Radiographic, Fluoroscopic System UMDNS GMDN 16885 Radiographic/Fluoroscopic Systems, General- 37645 Stationary Basic Diagnostic X-Raysystem, Digital Purpose
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

RADIOGRAPHY to Prepare Individuals to Become Registered Radiologic Technologists
RADIOGRAPHY To prepare individuals to become Registered Radiologic Technologists. THE WORKFORCE CAPITAL This two-year, advanced medical program trains students in radiography. Radiography uses radiation to produce images of tissues, organs, bones and vessels of the body. The radiographer is an essential member of the health care team who works in a variety of settings. Responsibili- ties include accurately positioning the patient, producing quality diagnostic images, maintaining equipment and keeping computerized records. This certificate program of specialized training focuses on each of these responsibilities. Graduates are eligible to apply for the national credential examination to become a registered technologist in radiography, RT(R). Contact Student Services for current tuition rates and enrollment information. 580.242.2750 Mission, Goals, and Student Learning Outcomes Program Effectiveness Data Radiography Program Guidelines (Policies and Procedures) “The programs at Autry prepare you for the workforce with no extra training needed after graduation.” – Kenedy S. autrytech.edu ENDLESS POSSIBILITIES 1201 West Willow | Enid, Oklahoma, 73703 | 580.242.2750 | autrytech.edu COURSE LENGTH Twenty-four-month daytime program î August-July î Monday-Friday Academic hours: 8:15am-3:45pm Clinical hours: Eight-hour shifts between 7am-5pm with some ADMISSION PROCEDURES evening assignments required Applicants should contact Student Services at Autry Technology Center to request an information/application packet. Applicants who have a completed application on file and who have met entrance requirements will be considered for the program. Meeting ADULT IN-DISTRICT COSTS the requirements does not guarantee admission to the program. Qualified applicants will be contacted for an interview, and class Year One: $2732 (Additional cost of books and supplies approx: $1820) selection will be determined by the admissions committee. -

ACR–SPR-STR Practice Parameter for the Performance of Chest Radiography
The American College of Radiology, with more than 30,000 members, is the principal organization of radiologists, radiation oncologists, and clinical medical physicists in the United States. The College is a nonprofit professional society whose primary purposes are to advance the science of radiology, improve radiologic services to the patient, study the socioeconomic aspects of the practice of radiology, and encourage continuing education for radiologists, radiation oncologists, medical physicists, and persons practicing in allied professional fields. The American College of Radiology will periodically define new practice parameters and technical standards for radiologic practice to help advance the science of radiology and to improve the quality of service to patients throughout the United States. Existing practice parameters and technical standards will be reviewed for revision or renewal, as appropriate, on their fifth anniversary or sooner, if indicated. Each practice parameter and technical standard, representing a policy statement by the College, has undergone a thorough consensus process in which it has been subjected to extensive review and approval. The practice parameters and technical standards recognize that the safe and effective use of diagnostic and therapeutic radiology requires specific training, skills, and techniques, as described in each document. Reproduction or modification of the published practice parameter and technical standard by those entities not providing these services is not authorized. Revised 2017 (Resolution 2)* ACR–SPR–STR PRACTICE PARAMETER FOR THE PERFORMANCE OF CHEST RADIOGRAPHY PREAMBLE This document is an educational tool designed to assist practitioners in providing appropriate radiologic care for patients. Practice Parameters and Technical Standards are not inflexible rules or requirements of practice and are not intended, nor should they be used, to establish a legal standard of care1. -

Estimation of the Collective Effective Dose to the Population from Medical X-Ray Examinations in Finland
Estimation of the collective effective dose to the population from medical x-ray examinations in Finland Petra Tenkanen-Rautakoskia, Hannu Järvinena, Ritva Blya aRadiation and Nuclear Safety Authority (STUK), PL 14, 00880 Helsinki, Finland Abstract. The collective effective dose to the population from all x-ray examinations in Finland in 2005 was estimated. The numbers of x-ray examinations were collected by a questionnaire to the health care units (response rate 100 %). The effective doses in plain radiography were calculated using a Monte Carlo based program (PCXMC), as average values for selected health care units. For computed tomography (CT), weighted dose length product (DLPw) in a standard phantom was measured for routine CT protocols of four body regions, for 80 % of CT scanners including all types. The effective doses were calculated from DPLw values using published conversion factors. For contrast-enhanced radiology and interventional radiology, the effective dose was estimated mainly by using published DAP values and conversion factors for given body regions. About 733 examinations per 1000 inhabitants (excluding dental) were made in 2005, slightly less than in 2000. The proportions of plain radiography, computed tomography, contrast-enhanced radiography and interventional procedures were about 92, 7, 1 and 1 %, respectively. From 2000, the frequencies (number of examinations per 1000 inhabitants) of plain radiography and contrast-enhanced radiography have decreased about 8 and 33 %, respectively, while the frequencies of CT and interventional radiology have increased about 28 and 38 %, respectively. The population dose from all x-ray examinations is about 0,43 mSv per person (in 1997 0,5 mSv). -
Projectional Radiography Simulator: an Interactive Teaching Tool
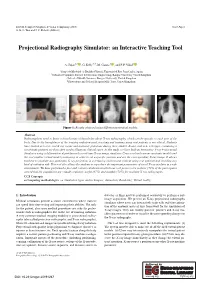
EG UK Computer Graphics & Visual Computing (2019) Short Paper G. K. L. Tam and J. C. Roberts (Editors) Projectional Radiography Simulator: an Interactive Teaching Tool A. Sujar1,2 , G. Kelly3,4, M. García1 , and F. P. Vidal2 1Grupo de Modelado y Realidad Virtual, Universidad Rey Juan Carlos, Spain 2School of Computer Science & Electronic Engineering, Bangor University United Kingdom 3School of Health Sciences, Bangor University, United Kingdom 4Shrewsbury and Telford Hospital NHS Trust, United Kingdom Figure 1: Results obtained using different anatomical models. Abstract Radiographers need to know a broad range of knowledge about X-ray radiography, which can be specific to each part of the body. Due to the harmfulness of the ionising radiation used, teaching and training using real patients is not ethical. Students have limited access to real X-ray rooms and anatomic phantoms during their studies. Books, and now web apps, containing a set of static pictures are then often used to illustrate clinical cases. In this study, we have built an Interactive X-ray Projectional Simulator using a deformation algorithm with a real-time X-ray image simulator. Users can load various anatomic models and the tool enables virtual model positioning in order to set a specific position and see the corresponding X-ray image. It allows teachers to simulate any particular X-ray projection in a lecturing environment without using real patients and avoiding any kind of radiation risk. This tool also allows the students to reproduce the important parameters of a real X-ray machine in a safe environment. We have performed a face and content validation in which our tool proves to be realistic (72% of the participants agreed that the simulations are visually realistic), useful (67%) and suitable (78%) for teaching X-ray radiography. -

ICD~10~PCS Complete Code Set Procedural Coding System Sample
ICD~10~PCS Complete Code Set Procedural Coding System Sample Table.of.Contents Preface....................................................................................00 Mouth and Throat ............................................................................. 00 Introducton...........................................................................00 Gastrointestinal System .................................................................. 00 Hepatobiliary System and Pancreas ........................................... 00 What is ICD-10-PCS? ........................................................................ 00 Endocrine System ............................................................................. 00 ICD-10-PCS Code Structure ........................................................... 00 Skin and Breast .................................................................................. 00 ICD-10-PCS Design ........................................................................... 00 Subcutaneous Tissue and Fascia ................................................. 00 ICD-10-PCS Additional Characteristics ...................................... 00 Muscles ................................................................................................. 00 ICD-10-PCS Applications ................................................................ 00 Tendons ................................................................................................ 00 Understandng.Root.Operatons..........................................00 -

Assessment of Bronchiectasis by Computed Tomography
Thorax: first published as 10.1136/thx.40.12.920 on 1 December 1985. Downloaded from Thorax 1985;40:920-924 Assessment of bronchiectasis by computed tomography IM MOOTOOSAMY, RH REZNEK, J OSMAN, RSO REES, MALCOLM GREEN From the Departments of Diagnostic Radiology and Chest Medicine, St Bartholomew's Hospital, London ABSTRACT Computed tomography and bronchography were used to assess the distribution of bronchiectasis in 15 lungs from eight patients with clinical features of the disease. Of the 36 lobes adequately displayed by bronchography, 22 were found to have bronchiectasis and 14 were found to be normal by both techniques. Cystic disease was readily identified by computed tomography but the cylindrical and varicose types of bronchiectasis could not be distinguished. Segmental local- isation was less accurate, with agreement between computed tomography and bronchography in 116 out of 130 segments. It is concluded that with a modern high resolution scanner computed tom- ography provides a useful method of assessing lobar distribution in bronchiectasis. The incidence of bronchiectasis in the United King- placing bronchography in a substantial number, dom has decreased since the advent ofantibiotic treat- Muller et al found correspondence in only about half ment and the decline in severe respiratory disease in the lungs studied. childhood. Nevertheless, it still occurs as the result of The purpose of this study is to assess the place of severe pulmonary infections and in association with modern high resolution computed tomography scan-copyright. immune deficiency, cystic fibrosis, and other condi- ners in the clinical management ofpatients with bron- tions. chiectasis and to investigate the accuracy with which The disease is defined as irreversible abnormal di- lobar and segmental disease and the type of disease latation of the bronchi and has been classified by present can be predicted. -

Download Article (PDF)
Current Directions in Biomedical Engineering 2015; 1:257–260 Thomas Homann*, Axel Boese, Sylvia Glaßer, Martin Skalej, and Oliver Beuing Intravascular optical coherence tomography (OCT) as an additional tool for the assessment of stent structures Abstract: Evaluation of the vascular stent position, shape cases an additional imaging of the implants by OCT would and correct expansion has a high relevance in therapy be benecial. In our study, we determined the ability of and diagnosis. Hence, the wall apposition in vessel areas OCT to image structural information of dierent vascular with diering diameters and the appearance of torsions or stents in a phantom study. structural defects of the implant body caused by catheter based device dropping are of special interest. Neurovascu- lar implants like braided ow diverter and laser cut stents 2 Materials and methods consist of metal struts and wires with diameters of about 40 µm. Depending on the implants material composition, A plastic model with bores of dierent diameters for the in- visibility is poor with conventional 2D X-ray uoroscopic take of 3 vascular implants was manufactured (see Figure and radiographic imaging. The metal structures of the im- 1). The model has a geometrical extend of 80 mm×50 mm× plants also lead to artifacts in 3D X-ray images and can 15 mm and a straight course of the bores. A translucent hamper the assessment of the device position. We inves- plastic material was selected for a low absorption of near tigated intravascular optical coherence tomography (OCT) infrared light generated by the OCT system. Objects of in- as a new imaging tool for the evaluation of the vascular vestigation were 3 vascular stents with dierent geometri- stent position, its shape and its correct expansion for 3 dif- cal and structural properties (see Table 1). -

X-Ray (Radiography) - Bone Bone X-Ray Uses a Very Small Dose of Ionizing Radiation to Produce Pictures of Any Bone in the Body
X-ray (Radiography) - Bone Bone x-ray uses a very small dose of ionizing radiation to produce pictures of any bone in the body. It is commonly used to diagnose fractured bones or joint dislocation. Bone x-rays are the fastest and easiest way for your doctor to view and assess bone fractures, injuries and joint abnormalities. This exam requires little to no special preparation. Tell your doctor and the technologist if there is any possibility you are pregnant. Leave jewelry at home and wear loose, comfortable clothing. You may be asked to wear a gown. What is Bone X-ray (Radiography)? An x-ray exam helps doctors diagnose and treat medical conditions. It exposes you to a small dose of ionizing radiation to produce pictures of the inside of the body. X-rays are the oldest and most often used form of medical imaging. A bone x-ray makes images of any bone in the body, including the hand, wrist, arm, elbow, shoulder, spine, pelvis, hip, thigh, knee, leg (shin), ankle or foot. What are some common uses of the procedure? A bone x-ray is used to: diagnose fractured bones or joint dislocation. demonstrate proper alignment and stabilization of bony fragments following treatment of a fracture. guide orthopedic surgery, such as spine repair/fusion, joint replacement and fracture reductions. look for injury, infection, arthritis, abnormal bone growths and bony changes seen in metabolic conditions. assist in the detection and diagnosis of bone cancer. locate foreign objects in soft tissues around or in bones. How should I prepare? Most bone x-rays require no special preparation. -

The ASRT Practice Standards for Medical Imaging and Radiation Therapy
The ASRT Practice Standards for Medical Imaging and Radiation Therapy Sonography ©2019 American Society of Radiologic Technologists. All rights reserved. Reprinting all or part of this document is prohibited without advance written permission of the ASRT. Send reprint requests to the ASRT Publications Department, 15000 Central Ave. SE, Albuquerque, NM 87123-3909. Effective June 23, 2019 Table of Contents Preface .......................................................................................................................................................... 1 Format ....................................................................................................................................................... 1 Introduction .................................................................................................................................................. 3 Definition .................................................................................................................................................. 3 Education and Certification ...................................................................................................................... 5 Medical Imaging and Radiation Therapy Scope of Practice .......................................................................... 6 Standards ...................................................................................................................................................... 8 Standard One – Assessment .................................................................................................................... -

Radiography Program
Radiography Program Program Description The Radiography (X-ray) Program at Tulsa Community College is designed to prepare students with the knowledge and skills to function as medical radiographers. The program is nationally accredited by the Joint Review Committee on Education in Radiologic Technology. Medical Radiographers/Radiologic Technologists are the medical personnel who perform diagnostic imaging examinations. Radiographers use x-rays to produce black and white images of anatomy. These images are captured on film, computer or videotape. Radiographers are educated in anatomy, patient positioning, examination techniques, equipment protocols, radiation safety, radiation protection and basic patient care. Radiographers often specialize in areas of CT, MRI, Mammography, Cardiovascular Technology, Quality Control, Management and Education. Radiographers work closely with radiologists, physicians who interpret medical images to either diagnose or rule out disease or injury. Program Information Degree Awarded: Associate Degree in Applied Science The Radiography (X-ray) Program admits a new class each year beginning in June (summer term). The number of students admitted to the class is determined by the number of clinical training sites available to place students, which is usually between 30-35 students. Radiography is a two-year (six-semester) program consisting of 48 credit hours of Radiography courses (didactic and clinical) and 22 hours of related general education courses. Lecture and clinical courses run concurrently throughout the two years. Upon completion of the program, graduates receive an Associate in Applied Science (AAS) degree, and are eligible to apply for examination by the American Registry of Radiologic Technologists (ARRT) in Radiography (R). Clinical education classes consist of eight-hour shifts for two to three days per week in the assigned clinical education center. -

Role of High-Resolution CT in Diagnosis, Regional Distribution and Characterize Bronchiectasis Morphologically
International Journal of Radiology and Diagnostic Imaging 2021; 4(1): 166-170 E-ISSN: 2664-4444 P-ISSN: 2664-4436 www.radiologypaper.com Role of high-resolution CT in diagnosis, regional IJRDI 2021; 4(1): 166-170 Received: 30-11-2020 distribution and characterize bronchiectasis Accepted: 05-01-2021 morphologically Priyanka Patil Specialist Radiologist, Department of Radiology, Priyanka Patil, Gururaj Bangari, Veeresh Hanchinal and Rahul Shirol Gadag Institute of Medical Sciences, Malasamudra, Karnataka, India DOI: http://dx.doi.org/10.33545/26644436.2021.v4.i1c.180 Gururaj Bangari Abstract Assistant Professor, Background: Bronchiectasis causes physical, social, and financial strain on affected patients and Department of Radiology, results in a significant negative effect on the quality of life of the patient. SDM College of Medical Objectives: This study was undertaken to find the role of HRCT in diagnosis, regional distribution and Sciences and Hospital, characterize bronchiectasis morphologically. Dharwad, Karnataka, India Method: A prospective study of sixty patients was done in whom clinically bronchiectasis was Veeresh Hanchinal suspected and were subjected to HRCT examination. Bronchiectasis was assessed in terms of Associate Professor, localization, regional distribution and morphological forms. Department of Radiology, Results: The mean age for all patients included in the study was 50.7 ± 12.09. The mean age of the Gadag Institute of Medical male patients was 51.56 ± 12.09 and the mean age of the female patients was 50.16 ± 12.23Out of a Sciences, Malasamudra, total of 60 patients there were 23 (38%) males and 37 (62%) females. 18 patients (30%) had unilateral Karnataka, India disease & 42 (70%) had disease in both lungs. -

CT Versus Bronchography in the Diagnosis and Management of Tracheobronchomalacia in Ventilator Dependent Infants
ADC-FNN Online First, published on April 27, 2005 as 10.1136/adc.2004.062604 Arch Dis Child Fetal Neonatal Ed: first published as 10.1136/adc.2004.062604 on 27 April 2005. Downloaded from CT versus bronchography in the diagnosis and management of tracheobronchomalacia in ventilator dependent infants + Mok Q#, Negus S*, McLaren CA*, Rajka T#, Elliott MJ , Roebuck DJ* & McHugh K* + #Paediatric Intensive Care Unit, Cardiothoracic Unit and *Department of Radiology Great Ormond Street Hospital for Children, London, United Kingdom. Address for correspondence: Quen Mok, Pediatric Intensive Care Unit, Great Ormond Street Hospital for Children, London WCIN 3JH copyright. United Kingdom Tel: +44 20 7813 8213 Fax: +44 20 7813 8206 Email: [email protected] http://fn.bmj.com/ on September 28, 2021 by guest. Protected 1 Copyright Article author (or their employer) 2005. Produced by BMJ Publishing Group Ltd (& RCPCH) under licence. Arch Dis Child Fetal Neonatal Ed: first published as 10.1136/adc.2004.062604 on 27 April 2005. Downloaded from Abstract Aim: To assess the relative accuracy of dynamic spiral computed tomography (CT) compared to tracheobronchography, in a population of ventilator dependent infants with suspected tracheobronchomalacia (TBM). Setting: Pediatric intensive care unit in a tertiary teaching hospital Patients and methods: Infants referred for investigation and management of ventilator dependence and suspected to have TBM were recruited into the study. Tracheobronchography and CT were performed during the same admission by different investigators who were blinded to the results of the other investigation. The study was approved by the hospital research ethics committee and signed parental consent was obtained.