Iraq Watching Briefs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Country of Origin Information Iraq
COUNTRY OF ORIGIN INFORMATION IRAQ United Nations High Commissioner for Refugees (UNHCR) October 2005 This report has been produced by UNHCR on the basis of information obtained from a variety of publicly available sources, analyses and comments. The purpose of the report is to serve as a reference for a breadth of country of origin information and thereby assists, inter alia, in the asylum determination process and when assessing the feasibility of returns to Iraq in safety and dignity. The information contained does not purport to be exhaustive with regard to conditions in the country surveyed, and incomplete, inaccurate or incorrect information cannot be ruled out. The inclusion of information in this report does not constitute an endorsement of the information or views of third parties. Neither does such information necessarily represent statements of policy or views of UNHCR or the United Nations. In particular the use of ethnic-sectarian terms such as ‘Shiite’, ‘Sunni’ or ‘Kurd’ does not constitute an endorsement of sectarianism but merely reflects the current realities on the ground (i.e. these groups should not be considered homogenous entities). ii Table of contents TABLE OF CONTENTS ................................................................................................ III LIST OF ACRONYMS ..................................................................................................VII EXECUTIVE SUMMARY ................................................................................................ 1 A. INTRODUCTION -
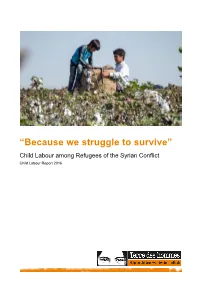
'Because We Struggle to Survive'
“Because we struggle to survive” Child Labour among Refugees of the Syrian Conflict Child Labour Report 2016 Disclaimer terre des hommes Siège | Hauptsitz | Sede | Headquarters Avenue de Montchoisi 15, CH-1006 Lausanne T +41 58 611 06 66, F +41 58 611 06 77 E-mail : [email protected], CCP : 10-11504-8 Research support: Ornella Barros, Dr. Beate Scherrer, Angela Großmann Authors: Barbara Küppers, Antje Ruhmann Photos : Front cover, S. 13, 37: Servet Dilber S. 3, 8, 12, 21, 22, 24, 27, 47: Ollivier Girard S. 3: Terre des Hommes International Federation S. 3: Christel Kovermann S. 5, 15: Terre des Hommes Netherlands S. 7: Helmut Steinkeller S. 10, 30, 38, 40: Kerem Yucel S. 33: Terre des hommes Italy The study at hand is part of a series published by terre des hommes Germany annually on 12 June, the World Day against Child Labour. We would like to thank terre des hommes Germany for their excellent work, as well as Terre des hommes Italy and Terre des Hommes Netherlands for their contributions to the study. We would also like to thank our employees, especially in the Middle East and in Europe for their contributions to the study itself, as well as to the work of editing and translating it. Terre des hommes (Lausanne) is a member of the Terre des Hommes International Federation (TDHIF) that brings together partner organisations in Switzerland and in other countries. TDHIF repesents its members at an international and European level. First published by terre des hommes Germany in English and German, June 2016. -

The Case of the Iraqi Disputed Territories Declaration Submitted By
Title: Education as an Ethnic Defence Strategy: The Case of the Iraqi Disputed Territories Declaration Submitted by Kelsey Jayne Shanks to the University of Exeter as a thesis for the degree of Doctor of Philosophy in Politics, October 2013. This thesis is available for Library use on the understanding that it is copyright material and that no quotation from the thesis may be published without proper acknowledgement. I certify that all material in this thesis which is not my own work has been identified and that no material has previously been submitted and approved for the award of a degree by this or any other University. Kelsey Shanks ................................................................................. 1 Abstract The oil-rich northern districts of Iraq were long considered a reflection of the country with a diversity of ethnic and religious groups; Arabs, Turkmen, Kurds, Assyrians, and Yezidi, living together and portraying Iraq’s demographic makeup. However, the Ba’ath party’s brutal policy of Arabisation in the twentieth century created a false demographic and instigated the escalation of identity politics. Consequently, the region is currently highly contested with the disputed territories consisting of 15 districts stretching across four northern governorates and curving from the Syrian to Iranian borders. The official contest over the regions administration has resulted in a tug-of-war between Baghdad and Erbil that has frequently stalled the Iraqi political system. Subsequently, across the region, minority groups have been pulled into a clash over demographic composition as each disputed districts faces ethnically defined claims. The ethnic basis to territorial claims has amplified the discourse over linguistic presence, cultural representation and minority rights; and the insecure environment, in which sectarian based attacks are frequent, has elevated debates over territorial representation to the height of ethnic survival issues. -

The Civilian Youth and Time of Crisis a Field Research in the Sociology of Living in a Various Civilian/Local Society(Mosul City As a Field Study)
JOURNAL OF CRITICAL REVIEWS ISSN- 2394-5125 VOL 7, ISSUE 09, 2020 THE CIVILIAN YOUTH AND TIME OF CRISIS A FIELD RESEARCH IN THE SOCIOLOGY OF LIVING IN A VARIOUS CIVILIAN/LOCAL SOCIETY(MOSUL CITY AS A FIELD STUDY) Asst.Prof. Dr. HasanJassim Rashid University of Mosul,College of Arts,Department of Sociology,Mosul, Iraq E-mail:[email protected] Civil Youth and Time of Crisis: Participatory Research With A Group of Students from the Department of Sociology to Know the Sociology of Living in a Diverse Community/Iraqi City of Mosul as Field of the Study. Received: 08.03.2020 Revised: 25.04.2020 Accepted: 14.05.2020 Abstract Young people are the mainstay of society, not only in terms of continuity in human existence, but also as a continuation of social thought, so they must be involved in finding solutions to those problems that affect their communities, such as Isis's control of Nineveh province and its center "the city of Mosul", which is socially and culturally heterogeneous. Therefore, these young people are the means and the goal in their view of this conflict and how to contribute to the mitigation of its results. The young people here are participants and through the experimental participation of questions and the distribution of those questions and answering them we can know their point of view about ISIS's control over their regions and the disadvantages of that control in what concerns civil liberties and its behaviors and the prevention of communication and interaction with others who belong to different cultural identity to create national distinction in difficult circumstances that their society passed through in ascending stages started from an epicenter of political crisis and then there were some automatic factors that helped to aggravate the situation with a favorable conditions till the crisis reached a stage of tension and anxiety then came the calm that precedes the storm. -

Iraq ELITES Rapid Labor Market Assessment (RLMA) Report
Iraq ELITES Rapid Labor Market Assessment (RLMA) Report English Language Investment & Training for Economic Success (ELITES) World Learning A project funded by the U.S. Embassy in Baghdad, designed and implemented by World Learning Inc. Iraq ELITES Rapid Labor Market Assessment (RLMA) Report Catherine Honeyman and Hannah Zuzek December 14, 2020 Table of Contents Acknowledgments ......................................................................................................................................... 2 Executive Summary ....................................................................................................................................... 3 I. Introduction and Methodology .................................................................................................................. 6 Phase 1: Desk research to identify growing areas of employment .......................................................... 6 Phase 2: Stakeholder Surveys ................................................................................................................... 8 Final Sample .............................................................................................................................................. 8 II. Employment Opportunities .................................................................................................................... 10 III. Skill Requirements and Skill Gaps .......................................................................................................... 15 English -
Interreligious Dialogue Mapping of the Middle East
PANTONE 2292 C PANTONE 416 C or similar or similar RGB 147 201 14 RGB 126 127 116 HEX 93C90E HEX 7E7F74 CMYK 48 0 92 0 CMYK 28 18 29 51 PANTONE P 104-16 U PANTONE P 179-14 U Interreligious Dialogue Mapping of the Middle East Lebanon, Jordan, Turkey and Iraq 2020 Interreligious Dialogue Mapping of the Middle East: Lebanon, Jordan, Turkey and Iraq Published by: Adyan Foundation Institute of Citizenship and Diversity Management and Rashad Center for Cultural Governance Lead Researcher: Michael Daniel Driessen, PhD Local Researchers: Anna Maria Daou (Lebanon) Dima Karadsheh (Jordan) Neira Omerovic (Turkey) Faris Ilyas Keti (Iraq) Under the direction of: Nayla Tabbara, PhD Director of the Institute of Citizenship and Diversity Management at the Adyan Foundation Ahmed Nagi Research Manager at the Institute of Citizenship and Diversity Management, Adyan Foundation © All Rights Reserved for Adyan Foundation Beirut, 2020 Table of Contents Executive Summary ........................................................................................ 1 Introduction .................................................................................................... 3 1. Theoretical Framework for Evaluating Interreligious Dialogue ........... 6 Preliminary Considerations: Defining and Naming Interreligious Dialogue ........................................ 6 Typologies of Interreligious Dialogue....................................................... 6 I. Type of Organization ................................................................................. -

Millennial Generation in Post-Intervention Iraq – What Alternatives for Destitute Youth in Ill-Functionning State? " by Nils BARTOLOMEO
"The Millennial Generation in Post-Intervention Iraq – What alternatives for destitute youth in ill-functionning state? " By Nils BARTOLOMEO Course “Sociologie des relations internationales dans le monde” Taught by Laurent Bonnefoy at Sciences Po Fall 2016 This paper has received the KSP Student Paper Award of the Kuwait Program at Sciences Po © The copyright of this paper remains the property of its author. No part of the content may be reproduced, published, distributed, copied or stored for public or private use without written permission of the author. All authorisation requests should be sent to [email protected] SCIENCES PO NILS BARTOLOMÉO THE MILLENNIAL GENERATION IN POST-INTERVENTION IRAQ — What alternatives for a destitute youth in an ill-functioning state ? — « If you catch the youth, you catch the future1 . » Saddam Hussein Introduction. In the context of the « war on terror », the U.S. intervention in Iraq sought to deeply transform the country, and with it the region, by inoculating democratic liberal values. The tacit objective of this « radical interventionism2 » was to turn Iraq into the glowing showcase of Western liberal values within the Arab world. The intervention turned out to be a fiasco and many since then consider Iraq as a « failed state3 ». However, although the U.S. intervention undoubtedly worsened Iraq’s domestic situation, one must bear in mind that Iraq’s predicament is actually the result of a long-term process. Today’s situation leaves us with a lingering sense of deja-vu. Since the Iran-Iraq war in the 1980s, the « sanctions decade4 » that followed the 1991 Gulf War, coupled with a large financial debt resulting from the war and the repression conducted by Saddam Hussein, strongly damaged the material, institutional and psychological foundations© of the Iraqi society. -

Iraq As a Failed State
Iraq as a Failed State Anthony H. Cordesman With the assistance of Max Molot Working Paper: November 18, 2019 Please provide comments to [email protected] Photo: HUSSEIN FALEH/AFP/Getty Images Cordesman: Iraq as a Failed State 11/18/19 1 Iraq as a Failed State Anthony H. Cordesman with the assistance of Max Molot The last few weeks have shown that Iraqis have effectively run out of patience with what has become yet another failed, corrupt government. Part of this is sheer frustration with the government’s incompetence and corruption – coupled with its failure to develop an effective recovery effort in the large Sunni areas in the West affected by the fight against ISIS, and its chronic failures to meet the needs and expectations of the rest of its population. What is less apparent, however, is just how bad things in Iraq really are. Its problems are not short- term political issues that can be solved by reforming its government and cutting corruption. They are products of deep sectarian and ethnic tensions and almost continuous war or crisis from the beginning of the Iran-Iraq War in 1980 to the present – a period of some 40 years. Today’s upheavals are not the result of some sudden form of local “populism.” There has never been a modern government in Iraq that pursued effective efforts at economic development and meeting the broader needs of its people. In some cases, like its agricultural development, and creation of some of the most expensive and unproductive state-owned enterprises (SOEs) in the world, they trace back to at least the fall of the monarchy in July 1958. -

Co-Operation Between the EU and Iraq
COOPERATION BETWEEN THE EUROPEAN UNION AND IRAQ Joint Strategy Paper 2011 – 2013 Table of Contents List of Acronyms 4 Executive Summary 5 Introduction – From Reconstruction to Development 6 Chapter 1: Framework for relations between the EU and Iraq 7 1.1. General objectives for cooperation with Iraq 7 1.2. Strategic objectives for cooperation with Iraq 7 1.3. Main bilateral agreements 8 Chapter 2: Joint Country Diagnosis 8 2.1. Analysis of the political, economic, social and environmental situation in Iraq 8 2.1.1. Political and security situation 8 2.1.2. Economic and social situation 10 2.1.3. Social situation, including decent work and unemployment 11 2.1.4. Iraq in the international context 12 2.1.5. Environmental situation 14 2.2. Development strategy of Iraq 14 2.3. Analysis of the viability of current policies and the medium term challenges 15 Chapter 3: Joint Overview of Cooperation and Political Dialogue Complementarity and consistency 16 3.1. European Commission 16 3.1.1. Overview of the European Commission’s past and present cooperation (lessons learned) 16 3.1.2. Information on the programmes of other donors (complementarity) 21 3.1.3. Description of the political dialogue between the EU and Iraq 23 3.1.4. Description of the state of development cooperation with Iraq and progress towards harmonisation 24 3.1.5. Analysis of consistency with EU policies (policy coherence) 25 3.2. Italy 26 3.2.1. Italy’s overview – past and present cooperation with Iraq 26 3.2.2. Information on the Italian bilateral programmes 27 3.2.3. -

Iraq Country Plan of Implementation Orange Knowledge Programme
Iraq Country Plan of Implementation Orange Knowledge Programme I. Introduction II. Brief presentation of the OKP programme III. Current state of affairs IV. Identification of the needs (priority theme and education gap) • The selected priority theme • Analysis of the priority theme The embassy’s objectives in the field of post-secondary education, relevant to the priority theme • The education and training gap in the priority theme Structure and current status of the provision of post-secondary education for the priority theme Analysis of the education and training gap for the priority theme V. Envisaged Theory of Change and outcomes VI. Articulation and calls VII. Indicative budget for the programme VIII. Coordination with other programmes IX. Monitoring programme progress Iraq - Country Plan of Implementation – Orange Knowledge Programme 1 / 28 List of abbreviations b2b business to business CPI Country Plan of Implementation CSA Climate Smart Agriculture EKN Embassy of the Kingdom of the Netherlands FNS Food and Nutrition Security g2g Government to government GoI Government of Iraq HE Higher Education IDP Internally Displaced People k2k knowledge institution to knowledge institution KRG Kurdistan Regional Government KRI Kurdistan Region of Iraq MA Ministry of Agriculture MASP Multi Annual Country Strategy MENA Middle East and North Africa MOE Ministry of Education MOFA Ministry of Foreign Affairs MOHESR Ministry of Higher Education and Scientific Research MOWR Ministry of Water Resources MSP MENA Scholarship Programme NFP Netherlands Fellowship Programmes NGO Non-Governmental Organisation NICHE Netherlands Initiative for Capacity development in Higher Education OKP Orange Knowledge Programme RRP Recovery and Resilience Programme ToC Theory of Change TVET Technical and Vocational Education and Training Iraq - Country Plan of Implementation – Orange Knowledge Programme 2 / 28 I. -
Uncertain Futures
UNCERTAIN FUTURES The impact of displacement on Syrian refugee and Iraqi internally displaced youth in Iraq Save the Children – Uncertain Futures LIST OF CONTENTS 1. Executive Summary 1 2. Introduction 5 3. Methodology 6 4. Findings 9 5. Conclusions 31 Endnotes 32 Author: Sarah Ireland, Humanitarian Advocacy and Policy Adviser, Save the Children Australia Front cover photo: Mohammed, 12 years old, is displaced in an urban community in Kirkuk. Photo: Ali Arkady/Save the Children. Save the Children in Iraq Save the Children has been working in Iraq since 1991, with a brief interruption from 2007 to 2008. Save the Children has been providing emergency response to Syrian refugees since 2012 and Iraqi internally displaced persons from the latest displacement crisis since 2014. Save the Children works with vulnerable groups in the community, focusing on areas least served by other agencies, and those with the greatest need. Save the Children in Iraq promotes and protects children’s rights with programs in child protection, health, education, livelihoods, child rights governance, shelter, and water, sanitation and hygiene. B 1. EXECUTIVE SUMMARY As the conflict in Syria edges towards its sixth year and world leaders grapple with its catastrophic human consequences, much attention has focussed on the conflict itself as the driver of mass migration to Europe. In this report, we seek to highlight a related but distinct set of drivers for a particular group of young, displaced people living in Iraq, and consider the terrible personal impact that displacement has had on their lives. The Iraqi ‘youth bulge’ and its repercussions Iraq has one of the highest youth populations in the world. -

The State of Disaster Risk Reduction in Iraq
THE STATE OF DISASTER RISK REDUCTION IN IRAQ EARL JAMES GOODYEAR, PH.D. DISASTER RISK MANAGEMENT CONSULTANT August 5, 2009 “While we cannot prevent natural phenomena such as earthquakes and cyclones, we can limit their impacts. The scale of any disaster is linked closely to past decisions taken by citizens and governments – or the absence of such decisions. Pre‐emptive risk reduction is the key. Sound response mechanisms after the event, however effective, are never enough.” BAN KI‐MOON SECRETARY‐GENERAL OF THE UNITED NATIONS Table of Contents List of Abbreviations and Acronyms Executive Summary …………………………………………………………………………………………………………………………………1 Section I: Situation Analysis ……………..……………………………………………………………………………………………………………………...6 Introduction.…........................................................................................................................................................6 Disaster Management in Iraq...............................................................................................................................12 Hazards, Vulnerabilities and Capacities…............................................................................................................13 Disaster Preparedness, Response and Recovery................................................................................................33 Section II: Accomplishments and Challenges ...........................................................................................................................................................................37