimbabwe Printing Telephone: +2636727496 CUT Printing Press E-mail: [email protected] | [email protected] SAICH NEWS SAFEGUARDING SAICH NEWS Participating Countries ParticipatingParticipating Countries Countries Participating Countries ParticipatingParticipatingParticipating CountriesCountries Countries BotswanaParticipatingBotswana -

Midlands Province Mobile Voter Registration Centres
Midlands Province Mobile Voter Registration Centres Chirumhanzu District Team 1 Ward Centre Dates 18 Mwire primary school 10/06/13-11/06/13 18 Tokwe 4 clinic 12/06/13-13/06/13 18 Chingegomo primary school 14/06/13-15/06/13 16 Chishuku Seondary school 16/06/13-18/06/13 9 Upfumba Secondary school 19/06/13-21/06/13 3 Mutya primary school 22/06/13-24/06/13 2 Gonawapotera secondary school 25/06/13-27/06/13 20 Wildegroove primary school 28/06/13-29/06/13 15 Kushinga primary school 30/06/13-02/07/13 12 Huchu compound 03/07/13-04/-07/13 12 Central estates HQ 5/7/13 20 Mtao/Fair Field compound 6/7/13 12 Chiudza homestead 07/07/13-08/06/13 14 Njerere primary school 9/7/13 Team 2 Ward Centre Dates 22 Hillview Secondary school 10/07/13-12/07/13 17 Lalapanzi Secondary school 13/07/13-15/07/13 16 Makuti homestead 16/06/13-17/06/13 1 Mapiravana Secondary school 18/06/13-19/06/13 9 Siyahukwe Secondary school 20/06/13-23/06/13 4 Chizvinire primary school 24/06/13-25/06/13 21 Mukomberana Seconadry school 26/06/13-29/06/13 20 Union primary school 30/06/13-01/07/13 15 Nyikavanhu primary school 02/07/13-03/07/13 19 Musens primary school 04/07/13-06/07/13 16 Utah primary school 07/7/13-09/07/13 Team 3 Ward Centre Dates 11 Faerdan primary school 10/07/13-11/07/13 11 Chamakanda Secondary school 12/07/13-14/07/13 11 Chamakanda primary school 15/07/13-16/07/13 5 Chizhou Secondary school 17/06/13-16/06/13 3 Chilimanzi primary school 21/06/13-23/06/13 25 Maponda primary school 24/06/13-25/06/13 6 Holy Cross seconadry school 26/06/13-28/06/13 20 New England Secondary -

(Ports of Entry and Routes) (Amendment) Order, 2020
Statutory Instrument 55 ofS.I. 2020. 55 of 2020 Customs and Excise (Ports of Entry and Routes) (Amendment) [CAP. 23:02 Order, 2020 (No. 20) Customs and Excise (Ports of Entry and Routes) (Amendment) “THIRTEENTH SCHEDULE Order, 2020 (No. 20) CUSTOMS DRY PORTS IT is hereby notifi ed that the Minister of Finance and Economic (a) Masvingo; Development has, in terms of sections 14 and 236 of the Customs (b) Bulawayo; and Excise Act [Chapter 23:02], made the following notice:— (c) Makuti; and 1. This notice may be cited as the Customs and Excise (Ports (d) Mutare. of Entry and Routes) (Amendment) Order, 2020 (No. 20). 2. Part I (Ports of Entry) of the Customs and Excise (Ports of Entry and Routes) Order, 2002, published in Statutory Instrument 14 of 2002, hereinafter called the Order, is amended as follows— (a) by the insertion of a new section 9A after section 9 to read as follows: “Customs dry ports 9A. (1) Customs dry ports are appointed at the places indicated in the Thirteenth Schedule for the collection of revenue, the report and clearance of goods imported or exported and matters incidental thereto and the general administration of the provisions of the Act. (2) The customs dry ports set up in terms of subsection (1) are also appointed as places where the Commissioner may establish bonded warehouses for the housing of uncleared goods. The bonded warehouses may be operated by persons authorised by the Commissioner in terms of the Act, and may store and also sell the bonded goods to the general public subject to the purchasers of the said goods paying the duty due and payable on the goods. -
MIDLANDS STATE UNIVERSITY APPROVAL FORM The
MIDLANDS STATE UNIVERSITY APPROVAL FORM The undersigned certify that they have supervised, read and recommend to the Midlands State University for acceptance of dissertation entitled: Violation of Children `s rights by Varemba cultural practise in Mberengwa District 1980-2013 submitted by Nokuthula Bula-Bula in partial fulfillment of the requirements for the Bachelor of Arts in History and International studies Honours Degree Signature of Student........................................................................................................................... Signature of Supervisor...................................................................................................................... Signature of the Chairperson............................................................................................................. Signature of the Examiner(s)............................................................................................................. 1 DECLARATION I, Bula-bula Nokuthula (R103446R), certify that this dissertation submitted in partial fulfillment of the requirement for the Bachelor of Arts honours degree in History and International Studies at Midlands State University has not been submitted for a degree at any other University, and that it is entirely my work. Student’s name Nokuthula.L Bula-Bula Signature ……………………………… Date ........../......../............ 2 ACKNOWLEDGEMENT I would like to thank the almightys God who gave me the wisdom and knowledge to accomplish the work. My appreciation is -

CHAPTER 10: Restructuring and Recovery in Railway Services
CHAPTER 10: Restructuring and Recovery in Railway Services 10.1 OVERVIEW OF Republic of Congo (DRC) (See Map 10.1). THE SECTOR As a result, the national railway of Zimbabwe has been critical to the growth of the country’s domestic, regional, and international trade as 10.1.1 The Setting it connects all major economic centers and Although continental rail master plans have provides transport for bulk raw materials, existed for more than a century, most of the fi nished goods, and passengers. As in most African railway network remains disconnected, other African countries, the Zimbabwean operating within a single country, or linking railway system served as a primary conduit a port and its immediate regional hinterland. for agricultural and other natural resources The only signifi cant international network is and this largely accounts for the standards and centered in South Africa and stretches north routing that were adopted. to Zimbabwe, Zambia, and the Democratic Map 10.1: Railway Network for the Southern Africa Region Within Zimbabwe, the railway network and its ports of Durban, Richards Bay, and Port connects all major mines and heavy industrial Elizabeth. It is also at the centre of shorter and plants, as well as major collection points for cost-effective railroad links between Malawi farms. The system has three well connected and South Africa through Bulawayo, the port hubs, Bulawayo, Gweru, and Harare (See of Beira through Harare, and Lusaka and the Map 10.2). The railway is at the centre of the port of Durban through Bulawayo. The -

The Spatial Dimension of Socio-Economic Development in Zimbabwe
THE SPATIAL DIMENSION OF SOCIO-ECONOMIC DEVELOPMENT IN ZIMBABWE by EVANS CHAZIRENI Submitted in fulfillment of the requirements for the degree of MASTER OF ARTS in the subject GEOGRAPHY at the UNIVERSITY OF SOUTH AFRICA SUPERVISOR: MRS AC HARMSE NOVEMBER 2003 1 Table of Contents List of figures 7 List of tables 8 Acknowledgements 10 Abstract 11 Chapter 1: Introduction, problem statement and method 1.1 Introduction 12 1.2 Statement of the problem 12 1.3 Objectives of the study 13 1.4 Geography and economic development 14 1.4.1 Economic geography 14 1.4.2 Paradigms in Economic Geography 16 1.4.3 Development paradigms 19 1.5 The spatial economy 21 1.5.1 Unequal development in space 22 1.5.2 The core-periphery model 22 1.5.3 Development strategies 23 1.6 Research design and methodology 26 1.6.1 Objectives of the research 26 1.6.2 Research method 27 1.6.3 Study area 27 1.6.4 Time period 30 1.6.5 Data gathering 30 1.6.6 Data analysis 31 1.7 Organisation of the thesis 32 2 Chapter 2: Spatial Economic development: Theory, Policy and practice 2.1 Introduction 34 2.2. Spatial economic development 34 2.3. Models of spatial economic development 36 2.3.1. The core-periphery model 37 2.3.2 Model of development regions 39 2.3.2.1 Core region 41 2.3.2.2 Upward transitional region 41 2.3.2.3 Resource frontier region 42 2.3.2.4 Downward transitional regions 43 2.3.2.5 Special problem region 44 2.3.3 Application of the model of development regions 44 2.3.3.1 Application of the model in Venezuela 44 2.3.3.2 Application of the model in South Africa 46 2.3.3.3 Application of the model in Swaziland 49 2.4. -

Conference Paper Series
POLITICAL ECONOMY RESEARCH INSTITUTE University of Massachusetts Amherst Community Rights, Costs, and Benefits: The Question of Natural Resource Stewardship and Community Benefits in Zimbabwe’s CAMPFIRE Program James C. Murombedzi January 2003 CONFERENCE PAPER SERIES No. 16 Committees, Rights, Costs and Benefits: The Question of Natural Resource Stewardship and Community Benefits in Zimbabwe’s CAMPFIRE Program James C. Murombedzi The Ford Foundation Johannesburg, South Africa 1 In the CAMPFIRE formulation, the resource management problems obtaining in the communal areas of Zimbabwe are the result of the absence of both the institutional capacity as well as the incentives to manage the resources in question. The CAMPFIRE solution, therefore, was to introduce new systems of group ownership and territorial rights to natural resources to communities, and provide the appropriate institutions for legitimate resource management for the benefit of these communities (Martin 1986). The implementation of this solution was attained through the enactment of an amendment to the Parks and Wild Life Act of 1975, which enables the government to delegate appropriate authority over the wildlife to the ‘communal representatives’. The CAMPFIRE program in fact constitutes a transfer of the notion of ownership, successfully implemented with regard to individual landowners, to communal landowners (Farquharson 1993). This chapter tests the extent to which CAMPFIRE has in fact been able to devolve ownership over wildlife to communities in the communal areas, and thereby promoted stewardship of wildlife through the production of benefits for the participating communities. To achieve this, I will proceed by first evaluating the extent to which CAMPFIRE has succeeded in eliciting stewardship of the wildlife resource by participating communities through the devolution of clear and unambiguous rights to wildlife to these communities. -

Turmoil in Zimbabwe's Mining Sector
All That Glitters is Not Gold: Turmoil in Zimbabwe’s Mining Sector Africa Report N°294 | 24 November 2020 Headquarters International Crisis Group Avenue Louise 235 • 1050 Brussels, Belgium Tel: +32 2 502 90 38 • [email protected] Preventing War. Shaping Peace. Table of Contents Executive Summary ................................................................................................................... i I. Introduction ..................................................................................................................... 1 II. The Makings of an Unstable System ................................................................................ 5 A. Pitfalls of a Single Gold Buyer ................................................................................... 5 B. Gold and Zimbabwe’s Patronage Economy ............................................................... 7 C. A Compromised Legal and Justice System ................................................................ 10 III. The Bitter Fruits of Instability .......................................................................................... 14 A. A Spike in Machete Gang Violence ............................................................................ 14 B. Mounting Pressure on the Mnangagwa Government ............................................... 15 C. A Large-scale Police Operation .................................................................................. 16 IV. Three Mines, Three Stories of Violence .......................................................................... -
LAN Installation Sites Coordinates
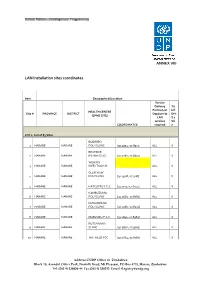
ANNEX VIII LAN Installation sites coordinates Item Geographical/Location Service Delivery Tic Points (List k if HEALTH CENTRE Site # PROVINCE DISTRICT Dept/umits DHI (EPMS SITE) LAN S 2 services Sit COORDINATES required e LOT 1: List of 83 Sites BUDIRIRO 1 HARARE HARARE POLYCLINIC [30.9354,-17.8912] ALL X BEATRICE 2 HARARE HARARE RD.INFECTIO [31.0282,-17.8601] ALL X WILKINS 3 HARARE HARARE INFECTIOUS H ALL X GLEN VIEW 4 HARARE HARARE POLYCLINIC [30.9508,-17.908] ALL X 5 HARARE HARARE HATCLIFFE P.C.C. [31.1075,-17.6974] ALL X KAMBUZUMA 6 HARARE HARARE POLYCLINIC [30.9683,-17.8581] ALL X KUWADZANA 7 HARARE HARARE POLYCLINIC [30.9285,-17.8323] ALL X 8 HARARE HARARE MABVUKU P.C.C. [31.1841,-17.8389] ALL X RUTSANANA 9 HARARE HARARE CLINIC [30.9861,-17.9065] ALL X 10 HARARE HARARE HATFIELD PCC [31.0864,-17.8787] ALL X Address UNDP Office in Zimbabwe Block 10, Arundel Office Park, Norfolk Road, Mt Pleasant, PO Box 4775, Harare, Zimbabwe Tel: (263 4) 338836-44 Fax:(263 4) 338292 Email: [email protected] NEWLANDS 11 HARARE HARARE CLINIC ALL X SEKE SOUTH 12 HARARE CHITUNGWIZA CLINIC [31.0763,-18.0314] ALL X SEKE NORTH 13 HARARE CHITUNGWIZA CLINIC [31.0943,-18.0152] ALL X 14 HARARE CHITUNGWIZA ST.MARYS CLINIC [31.0427,-17.9947] ALL X 15 HARARE CHITUNGWIZA ZENGEZA CLINIC [31.0582,-18.0066] ALL X CHITUNGWIZA CENTRAL 16 HARARE CHITUNGWIZA HOSPITAL [31.0628,-18.0176] ALL X HARARE CENTRAL 17 HARARE HARARE HOSPITAL [31.0128,-17.8609] ALL X PARIRENYATWA CENTRAL 18 HARARE HARARE HOSPITAL [30.0433,-17.8122] ALL X MURAMBINDA [31.65555953980,- 19 MANICALAND -

Midlands Province
School Province District School Name School Address Level Primary Midlands Chirumanzu BARU KUSHINGA PRIMARY BARU KUSHINGA VILLAGE 48 CENTAL ESTATES Primary Midlands Chirumanzu BUSH PARK MUSENA RESETTLEMENT AREA VILLAGE 1 MUSENA Primary Midlands Chirumanzu BUSH PARK 2 VILLAGE 5 WARD 19 CHIRUMANZU Primary Midlands Chirumanzu CAMBRAI ST MATHIAS LALAPANZI TOWNSHIP CHIRUMANZU Primary Midlands Chirumanzu CHAKA NDARUZA VILLAGE HEAD CHAKA Primary Midlands Chirumanzu CHAKASTEAD FENALI VILLAGE NYOMBI SIDING Primary Midlands Chirumanzu CHAMAKANDA TAKAWIRA RESETTLEMENT SCHEME MVUMA Primary Midlands Chirumanzu CHAPWANYA HWATA-HOLYCROSS ROAD RUDUMA VILLAGE Primary Midlands Chirumanzu CHIHOSHO MATARITANO VILLAGE HEADMAN DEBWE Primary Midlands Chirumanzu CHILIMANZI NYONGA VILLAGE CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHIMBINDI CHIMBINDI VILLAGE WARD 5 CHIRUMANZU Primary Midlands Chirumanzu CHINGEGOMO WARD 18 TOKWE 4 VILLAGE 16 CHIRUMANZU Primary Midlands Chirumanzu CHINYUNI CHINYUNI WARD 7 CHUKUCHA VILLAGE Primary Midlands Chirumanzu CHIRAYA (WYLDERGROOVE) MVUMA HARARE ROAD WASR 20 VILLAGE 1 Primary Midlands Chirumanzu CHISHUKU CHISHUKU VILAGE 3 CHIEF CHIRUMANZU Primary Midlands Chirumanzu CHITENDERANO TAKAWIRA RESETTLEMENT AREA WARD 11 Primary Midlands Chirumanzu CHIWESHE PONDIWA VILLAGE MAPIRAVANA Primary Midlands Chirumanzu CHIWODZA CHIWODZA RESETTLEMENT AREA Primary Midlands Chirumanzu CHIWODZA NO 2 VILLAGE 66 CHIWODZA CENTRAL ESTATES Primary Midlands Chirumanzu CHIZVINIRE CHIZVINIRE PRIMARY SCHOOL RAMBANAPASI VILLAGE WARD 4 Primary Midlands -

THE HISTORY of the TONGA and FISHING COOPERATIVES in BINGA DISTRICT 1950S-2015
FACULTY OF ARTS DEPARTMENT OF HISTORY EMPOWERMENT OR CONTROL? : THE HISTORY OF THE TONGA AND FISHING COOPERATIVES IN BINGA DISTRICT 1950s-2015 BY HONOUR M.M. SINAMPANDE R131722P DISSERTATION SUBMITTED TO THE FACULTY OF ARTS IN PARTIAL FULLFILMENT OF THE REQUIREMENTS OF THE HONOURS DEGREE IN HISTORY AT MIDLANDS STATE UNIVERSITY. NOVEMBER 2016 ZVISHAVANE: ZIMBABWE SUPERVISOR DR. T.M. MASHINGAIDZE APPROVAL FORM The undersigned certify that they have supervised the student Honour M.M Sinampande (R131722P) dissertation entitled Empowerment or Control? : The history of the Tonga and fishing cooperatives in Binga District 1950-210 submitted in partial fulfillment of the requirements of the Bachelor of Arts in History Honours Degree offered by Midlands State University. Dr. T.M Mashingaidze ……………………… SUPERVISOR DATE …….……………………………………… …………………………….. CHAIRPERSON DATE ….………………………………………… …………………………….. EXTERNAL EXAMINER DATE DECLARATION I, Honour M.M Sinampande declare that, Empowerment or Control? : The history of the Tonga and fishing cooperatives in Binga District 1950s-2015 is my own work and it has never been submitted before any degree or examination in any other university. I declare that all sources which have been used have been acknowledged. I authorize the Midlands State University to lend this to other institution or individuals for purposes of academic research only. Honour M.M Sinampande …………………………………………… 2016 DEDICATION This work is dedicated to my father Mr. H.M Sinampande and my mother Ms. J. Muleya for their inspiration, love and financial support throughout my four year degree programme. ABSTRACT The history of the Tonga have it that, the introduction of the fishing villages initially and then later the cooperative system in Binga District from the 1950s-2015 saw the Zambezi Tonga lose their fishing rights. -

Faculty of Arts Department of History And
FACULTY OF ARTS DEPARTMENT OF HISTORY AND INTERNATIONAL STUDIES RESOURCE NATIONALISM AND LOCAL EMPOWERMENT, THE CASE OF ZVISHAVANE COMMUNITY SHARE OWNERSIP TRUST, 2012 TO 2017. By FAITH MAFUNGA R147013M SUPERVISOR: DR T. MASHINGAIDZE A DISSERTATION SUBMITTED TO THE HISTORY DEPARTMENT OF THE MIDLANDS STATE UNIVERSITY IN PARTIAL FULFILMENT OF THE REQUIREMENTS OF THE BACHELOR OF ARTS IN HISTORY AND INTERNATIONAL STUDIES HONOURS DEGREE. ZVISHAVANE, ZIMBABWE JUNE 2018 Declaration I, Faith Mafunga declare that this dissertation hereby submitted for the Bachelor of Arts Honors Degree in History and International Studies at Midlands State University is my own effort. Information from published and unpublished work from other authors have been acknowledged. …………………………. ……………………………… Student Date i Approval form The undersigned certify that they have supervised and recommended to Midlands State University the student FAITH MAFUNGA dissertation entitled RESOURCE NATIONALISM AND LOCAL EMPOWERMENT, THE CASEOF ZVISHAVANE COMMUNITY SHARE OWNERSIP TRUST, 2012 TO 2017. The dissertation submitted in partial fulfillment of the requirements for the History and International Studies Department. …………………………. ……………………………… Supervisor Date …………………………… …………………………………. Chairperson Date …………………………. ……………………………………… External Examiner Date ii Dedication This piece of work is dedicated to my late father Mr. E.C Mafunga, my mother Mrs. E Mauto, my siblings Yvonne, Tanaka and Tafadzwa Mafunga. Thank you all for your constant love and support. God Bless you. iii Acknowledgements Utmost gratitude goes to God Almighty for he has been an unwavering source of strength throughout my academic years. I must pay tribute to my academic supervisor Doctor Mashingaidze who has given me supervision and motivation throughout this research. My exceptional gratefulness also goes to Mr. N.T Jinga the C.E.O of ZCSOT and the entire organization for helping me in crafting this dissertation.