Protecting Mental Health in the Age of Anxiety: the Context of Valium's Development, Synthesis, and Discovery in the United States, to 1963 Catherine (Cai) E
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
ANNNNNNNNNNNNNNNNNNNN 100A 006 Left Eye Input Right Eye Input
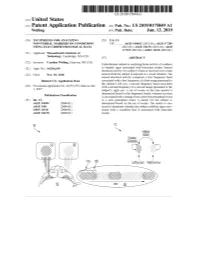
US 20190175049A1 ( 19) United States (12 ) Patent Application Publication (10 ) Pub. No. : US 2019 /0175049 A1 Welling ( 43 ) Pub . Date : Jun . 13 , 2019 ( 54 ) TECHNIQUES FOR ANALYZING (52 ) U . S . CI. NON -VERBAL MARKERS OF CONDITIONS CPC . .. A61B 5 /04842 (2013 . 01 ) ; A61B 5 / 7289 USING ELECTROPHYSIOLOGICAL DATA (2013 . 01) ; A61B 5 /0478 ( 2013 .01 ) ; A61B 5 /7225 ( 2013. 01 ) ; G06N 20 / 10 (2019 .01 ) (71 ) Applicant: Massachusetts Institute of Technology , Cambridge , MA (US ) ( 57 ) ABSTRACT (72 ) Inventor : Caroline Welling, Hanover, NH (US ) Embodiments related to analyzing brain activity of a subject to identify signs associated with binocular rivalry . Sensed ( 21 ) Appl. No. : 16 / 206, 639 electrical activity of a subject' s brain is received over a time period while the subject is exposed to a visual stimulus. The ( 22 ) Filed : Nov. 30 , 2018 sensed electrical activity comprises a first frequency band Related U . S . Application Data associated with a first frequency of a first image presented to the subject ' s left eye , a second frequency band associated (60 ) Provisional application No .62 / 593 , 535, filed on Dec . with a second frequency of a second image presented to the 1 , 2017 subject ' s right eye . A set of events in the time period is determined based on the frequency bands, wherein an event Publication Classification is associated with a change from a previous perceptual event (51 ) Int. Ci. to a new perceptual event. A metric for the subject is A61B 5 /0484 ( 2006 .01 ) determined based on the set of events . The metric is ana A61B 5 /00 ( 2006 .01 ) lyzed to determine whether the subject exhibits signs asso GO6N 20 / 10 (2006 .01 ) ciated with a condition that is associated with binocular A61B 5 /0478 ( 2006 .01 ) rivalry . -

Sulphonmethane, Sulphonal, Diethylsulpho
is a combination of amylene hydrate and chloral hydrate, superior to the corresponding compounds of other elements. while chloralose, a combination of chloral hydrate and glucose, Experience has shown that, in the main, these claims were un- partakes of the action of morphin and is rather expensive. founded, though many, even now, claim that strontium bro- Chloretone, a more recent product, is not entirely devoid of mid disturbs the stomach less than the corresponding sodium danger and is not always so certain in its action as chloral or potassium salt. Another claim that is frequently made by hydrate, while butyl chloral hydrate, or crotón chloral hydrate, manufacturers of nostrums, like "Peacock's Bromides," is that is one of the older compounds that has been found wanting and they use "chemically pure" salts. Exactly what is meant by is now little used. Of the official compounds of this group we this claim is difficult to say, but the Pharmacopeia gives us a have: number of readily applied tests by which the salts themselves Chloralamid and Paraldehyd. may be tested. The manufacturers of nostrums, on the other Chlobalformamidum.—TJ. S.—Chloralformamid. Chlorala- hand, not infrequently add the very substances that are consid- mid. This has practically the same action as therapeutic ered contaminations. doses of chloral hydrate, the latter being formed in the body by {To be continued.) decomposition of chloralformamid. Average dose: 1 gm. (15 grains). Paraldehtdum.—TJ. S.—Paraldehyd is slower in its action transparent liquid, slower in its action than chloral hydrate, but also safer. It has the disadvantage of a persistently dis- A NEW NEEDLE HOLDER. -

Upregulation of Peroxisome Proliferator-Activated Receptor-Α And
Upregulation of peroxisome proliferator-activated receptor-α and the lipid metabolism pathway promotes carcinogenesis of ampullary cancer Chih-Yang Wang, Ying-Jui Chao, Yi-Ling Chen, Tzu-Wen Wang, Nam Nhut Phan, Hui-Ping Hsu, Yan-Shen Shan, Ming-Derg Lai 1 Supplementary Table 1. Demographics and clinical outcomes of five patients with ampullary cancer Time of Tumor Time to Age Differentia survival/ Sex Staging size Morphology Recurrence recurrence Condition (years) tion expired (cm) (months) (months) T2N0, 51 F 211 Polypoid Unknown No -- Survived 193 stage Ib T2N0, 2.41.5 58 F Mixed Good Yes 14 Expired 17 stage Ib 0.6 T3N0, 4.53.5 68 M Polypoid Good No -- Survived 162 stage IIA 1.2 T3N0, 66 M 110.8 Ulcerative Good Yes 64 Expired 227 stage IIA T3N0, 60 M 21.81 Mixed Moderate Yes 5.6 Expired 16.7 stage IIA 2 Supplementary Table 2. Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of an ampullary cancer microarray using the Database for Annotation, Visualization and Integrated Discovery (DAVID). This table contains only pathways with p values that ranged 0.0001~0.05. KEGG Pathway p value Genes Pentose and 1.50E-04 UGT1A6, CRYL1, UGT1A8, AKR1B1, UGT2B11, UGT2A3, glucuronate UGT2B10, UGT2B7, XYLB interconversions Drug metabolism 1.63E-04 CYP3A4, XDH, UGT1A6, CYP3A5, CES2, CYP3A7, UGT1A8, NAT2, UGT2B11, DPYD, UGT2A3, UGT2B10, UGT2B7 Maturity-onset 2.43E-04 HNF1A, HNF4A, SLC2A2, PKLR, NEUROD1, HNF4G, diabetes of the PDX1, NR5A2, NKX2-2 young Starch and sucrose 6.03E-04 GBA3, UGT1A6, G6PC, UGT1A8, ENPP3, MGAM, SI, metabolism -

Determination of Barbiturates and 11-Nor-9-Carboxy-Δ9-THC in Urine
Determination of Barbiturates and 11-Nor-9-carboxy- 9-THC in Urine using Automated Disposable Pipette Extraction (DPX) and LC/MS/MS Fred D. Foster, Oscar G. Cabrices, John R. Stuff, Edward A. Pfannkoch GERSTEL, Inc., 701 Digital Dr. Suite J, Linthicum, MD 21090, USA William E. Brewer Department of Chemistry and Biochemistry, University of South Carolina, 631 Sumter St. Columbia, SC 29208, USA KEYWORDS DPX, LC/MS/MS, Sample Preparation, High Throughput Lab Automation ABSTRACT This work demonstrates the use of disposable pipette extraction (DPX) as a fast and automated sample preparation technique for the determination of barbiturates and 11-nor-9- carboxy- 9-THC (COOH-THC) in urine. Using a GERSTEL MultiPurpose Sampler (MPS) with DPX option coupled to an Agilent 6460 LC-MS/MS instrument, 8 barbiturates and COOH-THC were extracted and their concentrations determined. The resulting average cycle time of 7 min/ sample, including just-in-time sample preparation, enabled high throughput screening. Validation results show that the automated DPX-LC/ AppNote 1/2013 MS/MS screening method provides adequate sensitivity for all analytes and corresponding internal standards that were monitored. Lower limits of quantitation (LLOQ) were found to be 100 ng/mL for the barbiturates and 10 ng/mL for COOH-THC and % CVs were below 10 % in most cases. INTRODUCTION The continuously growing quantity of pain management sample extract for injection [1-2]. The extraction of the drugs used has increased the demand from toxicology Barbiturates and COOH-THC is based on the DPX-RP- laboratories for more reliable solutions to monitor S extraction method described in an earlier Application compliance in connection with substance abuse and/or Note detailing monitoring of 49 Pain Management diversion. -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -

Intravenous Anesthetics a Drug That Induces Reversible Anesthesia the State of Loss of Sensations, Or Awareness
DR.MED. ABDELKARIM ALOWEIDI AL-ABBADI ASSOCIATE PROF. FACULTY OF MEDICINE THE UNIVERSITY OF JORDAN Goals of General Anesthesia Hypnosis (unconsciousness) Amnesia Analgesia Immobility/decreased muscle tone (relaxation of skeletal muscle) Reduction of certain autonomic reflexes (gag reflex, tachycardia, vasoconstriction) Intravenous Anesthetics A drug that induces reversible anesthesia The state of loss of sensations, or awareness. Either stimulates an inhibitory neuron, or inhibits an excitatory neuron. Organs are divided according to blood perfusion: High- perfusion organs (vessel-rich); brain takes up disproportionately large amount of drug compared to less perfused areas (muscles, fat, and vessel-poor groups). After IV injection, vessel-rich group takes most of the available drug Drugs bound to plasma proteins are unavailable for uptake by an organ After highly perfused organs are saturated during initial distribution, the greater mass of the less perfused organs continue to take up drug from the bloodstream. As plasma concentration falls, some drug leaves the highly perfused organs to maintain equilibrium. This redistribution from the vessel-rich group is responsible for termination of effect of many anesthetic drugs. Compartment Model Inhibitory channels : GABA-A channels ( the main inhibitory receptor). Glycine channels. Excitatory channels : Neuronal nicotic. NMDA. Rapid onset (mainly unionized at physiological pH) High lipid solubility Rapid recovery, no accumulation during prolonged infusion Analgesic -

Benzodiazepine Zu Natur Und Kultur Einer Beliebten Substanzklasse
voll langweilig! Benzodiazepine zu Natur und Kultur einer beliebten Substanzklasse walter heuberger psgn klinik wil FOSUMOS Regionale Gesprächsgruppe St. Gallen März 2018 Inhalt Naturwissenschaft: Pharmakologie Wirkung/Indikationen/KI Benzodiazepinabhängigkeit Mehrfachabhängigkeit Benzodiazepinentzug Substitution Natur Geschichte der Benzodiazepine Was wesensgemäss von selbst da ist Leo Sternbach und der Zufall und sich selbst reproduziert. Kultur im 21. Jahrhundert Kultur Kultur und Benzodiazepine Alles, was der Mensch geschaffen hat, was also nicht naturgegeben ist. voll langweilig! Benzodiazepine FOSUMOS Regionale Gesprächsgruppe St. Gallen März 2018 Pharmakologie der Benzodiazepine voll langweilig! Benzodiazepine FOSUMOS Regionale Gesprächsgruppe St. Gallen März 2018 GABA (Gammaaminobuttersäure) • Wichtigster hemmender Neurotransmitter im Hirn O NH2 HO Relative Häufigkeit von Neuronen nach Neurotransmitter Neuroscience of Clinical Psychiatry Higgins 2007 • Die Aktivierung des GABAA Rezeptors bewirkt durch Chlorideinstrom in die Nervenzelle eine Hyperpolarisation der Zellmembran. • Die Nervenzelle wird so stabilisiert und reagiert weniger schnell. voll langweilig! Benzodiazepine FOSUMOS Regionale Gesprächsgruppe St. Gallen März 2018 Wirkort GABAA Rezeptor Aufbau Proteinkette gefaltet Untereiheit GABAA -Rezeptor GABAA Rezeptor Komplex elektronenmikroskopische Darstellung Nutt BJP 2001 179 Out In (a) (b) Cl – Figure 6.24 Orientation of the GABAA receptor in the membrane. voll langweilig! Benzodiazepine FOSUMOS Regionale Gesprächsgruppe -

International Classification of Diseases
INTERNATIONAL CLASSIFICATION OF DISEASES MANUAL OF THE INTERNATIONAL STATISTICAL CLASSIFICATION OF DISEASES, INJURIES, AND CAUSES OF DEATH Based on the Recommendations of the Eighth Revision Conference, 1965, and Adopted by the Nineteenth World Health Assembly Volume 2 ALPHABETICAL INDEX WORLD HEALTH ORGANIZATION GENEVA 1969 Volume 1 Introduction List of Three-digit Categories Tabular List of Inclusions and Four-digit Sub- categories Medical Certification and Rules for Classification Special Lists for Tabulation Definitions and Recommendations Regulations Volume 2 Alphabetical Index PRINTED IN ENGLAND CONTENTS Introduction Page General arrangement of the Index ....................................... VIII Main sections ............................................................... VIII Structure ..................................................................... IX Code numbzrs .............................................................. x Primary and secondary conditions. ................................... x Multiple diagnoses. ........................................................ XI Spelling....................................................................... XI Order of listing ............................................................. Conventions used in the Index ........................................... XII Parentheses. ................................................................. XII Cross-referexes ........................................................... XI1 Abbreviation NEC. ...................................................... -

Pharmaceutical Appendix to the Tariff Schedule 2
Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE Harmonized Tariff Schedule of the United States (2007) (Rev. 2) Annotated for Statistical Reporting Purposes PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 2 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. ABACAVIR 136470-78-5 ACIDUM LIDADRONICUM 63132-38-7 ABAFUNGIN 129639-79-8 ACIDUM SALCAPROZICUM 183990-46-7 ABAMECTIN 65195-55-3 ACIDUM SALCLOBUZICUM 387825-03-8 ABANOQUIL 90402-40-7 ACIFRAN 72420-38-3 ABAPERIDONUM 183849-43-6 ACIPIMOX 51037-30-0 ABARELIX 183552-38-7 ACITAZANOLAST 114607-46-4 ABATACEPTUM 332348-12-6 ACITEMATE 101197-99-3 ABCIXIMAB 143653-53-6 ACITRETIN 55079-83-9 ABECARNIL 111841-85-1 ACIVICIN 42228-92-2 ABETIMUSUM 167362-48-3 ACLANTATE 39633-62-0 ABIRATERONE 154229-19-3 ACLARUBICIN 57576-44-0 ABITESARTAN 137882-98-5 ACLATONIUM NAPADISILATE 55077-30-0 ABLUKAST 96566-25-5 ACODAZOLE 79152-85-5 ABRINEURINUM 178535-93-8 ACOLBIFENUM 182167-02-8 ABUNIDAZOLE 91017-58-2 ACONIAZIDE 13410-86-1 ACADESINE 2627-69-2 ACOTIAMIDUM 185106-16-5 ACAMPROSATE 77337-76-9 -
Benzodiazepines
Benzodiazepines CRIT program May 2010 Alex Walley, MD, MSc Primary Care Physician HIV Clinic, Boston Medical Center Medical Director, Opioid Treatment Program Boston Public Health Commission Medical Director, Overdose Prevention Pilot Program Massachusetts Department of Public Health CRIT 2010 Learning objectives At the end of this session, participants will be able to: 1. Understand why people use benzodiazepines 2. Know the characteristics of benzodiazepine intoxication and withdrawal syndromes 3. Understand the consequences of these drugs 4. Know the current options for treatment of benzodiazepine dependence CRIT 2010 Roadmap 1. Case and controversies 2. Epidemiology 3. Benzo effects 4. Treatment CRIT 2010 Case • 29 yo man presents for follow-up at methadone clinic after inpatient admission for femur fracture from falling onto subway track from platform. • Treated with clonazepam since age 16 for panic disorder. Takes 6mg in divided doses daily. Missed his afternoon dose day of the accident • Started using heroin at age 23. • On methadone maintenance for 1 year, doing well, about to get his first take home CRIT 2010 Controversies • Are benzodiazepines over-prescribed or under prescribed? • Are they safe in opioid dependent patients? • Why do people buy them off the street? • Why is it so hard to get chronic benzo users off of benzos? CRIT 2010 Why benzos? • Disabling anxiety, insomnia, nausea, seizure disorder • Chronically treated for whom discontinuation is feared • Boosting other sedating medications (opioids) • Euphoria seeking • Self-medication of opioid or alcohol withdrawal or cocaine toxicity CRIT 2010 Prescribers are ambivalent On the one hand On the other hand • Non-medical use of benzos • Rarely the drug of choice very common, esp. -

Drug and Medication Classification Schedule
KENTUCKY HORSE RACING COMMISSION UNIFORM DRUG, MEDICATION, AND SUBSTANCE CLASSIFICATION SCHEDULE KHRC 8-020-1 (11/2018) Class A drugs, medications, and substances are those (1) that have the highest potential to influence performance in the equine athlete, regardless of their approval by the United States Food and Drug Administration, or (2) that lack approval by the United States Food and Drug Administration but have pharmacologic effects similar to certain Class B drugs, medications, or substances that are approved by the United States Food and Drug Administration. Acecarbromal Bolasterone Cimaterol Divalproex Fluanisone Acetophenazine Boldione Citalopram Dixyrazine Fludiazepam Adinazolam Brimondine Cllibucaine Donepezil Flunitrazepam Alcuronium Bromazepam Clobazam Dopamine Fluopromazine Alfentanil Bromfenac Clocapramine Doxacurium Fluoresone Almotriptan Bromisovalum Clomethiazole Doxapram Fluoxetine Alphaprodine Bromocriptine Clomipramine Doxazosin Flupenthixol Alpidem Bromperidol Clonazepam Doxefazepam Flupirtine Alprazolam Brotizolam Clorazepate Doxepin Flurazepam Alprenolol Bufexamac Clormecaine Droperidol Fluspirilene Althesin Bupivacaine Clostebol Duloxetine Flutoprazepam Aminorex Buprenorphine Clothiapine Eletriptan Fluvoxamine Amisulpride Buspirone Clotiazepam Enalapril Formebolone Amitriptyline Bupropion Cloxazolam Enciprazine Fosinopril Amobarbital Butabartital Clozapine Endorphins Furzabol Amoxapine Butacaine Cobratoxin Enkephalins Galantamine Amperozide Butalbital Cocaine Ephedrine Gallamine Amphetamine Butanilicaine Codeine -

Leo Sternbach Mogens Schou Roland Kuhn
DURING THE PAST TWO MONTHS THREE MAJOR FIGURES IN THE HISTORY OF PSCHOPHARMACOLOGY PASSED AWAY: LEO STERNBACH MOGENS SCHOU ROLAND KUHN LEO STERNBACH The son of a Polish pharmacist Leo Sternbach was born in Abbazia, Croatia in 1907 He studied pharmacy and chemistry at Jegellonian University, in Cracow, Poland As a postdoctoral student he was involved in developing synthetic dyes and in the course of this process he synthesized several compounds known as HEPTOXDIAZINES, substances with a seven-membered ring After a short academic career at the Swiss Federal Institute of Technology in Zurich, he joined Hoffman-La-Roche in Europe After leaving Switzerland for the United States, he continued with Roche. He became Director of Medicinal Chemistry in the Chemical Research Department of Roche in Nutley, New Jersey LEO STERNBACH In the 1940s Sternbach thought that the HEPTOXDIAZINE structure might interact with CNS and stabilized one heptoxdiazine with methyl amine. He named the crystalline powder Ro 5-0690. Reprimanded for pursuing his own project on company time he was told to work on synthesizing potential antibiotics. In the mid-1950s Sternbach in view of the success of Miltown (meprobamate) as a tranquillizer was asked to study the drug and develop something “just different enough to get around the patent.” Reminded of his powder (Ro 5-0690) by a colleague who asked whether it should be thrown away, Sternbach decided to test Ro 5-0690 on mice. In behavioral pharmacological tests Ro 5-0690 was similar to Miltown and different from the barbiturates. Ro 5-0690, or chlordiazepoxide (methaminodiazepoxide) was given the brand name Librium.