Of M.D. M.R.C.P., Ed. Superintendent, Stirling District Asylum
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
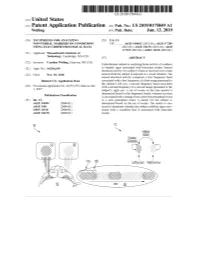
ANNNNNNNNNNNNNNNNNNNN 100A 006 Left Eye Input Right Eye Input
US 20190175049A1 ( 19) United States (12 ) Patent Application Publication (10 ) Pub. No. : US 2019 /0175049 A1 Welling ( 43 ) Pub . Date : Jun . 13 , 2019 ( 54 ) TECHNIQUES FOR ANALYZING (52 ) U . S . CI. NON -VERBAL MARKERS OF CONDITIONS CPC . .. A61B 5 /04842 (2013 . 01 ) ; A61B 5 / 7289 USING ELECTROPHYSIOLOGICAL DATA (2013 . 01) ; A61B 5 /0478 ( 2013 .01 ) ; A61B 5 /7225 ( 2013. 01 ) ; G06N 20 / 10 (2019 .01 ) (71 ) Applicant: Massachusetts Institute of Technology , Cambridge , MA (US ) ( 57 ) ABSTRACT (72 ) Inventor : Caroline Welling, Hanover, NH (US ) Embodiments related to analyzing brain activity of a subject to identify signs associated with binocular rivalry . Sensed ( 21 ) Appl. No. : 16 / 206, 639 electrical activity of a subject' s brain is received over a time period while the subject is exposed to a visual stimulus. The ( 22 ) Filed : Nov. 30 , 2018 sensed electrical activity comprises a first frequency band Related U . S . Application Data associated with a first frequency of a first image presented to the subject ' s left eye , a second frequency band associated (60 ) Provisional application No .62 / 593 , 535, filed on Dec . with a second frequency of a second image presented to the 1 , 2017 subject ' s right eye . A set of events in the time period is determined based on the frequency bands, wherein an event Publication Classification is associated with a change from a previous perceptual event (51 ) Int. Ci. to a new perceptual event. A metric for the subject is A61B 5 /0484 ( 2006 .01 ) determined based on the set of events . The metric is ana A61B 5 /00 ( 2006 .01 ) lyzed to determine whether the subject exhibits signs asso GO6N 20 / 10 (2006 .01 ) ciated with a condition that is associated with binocular A61B 5 /0478 ( 2006 .01 ) rivalry . -

Sulphonmethane, Sulphonal, Diethylsulpho
is a combination of amylene hydrate and chloral hydrate, superior to the corresponding compounds of other elements. while chloralose, a combination of chloral hydrate and glucose, Experience has shown that, in the main, these claims were un- partakes of the action of morphin and is rather expensive. founded, though many, even now, claim that strontium bro- Chloretone, a more recent product, is not entirely devoid of mid disturbs the stomach less than the corresponding sodium danger and is not always so certain in its action as chloral or potassium salt. Another claim that is frequently made by hydrate, while butyl chloral hydrate, or crotón chloral hydrate, manufacturers of nostrums, like "Peacock's Bromides," is that is one of the older compounds that has been found wanting and they use "chemically pure" salts. Exactly what is meant by is now little used. Of the official compounds of this group we this claim is difficult to say, but the Pharmacopeia gives us a have: number of readily applied tests by which the salts themselves Chloralamid and Paraldehyd. may be tested. The manufacturers of nostrums, on the other Chlobalformamidum.—TJ. S.—Chloralformamid. Chlorala- hand, not infrequently add the very substances that are consid- mid. This has practically the same action as therapeutic ered contaminations. doses of chloral hydrate, the latter being formed in the body by {To be continued.) decomposition of chloralformamid. Average dose: 1 gm. (15 grains). Paraldehtdum.—TJ. S.—Paraldehyd is slower in its action transparent liquid, slower in its action than chloral hydrate, but also safer. It has the disadvantage of a persistently dis- A NEW NEEDLE HOLDER. -

31V March 1891 — Insomnia As a Disease Per Se and As a Symp¬
SYMPTOMATIC A' N D IDIOPATHIC INSOMNIA. ITS ETIOLOGY AND TREATMENT. B Y GEORGE DOUGLAS GRAY, M.B. 00O00O00O00 — 31V March 1891 — Insomnia as a disease per se and as a symp¬ tom of many diseases I have chosen as the subject of this thesis for several reasons. I have suffered . much from it myself and consequently have examined with more than ordinary clinical interest every case that has come under my notice, and in addition I have j found that, with the exception of odd notes in the medical journals, the literature on this subj.ect is comparatively rare. During this last half century since the introduction of steam power, and follov/lng it , the I "telegraph, electricity in its numerous forms, not to mention countless other time-saving devices, and with - an ever increasing population, competition or the race for life has become keener than at any " previoxis time, j -. : <■ , •- : 'V ■ " ■ ■ . - I The average human being lives at a very high pressure,! and this struggle for existence, with its concomitant 1 worries, has of late made Insomnia a much more fre¬ quent complaint than before. Indeed, in several of the older text-books on Practice of Physic (e.g. that of Dr. Hughes Bennet, published as lately as 1853) the subject is not even mentioned. In order to work well we must eat well and sleep well: loss of appet¬ ite and lowering of all bodily functions soon follow loss of sleep,therefore all the more important is it that the etiology and treatment of Insomnia should be thoroughly understood. -

Yasakli Maddeler
YASAKLI MADDELER Ülkemizde yarış atlarında kullanılan/kullanılma ihtimali olan ilaçların/maddelerin belirlenmesinde; ilacın farmakolojisi (öncelikle etkisi, etki grubu), farmasötik şekli, kullanılma yolu, kullanılma alanı, yarış sonucunu etkileme durumu, ulusal mevzuata göre veteriner hekimlikte ve/veya yarış atlarında kullanmak için ruhsatlı/izinli olup-olmama durumu, etiket-dışı kullanılma gibi hususlar dikkate alınmıştır. Eşik değeri (Threshold level) olan maddelerin (vücutta şekillenirler, çevre ve yem kaynaklı olabilirler) miktarı, belirlenen miktarı aştığında yasaklı-madde kullanılması/doping ihlali olarak değerlendirilir. Tedavide kullanılan/tarama limiti (Screening level) olan maddelerle ilgili değerlendirmede; bu maddelerle ilgili olarak yapılan doping analizlerinde ölçülen miktar, idrarda/plazmada belirlenen tarama değerini aştığında yasaklı madde kullanılması/doping-ihlali olarakdeğerlendirilir. Ana madde yanında, izomeri, metaboliti, metabolit izomeri, tuzları, esterleri, eterleri, diğer türevleri, ön-ilaç da yasaklı-madde listesinde yer alır; doping analizinde ortaya konulmaları doping ihlali olarak değerlendirilir. Maddeler ve yasaklı uygulamalar 6 başlık altında toplanmıştır. Bu liste ilgili uluslararası kuruluşların mevzuat ve düzenlemeleri ile ilgili maddelerin Farmakolojik özellikleri ve etkileri dikkate alınarak hazırlanmıştır. 1. YasaklıMaddeler Yasaklı maddeler; yarış atlarında tıbbi olarak kullanım yeri olmayan, atın yarış performansını açık şekilde etkileyen maddelerdir. İllegal kullanılan maddeler (Türkiye’de veteriner -
Toward Refined Theoretical Models for the Description of Lipophilicity in Biomolecules
Toward Refined Theoretical Models for the Description of Lipophilicity in Biomolecules William J. Zamora Ramírez ADVERTIMENT. La consulta d’aquesta tesi queda condicionada a l’acceptació de les següents condicions d'ús: La difusió d’aquesta tesi per mitjà del servei TDX (www.tdx.cat) i a través del Dipòsit Digital de la UB (diposit.ub.edu) ha estat autoritzada pels titulars dels drets de propietat intel·lectual únicament per a usos privats emmarcats en activitats d’investigació i docència. No s’autoritza la seva reproducció amb finalitats de lucre ni la seva difusió i posada a disposició des d’un lloc aliè al servei TDX ni al Dipòsit Digital de la UB. No s’autoritza la presentació del seu contingut en una finestra o marc aliè a TDX o al Dipòsit Digital de la UB (framing). Aquesta reserva de drets afecta tant al resum de presentació de la tesi com als seus continguts. En la utilització o cita de parts de la tesi és obligat indicar el nom de la persona autora. ADVERTENCIA. La consulta de esta tesis queda condicionada a la aceptación de las siguientes condiciones de uso: La difusión de esta tesis por medio del servicio TDR (www.tdx.cat) y a través del Repositorio Digital de la UB (diposit.ub.edu) ha sido autorizada por los titulares de los derechos de propiedad intelectual únicamente para usos privados enmarcados en actividades de investigación y docencia. No se autoriza su reproducción con finalidades de lucro ni su difusión y puesta a disposición desde un sitio ajeno al servicio TDR o al Repositorio Digital de la UB. -

International Classification of Diseases
INTERNATIONAL CLASSIFICATION OF DISEASES MANUAL OF THE INTERNATIONAL STATISTICAL CLASSIFICATION OF DISEASES, INJURIES, AND CAUSES OF DEATH Based on the Recommendations of the Eighth Revision Conference, 1965, and Adopted by the Nineteenth World Health Assembly Volume 2 ALPHABETICAL INDEX WORLD HEALTH ORGANIZATION GENEVA 1969 Volume 1 Introduction List of Three-digit Categories Tabular List of Inclusions and Four-digit Sub- categories Medical Certification and Rules for Classification Special Lists for Tabulation Definitions and Recommendations Regulations Volume 2 Alphabetical Index PRINTED IN ENGLAND CONTENTS Introduction Page General arrangement of the Index ....................................... VIII Main sections ............................................................... VIII Structure ..................................................................... IX Code numbzrs .............................................................. x Primary and secondary conditions. ................................... x Multiple diagnoses. ........................................................ XI Spelling....................................................................... XI Order of listing ............................................................. Conventions used in the Index ........................................... XII Parentheses. ................................................................. XII Cross-referexes ........................................................... XI1 Abbreviation NEC. ...................................................... -

Protecting Mental Health in the Age of Anxiety: the Context of Valium's Development, Synthesis, and Discovery in the United States, to 1963 Catherine (Cai) E
Iowa State University Capstones, Theses and Graduate Theses and Dissertations Dissertations 2009 Protecting mental health in the Age of Anxiety: The context of Valium's development, synthesis, and discovery in the United States, to 1963 Catherine (cai) E. Guise-richardson Iowa State University Follow this and additional works at: https://lib.dr.iastate.edu/etd Part of the History Commons Recommended Citation Guise-richardson, Catherine (cai) E., "Protecting mental health in the Age of Anxiety: The onc text of Valium's development, synthesis, and discovery in the United States, to 1963" (2009). Graduate Theses and Dissertations. 10574. https://lib.dr.iastate.edu/etd/10574 This Dissertation is brought to you for free and open access by the Iowa State University Capstones, Theses and Dissertations at Iowa State University Digital Repository. It has been accepted for inclusion in Graduate Theses and Dissertations by an authorized administrator of Iowa State University Digital Repository. For more information, please contact [email protected]. Protecting mental health in the Age of Anxiety: The context of Valium’s development, synthesis, and discovery in the United States, to 1963 by Catherine (Cai) Guise-Richardson A dissertation submitted to the graduate faculty in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY Major: History of Technology and Science Program of Study Committee: Hamilton Cravens, Co-Major Professor Alan I Marcus, Co-Major Professor Amy Sue Bix Charles Dobbs David Wilson Iowa State University Ames, Iowa 2009 Copyright © Catherine (Cai) Guise-Richardson, 2009. All rights reserved. ii TABLE OF CONTENTS LIST OF TABLES iv ABSTRACT v CHAPTER 1. -

Modern Surgery, 4Th Edition, by John Chalmers Da Costa Rare Medical Books
Thomas Jefferson University Jefferson Digital Commons Modern Surgery, 4th edition, by John Chalmers Da Costa Rare Medical Books 1903 Modern Surgery - Chapter 23. Diseases and Injuries of the Head John Chalmers Da Costa Jefferson Medical College Follow this and additional works at: https://jdc.jefferson.edu/dacosta_modernsurgery Part of the History of Science, Technology, and Medicine Commons Let us know how access to this document benefits ouy Recommended Citation Da Costa, John Chalmers, "Modern Surgery - Chapter 23. Diseases and Injuries of the Head" (1903). Modern Surgery, 4th edition, by John Chalmers Da Costa. Paper 29. https://jdc.jefferson.edu/dacosta_modernsurgery/29 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in Modern Surgery, 4th edition, by John Chalmers Da Costa by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Diseases of the Head 595 XXIII. DISEASES AND INJURIES OF THE HEAD. I. DISEASES OF I:: HEAD. IN approaching a case of brain disorder, first endeavor to locate the seat of the trouble; next, ascertain the nature of the lesion; and, finally, deter- mine the best plan of treatment, operative or otherwise. -

Federal Register Volume 31 • Number 182
FEDERAL REGISTER VOLUME 31 • NUMBER 182 Tuesday, September 20, 1966 • Washington, D.C. Pages 12427-12470 Agencies in this issue—• Atomic Energy Commission Civil Aeronautics Board Civil Service Commission Comptroller of the Currency Consumer and Marketing Service Defense Department Engineers Corps Federal Aviation Agency Federal Maritime Commission Federal Power Commission Federal Trade Commission Fish and Wildlife Service Food and Drug Administration General Services Administration International Commerce Bureau Interstate Commerce Commission Land Management Bureau National Bureau of Standards Post Office Department Reclamation Bureau Securities and Exchange Commission Wage and Hour Division Detailed list of Contents appears- inside. Latest Edition Guide to Record Retention Requirements [Revised as of January 1, 1966] This useful reference tool is designed keep them, and (3) how long they to keep industry and the general must be kept. Each digest also public informed concerning published includes a reference to the full text requirements in laws and regulations of the basic law or regulation govern relating to records-retention. It corn- ing such retention. tains over 900 digests detailing the retention periods for the many types of records required to be kept under The booklet’s index, numbering over Federal laws and rules. 2,000 items, lists for ready reference the categories of persons, companies, The “Guide” tells the user (1) what and products affected by Federal records must be kept, (2) who must record-retention requirements. Price; 40 cents Compiled by Office of the Federal Register, Nati onal Archives and Records Service, General Services Admi nistration * Order from Superintendent of Documents, U.S. Government Printing Office Washington, D.C. -

The Many Faces of Apomorphine: Lessons from the Past and Challenges for the Future
Drugs R D (2018) 18:91–107 https://doi.org/10.1007/s40268-018-0230-3 REVIEW ARTICLE The Many Faces of Apomorphine: Lessons from the Past and Challenges for the Future 1 1,2 1,2 Manon Auffret • Sophie Drapier • Marc Ve´rin Published online: 15 March 2018 Ó The Author(s) 2018. This article is an open access publication Abstract Apomorphine is now recognized as the oldest antiparkinsonian drug on the market. Though still under- Key Points used, it is increasingly prescribed in Europe for patients with advanced Parkinson’s disease (PD) with motor fluc- Apomorphine has a long and tortuous path in the tuations. However, its history is far from being limited to therapeutic armamentarium, with numerous movement disorders. This paper traces the history of apo- indications in human and veterinary medicine. morphine, from its earliest empirical use, to its synthesis, The controversy that apomorphine aroused among pharmacological development, and numerous indications clinicians in the past (and in some ways, continues in human and veterinary medicine, in light of its most among neurologists) can be explained by the lack of recent uses and newest challenges. From shamanic rituals controlled studies and its affiliation to morphine. in ancient Egypt and Mesoamerica, to the treatment of There are three main indications for apomorphine: erectile dysfunction, from being discarded as a pharma- emetic, sedative, and antiparkinsonian. cological tool to becoming an essential antiparkinsonian drug, the path of apomorphine in the therapeutic arma- This old drug needs to be reconsidered by clinicians mentarium has been tortuous and punctuated by setbacks and will benefit from current galenic and technical and groundbreaking discoveries. -

Sider Its Chemical Aspects ; and (3) to Discuss Its Therapeutic Said to Have Already Been Arrived At
252 DR. SAINSBURY: CHEMICAL CONSTITUTION AND THERAPEUTIC ACTION. was instituted ; and it is to be particularly noted that of SummingS up the evidence, so far as it is possible to sum up the total 17 cases 13 occurred in the period ending 1876. oon a subject as to which so much is still to be learned, we In the various streets within a quarter-mile radius of the seems to reach the general conclusion that, as a result of the hospital the percentage of the population attacked in the simultaneouss action of causes favourable to the spread of ten,years 1871-80 ranged from 4 per cent. to 25 per cent., infection,ii the contagion of small-pox may sometimes be con- the average being 9 per cent.2 In the workhouse, on the veyedv atmospherically to a distance much greater than had other hand, only some 3 per cent. were attacked. The tbeen usually admitted-a distance measurable by quarters of difference is certainly considerable; but the fact that the miles.r In endeavouring to summarise the agencies which cases in the workhouse practically stopped after 1876, 1:have to do with this result it is necessary to bear in mind when revaccination became part of the administrative thatt other unknown agencies may also be involved, and that system, goes far to account for the low attack-rate calcu- sometimess the joint action of all the known agencies may not lated over the whole eleven years. Whether, in addition, bet necessary, special activity of some, perhaps, atoning for anything (is to be attributed to the age-distribution of relativer deficiency or absence, and vice versâ, of others the workhouse inmates or to previous small-pox or to Keeping1 this in view, the factors whose coincident operation the well - regulated conditions as to ventilation, clean- (can produce the result in question may be subdivided as liness, &c. -
Neotropical Primates 19(1), June 2012
Neotropical Primates A Journal of the Neotropical Section of the IUCN/SSC Primate Specialist Group Conservation International 2011 Crystal Drive, Suite 500, Arlington, VA 22202, USA ISSN 1413-4703 Abbreviation: Neotrop. Primates Editors Erwin Palacios, Conservación Internacional Colombia, Bogotá DC, Colombia Liliana Cortés Ortiz, Museum of Zoology, University of Michigan, Ann Arbor, MI, USA Júlio César Bicca-Marques, Pontifícia Universidade Católica do Rio Grande do Sul, Porto Alegre, Brasil Eckhard Heymann, Deutsches Primatenzentrum, Göttingen, Germany Jessica Lynch Alfaro, Institute for Society and Genetics, University of California-Los Angeles, Los Angeles, CA, USA Anita Stone, Museu Paraense Emílio Goeldi, Belém, Pará, Brazil News and Books Reviews Brenda Solórzano, Instituto de Neuroetología, Universidad Veracruzana, Xalapa, México Ernesto Rodríguez-Luna, Instituto de Neuroetología, Universidad Veracruzana, Xalapa, México Founding Editors Anthony B. Rylands, Conservation International, Arlington VA, USA Ernesto Rodríguez-Luna, Instituto de Neuroetología, Universidad Veracruzana, Xalapa, México Editorial Board Bruna Bezerra, University of Louisville, Louisville, KY, USA Hannah M. Buchanan-Smith, University of Stirling, Stirling, Scotland, UK Adelmar F. Coimbra-Filho, Academia Brasileira de Ciências, Rio de Janeiro, Brazil Carolyn M. Crockett, Regional Primate Research Center, University of Washington, Seattle, WA, USA Stephen F. Ferrari, Universidade Federal do Sergipe, Aracajú, Brazil Russell A. Mittermeier, Conservation International, Arlington, VA, USA Marta D. Mudry, Universidad de Buenos Aires, Argentina Anthony Rylands, Conservation International, Arlington, VA, USA Horácio Schneider, Universidade Federal do Pará, Campus Universitário de Bragança, Brazil Karen B. Strier, University of Wisconsin, Madison, WI, USA Maria Emília Yamamoto, Universidade Federal do Rio Grande do Norte, Natal, Brazil Primate Specialist Group Chairman, Russell A. Mittermeier Deputy Chair, Anthony B.