201028 the Lymphatic System 2 – Structure and Function of The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Te2, Part Iii
TERMINOLOGIA EMBRYOLOGICA Second Edition International Embryological Terminology FIPAT The Federative International Programme for Anatomical Terminology A programme of the International Federation of Associations of Anatomists (IFAA) TE2, PART III Contents Caput V: Organogenesis Chapter 5: Organogenesis (continued) Systema respiratorium Respiratory system Systema urinarium Urinary system Systemata genitalia Genital systems Coeloma Coelom Glandulae endocrinae Endocrine glands Systema cardiovasculare Cardiovascular system Systema lymphoideum Lymphoid system Bibliographic Reference Citation: FIPAT. Terminologia Embryologica. 2nd ed. FIPAT.library.dal.ca. Federative International Programme for Anatomical Terminology, February 2017 Published pending approval by the General Assembly at the next Congress of IFAA (2019) Creative Commons License: The publication of Terminologia Embryologica is under a Creative Commons Attribution-NoDerivatives 4.0 International (CC BY-ND 4.0) license The individual terms in this terminology are within the public domain. Statements about terms being part of this international standard terminology should use the above bibliographic reference to cite this terminology. The unaltered PDF files of this terminology may be freely copied and distributed by users. IFAA member societies are authorized to publish translations of this terminology. Authors of other works that might be considered derivative should write to the Chair of FIPAT for permission to publish a derivative work. Caput V: ORGANOGENESIS Chapter 5: ORGANOGENESIS -

Health Tip: Swollen Lymph "Glands" - When Should You Be Concerned?
Printer Friendly Version Page 1 of 3 Health Tip: Swollen lymph "glands" - When should you be concerned? Lymph nodes, sometimes referred to as lymph "glands", are part of the body's lymphatic system. The lymphatic system consists of a system of conduits and organized collections of lymphoid tissue that include nodes, the tonsils, and the spleen. Coursing through these channels is liquid called lymph that eventually drains into the bloodstream near the heart, but along the way, it is "filtered" by the lymph nodes. Within these lymph nodes are high concentrations of disease fighting cells, particularly lymphocytes. While performing their intended function of fighting infection, lymph nodes typically become enlarged. In fact, infection is most common reason for lymph nodes enlargement. Lymph nodes are found throughout the body, but when enlarged, are usually noticed in characteristic locations, particularly the neck, groin and armpit regions. Lymph node enlargement can be localized to one group of lymph nodes or can be generalized (involving several sites of lymph nodes). For example, enlarged lymph nodes localized to the arm pit could occur as a result of a bacterial infection in a hand wound. Generalized lymph node swelling, on the other hand, could be seen in a systemic illness such as viral mononucleosis. In addition to viral and bacterial infections, other causes for enlarged lymph nodes include immune disorders (lupus, rheumatoid arthritis, etc.), cancers affecting the lymphatic system (leukemia, lymphoma, Hodgkin's disease), and cancers that have spread (metastasized) from some other part of the body to the lymphatic system. The discovery of enlarged lymph nodes often causes concern because many people are aware that lymph node enlargement can be an early sign of cancer. -

Regulate CD4 T Cell Responses Dependent Red Pulp Macrophages − CSF-1
CSF-1−Dependent Red Pulp Macrophages Regulate CD4 T Cell Responses Daisuke Kurotaki, Shigeyuki Kon, Kyeonghwa Bae, Koyu Ito, Yutaka Matsui, Yosuke Nakayama, Masashi Kanayama, This information is current as Chiemi Kimura, Yoshinori Narita, Takashi Nishimura, of September 29, 2021. Kazuya Iwabuchi, Matthias Mack, Nico van Rooijen, Shimon Sakaguchi, Toshimitsu Uede and Junko Morimoto J Immunol published online 14 January 2011 http://www.jimmunol.org/content/early/2011/01/14/jimmun Downloaded from ol.1001345 Supplementary http://www.jimmunol.org/content/suppl/2011/01/14/jimmunol.100134 Material 5.DC1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists by guest on September 29, 2021 • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2011 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Published January 14, 2011, doi:10.4049/jimmunol.1001345 The Journal of Immunology CSF-1–Dependent Red Pulp Macrophages Regulate CD4 T Cell Responses Daisuke Kurotaki,*,† Shigeyuki Kon,† Kyeonghwa Bae,† Koyu Ito,† Yutaka Matsui,* Yosuke Nakayama,† Masashi Kanayama,† Chiemi Kimura,† Yoshinori Narita,‡ Takashi Nishimura,‡ Kazuya Iwabuchi,x Matthias Mack,{ Nico van Rooijen,‖ Shimon Sakaguchi,# Toshimitsu Uede,*,† and Junko Morimoto† The balance between immune activation and suppression must be regulated to maintain immune homeostasis. -

Prolongevity Hormone FGF21 Protects Against Immune Senescence by Delaying Age-Related Thymic Involution
Prolongevity hormone FGF21 protects against immune senescence by delaying age-related thymic involution Yun-Hee Youma, Tamas L. Horvatha, David J. Mangelsdorfb,c, Steven A. Kliewerb,d, and Vishwa Deep Dixita,e,1 aSection of Comparative Medicine and Program on Integrative Cell Signaling and Neurobiology of Metabolism, Yale School of Medicine, New Haven, CT 06520; bDepartment of Pharmacology, University of Texas Southwestern Medical Center, Dallas, TX 75390; cHoward Hughes Medical Institute, University of Texas Southwestern Medical Center, Dallas, TX 75390; dDepartment of Molecular Biology, University of Texas Southwestern Medical Center, Dallas, TX 75390; and eDepartment of Immunobiology, Yale School of Medicine, New Haven, CT 06520 Edited by Ruslan Medzhitov, Yale School of Medicine, New Haven, CT, and approved December 16, 2015 (received for review July 22, 2015) Age-related thymic degeneration is associated with loss of naïve T showed that FGF7/keratinocyte growth factor (KGF) adminis- cells, restriction of peripheral T-cell diversity, and reduced health- tration in aged mice partially reversed thymic involution (17–19). span due to lower immune competence. The mechanistic basis of Notably, unlike most FGFs, FGF21 lacks affinity for heparan age-related thymic demise is unclear, but prior evidence suggests sulfate in the extracellular matrix and thus can be secreted to act that caloric restriction (CR) can slow thymic aging by maintaining in an endocrine fashion (20). FGF21 is predominantly secreted thymic epithelial cell integrity and reducing the generation of from liver but is also expressed in thymus (21). FGF21 is a pro- intrathymic lipid. Here we show that the prolongevity ketogenic longevity hormone that elicits it biological effects by binding to β hormone fibroblast growth factor 21 (FGF21), a member of the Klotho in complex with FGF receptor (FGFR) 1c, 2c, or 3c, but endocrine FGF subfamily, is expressed in thymic stromal cells along not FGFR4 (16, 22, 23). -
Central Immune Senescence, Reversal Potentials
31 Central Immune Senescence, Reversal Potentials Krisztian Kvell and Judit E. Pongracz Department of Medical Biotechnology, University of Pecs, Hungary 1. Introduction 1.1 Ageing in focus Ageing is a complex process that affects all living organisms. Senescence is not only conceivable in multicellular organisms, but also in unicellulars. Unlike certain diseases that have specific morbidity rates, ageing is a physiological process that affects all individuals that live long enough (unaffected by i.e. predation or famine) to experience senescence. A pioneer of ageing research, August Weismann has established two rather opposing concepts for aging and even today both gather numerous followers. One is the adaptive concept, according to which ageing has evolved to cleanse the population from old, non- reproductive consumers. The other, non-adaptive concept suggests that ageing is due to greater weight on early survival / reproduction rather than vigour at later ages. This latter has been reshaped by the theory of antagonistic pleiotropy (Ljubuncic et al. 2009). Due to advances in biomedical research and care, currently an average 55-aged person is expected to live up to 85 years of age at death on average in the Western societies. This number is expected to increase if biomedical research continues to develop at the current rate and by the year 2030 an average 55-aged person is expected to live up to 115 years of age at death (according to SENS plans) (de Grey 2007). If such forecasts prove to be true, it is of extraordinary significance and will likely trigger immense social and economical conflicts. 1.1.1 Ageing and society Ageing of the population is one of the most important challenges for the developed world to face over the next decades. -
Thymic Involution in Viable Motheaten (Me(V)) Mice Is Associated with a Loss of Intrathymic Precursor Activity
University of Massachusetts Medical School eScholarship@UMMS Open Access Articles Open Access Publications by UMMS Authors 1992-3 Thymic involution in viable motheaten (me(v)) mice is associated with a loss of intrathymic precursor activity Sandra M. Hayes University of Connecticut Health Center Et al. Let us know how access to this document benefits ou.y Follow this and additional works at: https://escholarship.umassmed.edu/oapubs Part of the Life Sciences Commons, and the Medicine and Health Sciences Commons Repository Citation Hayes SM, Shultz LD, Greiner DL. (1992). Thymic involution in viable motheaten (me(v)) mice is associated with a loss of intrathymic precursor activity. Open Access Articles. Retrieved from https://escholarship.umassmed.edu/oapubs/2309 This material is brought to you by eScholarship@UMMS. It has been accepted for inclusion in Open Access Articles by an authorized administrator of eScholarship@UMMS. For more information, please contact [email protected]. Developmental Immunology, 1992, Vol. 2, pp. 191-205 (C) 1992 Harwood Academic Publishers GmbH Reprints available directly from the publisher Printed in the United Kingdom Photocopying permitted by license only Thymic Involution in Viable Motheaten (mev) Mice is Associated with a Loss of Intrathymic Precursor Activity SANDRA M. HAYES,t LEONARD D. SHULTZ,* and DALE L. GREINERt "Department of Pathology, University of Connecticut Health Center, Farmington, Connecticut 06030 :The Jackson Laboratory, Bar Harbor, Maine 04609 Department of Medicine, University of Massachusetts, 55 Lake Avenue North, Worcester, Massachusetts 01655 Mice homozygous for the viable motheaten (mev) allele manifest abnormalities in thymocytopoiesis, are severely immunodeficient, and develop autoimmune disorders early in life. -

Thymic Involution Development in Two Different Models of Effects Of
Effects of Castration on Thymocyte Development in Two Different Models of Thymic Involution This information is current as Tracy S. P. Heng, Gabrielle L. Goldberg, Daniel H. D. Gray, of October 3, 2021. Jayne S. Sutherland, Ann P. Chidgey and Richard L. Boyd J Immunol 2005; 175:2982-2993; ; doi: 10.4049/jimmunol.175.5.2982 http://www.jimmunol.org/content/175/5/2982 Downloaded from References This article cites 64 articles, 27 of which you can access for free at: http://www.jimmunol.org/content/175/5/2982.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average by guest on October 3, 2021 Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2005 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology Effects of Castration on Thymocyte Development in Two Different Models of Thymic Involution1 Tracy S. P. Heng,2 Gabrielle L. Goldberg,2 Daniel H. D. Gray,2 Jayne S. -

Cells, Tissues and Organs of the Immune System
Immune Cells and Organs Bonnie Hylander, Ph.D. Aug 29, 2014 Dept of Immunology [email protected] Immune system Purpose/function? • First line of defense= epithelial integrity= skin, mucosal surfaces • Defense against pathogens – Inside cells= kill the infected cell (Viruses) – Systemic= kill- Bacteria, Fungi, Parasites • Two phases of response – Handle the acute infection, keep it from spreading – Prevent future infections We didn’t know…. • What triggers innate immunity- • What mediates communication between innate and adaptive immunity- Bruce A. Beutler Jules A. Hoffmann Ralph M. Steinman Jules A. Hoffmann Bruce A. Beutler Ralph M. Steinman 1996 (fruit flies) 1998 (mice) 1973 Discovered receptor proteins that can Discovered dendritic recognize bacteria and other microorganisms cells “the conductors of as they enter the body, and activate the first the immune system”. line of defense in the immune system, known DC’s activate T-cells as innate immunity. The Immune System “Although the lymphoid system consists of various separate tissues and organs, it functions as a single entity. This is mainly because its principal cellular constituents, lymphocytes, are intrinsically mobile and continuously recirculate in large number between the blood and the lymph by way of the secondary lymphoid tissues… where antigens and antigen-presenting cells are selectively localized.” -Masayuki, Nat Rev Immuno. May 2004 Not all who wander are lost….. Tolkien Lord of the Rings …..some are searching Overview of the Immune System Immune System • Cells – Innate response- several cell types – Adaptive (specific) response- lymphocytes • Organs – Primary where lymphocytes develop/mature – Secondary where mature lymphocytes and antigen presenting cells interact to initiate a specific immune response • Circulatory system- blood • Lymphatic system- lymph Cells= Leukocytes= white blood cells Plasma- with anticoagulant Granulocytes Serum- after coagulation 1. -

Pulp Border in L1-Deficient Mice Selective Malformation of the Splenic White
Selective Malformation of the Splenic White Pulp Border in L1-Deficient Mice Shih-Lien Wang, Michael Kutsche, Gino DiSciullo, Melitta Schachner and Steven A. Bogen This information is current as of September 27, 2021. J Immunol 2000; 165:2465-2473; ; doi: 10.4049/jimmunol.165.5.2465 http://www.jimmunol.org/content/165/5/2465 Downloaded from References This article cites 45 articles, 12 of which you can access for free at: http://www.jimmunol.org/content/165/5/2465.full#ref-list-1 Why The JI? Submit online. http://www.jimmunol.org/ • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average by guest on September 27, 2021 Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2000 by The American Association of Immunologists All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. Selective Malformation of the Splenic White Pulp Border in L1-Deficient Mice1 Shih-Lien Wang,* Michael Kutsche,† Gino DiSciullo,* Melitta Schachner,† and Steven A. Bogen2* Lymphocytes enter the splenic white pulp by crossing the poorly characterized boundary of the marginal sinus. In this study, we describe the importance of L1, an adhesion molecule of the Ig superfamily, for marginal sinus integrity. -

M. H. RATZLAFF: the Superficial Lymphatic System of the Cat 151
M. H. RATZLAFF: The Superficial Lymphatic System of the Cat 151 Summary Four examples of severe chylous lymph effusions into serous cavities are reported. In each case there was an associated lymphocytopenia. This resembled and confirmed the findings noted in experimental lymph drainage from cannulated thoracic ducts in which the subject invariably devdops lymphocytopenia as the lymph is permitted to drain. Each of these patients had com munications between the lymph structures and the serous cavities. In two instances actual leakage of the lymphography contrrult material was demonstrated. The performance of repeated thoracenteses and paracenteses in the presenc~ of communications between the lymph structures and serous cavities added to the effect of converting the. situation to one similar to thoracic duct drainage .The progressive immaturity of the lymphocytes which was noted in two patients lead to the problem of differentiating them from malignant cells. The explanation lay in the known progressive immaturity of lymphocytes which appear when lymph drainage persists. Thankful acknowledgement is made for permission to study patients from the services of Drs. H. J. Carroll, ]. Croco, and H. Sporn. The graphs were prepared in the Department of Medical Illustration and Photography, Dowristate Medical Center, Mr. Saturnino Viloapaz, illustrator. References I Beebe, D. S., C. A. Hubay, L. Persky: Thoracic duct 4 Iverson, ]. G.: Phytohemagglutinin rcspon•e of re urctcral shunt: A method for dccrcasingi circulating circulating and nonrecirculating rat lymphocytes. Exp. lymphocytes. Surg. Forum 18 (1967), 541-543 Cell Res. 56 (1969), 219-223 2 Gesner, B. M., J. L. Gowans: The output of lympho 5 Tilney, N. -
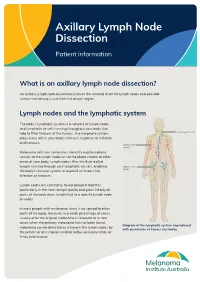
Axillary Lymph Node Dissection
Axillary Lymph Node Dissection Patient information What is an axillary lymph node dissection? An axillary lymph node dissection involves the removal of all the lymph nodes and possible tumour-containing tissue from the armpit region. Lymph nodes and the lymphatic system The body’s lymphatic system is a network of lymph nodes and lymphatic vessels running throughout your body that help to filter fluid out of the tissues. The lymphatic system plays a key role in your body’s immune response to infection and tumours. Melanoma cells can sometimes travel through lymphatic vessels to the lymph nodes or via the blood stream to other areas of your body. Lymph nodes filter the fluid (called lymph) running through your lymphatic vessels, enabling the body’s immune system to respond to threats like infection or tumours. Lymph nodes are commonly found grouped together, particularly in the neck, armpit (axilla) and groin. Nearly all parts of the body drain lymph fluid to a specific lymph node or nodes. In most people with melanoma, there is no spread to other parts of the body. However, in a small percentage of cases, usually after the original melanoma is removed or in rare cases when the primary melanoma has not been found, Diagram of the lymphatic system (reproduced melanoma can be detected as a lump in the lymph nodes by with permission of Cancer Australia). the patient or at a regular medical follow up examination or X-ray examination. In this situation, the standard treatment has been to remove all the lymph nodes in that area as often there is more than one lymph node involved. -

Extramedullary Hematopoiesis Generates Ly-6Chigh Monocytes That Infiltrate Atherosclerotic Lesions
Extramedullary Hematopoiesis Generates Ly-6Chigh Monocytes that Infiltrate Atherosclerotic Lesions The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Robbins, Clinton S., Aleksey Chudnovskiy, Philipp J. Rauch, Jose- Luiz Figueiredo, Yoshiko Iwamoto, Rostic Gorbatov, Martin Etzrodt, et al. 2012. “Extramedullary Hematopoiesis Generates Ly-6C High Monocytes That Infiltrate Atherosclerotic Lesions.” Circulation 125 (2): 364–74. https://doi.org/10.1161/circulationaha.111.061986. Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:41384259 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA NIH Public Access Author Manuscript Circulation. Author manuscript; available in PMC 2013 January 17. NIH-PA Author ManuscriptPublished NIH-PA Author Manuscript in final edited NIH-PA Author Manuscript form as: Circulation. 2012 January 17; 125(2): 364±374. doi:10.1161/CIRCULATIONAHA.111.061986. Extramedullary Hematopoiesis Generates Ly-6Chigh Monocytes that Infiltrate Atherosclerotic Lesions Clinton S. Robbins, PhD1,*, Aleksey Chudnovskiy, MS1,*, Philipp J. Rauch, BS1,*, Jose-Luiz Figueiredo, MD1, Yoshiko Iwamoto, BS1, Rostic Gorbatov, BS1, Martin Etzrodt, BS1, Georg F. Weber, MD1, Takuya Ueno, MD, PhD1, Nico van Rooijen, PhD2, Mary Jo Mulligan-Kehoe, PhD3, Peter