Edition 2 Trauma Basics
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Guidelines for Field Triage of Injured Patients (Regional Modifications Are Permissible)
Arizona Guidelines for Field Triage of Injured Patients (Regional modifications are permissible) FIELD TRIAGE DECISION SCHEME Measure vital signs and level of consciousness Glasgow Coma Scale ≤13 Systolic blood pressure (mmHg) <90 mmHg Step One Respiratory rate <10 or >29 breaths per minute (<20 in infant aged < 1 year1), or need for ventilator support YES NO Transport to a Trauma Center2. Steps 1 and 2 attempt to identify the most seriously injured Assess anatomy of injury. patients. These patients should be transported preferentially to the highest level of care within the trauma system. • All penetrating injuries to head, neck, torso, and extremities proximal to elbow or knee • Chest wall instability or deformity (e.g., flail chest) • Two or more proximal long-bone fractures • Crushed, de-gloved, mangled, or pulseless extremity Step Two3 • Amputation proximal to wrist or ankle • Pelvic fractures • Open or depressed skull fracture • Paralysis YES NO Transport to a Trauma Center2. Steps 1 and 2 attempt to identify the most seriously injured Assess mechanism of injury patients. These patients should be transported preferentially to the highest level of care within the and evidence of high-energy trauma system. impact. • Falls o Adults: >20 feet (one story is equal to 10 feet) 4 o Children : >10 feet or two or three times the height of the child • High-risk auto crash 5 Intrusion , including roof: >12 inches occupant site; >18 inches any site Step Three3 o o Ejection (partial or complete) from automobile o Death in same passenger compartment o Vehicle telemetry data consistent with high risk of injury 6 • Auto vs. -

Boerhaave's Syndrome – Tension Hydropneumothorax and Rapidly
Boerhaave’s syndrome – tension hydropneumothorax and rapidly developing hydropneumothorax: two radiographic clues in one case Lam Nguyen Ho, Ngoc Tran Van & Thuong Vu Le Department of Internal Medicine, Faculty of Medicine, University of Medicine and Pharmacy, Ho Chi Minh City, Vietnam. Keywords Abstract Boerhaave’s syndrome, hydropneumothorax, methylene blue, pleural effusion, tension Boerhaave’s syndrome is a rare and severe condition with high mortality partly pneumothorax. because of its atypical presentation resulting in delayed diagnosis and management. Diagnostic clues play an important role in the approach to this syndrome. Here, we Correspondence report a 48 year-old male patient hospitalized with fever and left chest pain radiating Nguyen Ho Lam, Department of Internal into the interscapular area. Two chest radiographs undertaken 22 h apart showed a Medicine, Faculty of Medicine, University of rapidly developing tension hydropneumothorax. The amylase level in the pleural Medicine and Pharmacy, 217 Hong Bang fl fl Street, Ward 11, District 5, Ho Chi Minh City, uid was high. The uid in the chest tube turned bluish after the patient drank Vietnam. E-mail: [email protected] methylene blue. The diagnosis of Boerhaave’s syndrome was suspected based on the aforementioned clinical clues and confirmed at the operation. The patient Received: 17 January 2016; Revised: recovered completely with the use of antibiotics and surgical treatment. In this case, 25 February 2016; Accepted: 10 March 2016 we describe key findings on chest radiographs that are useful in diagnosing Boerhaave’s syndrome. Respirology Case Reports, 4(4),2016,e00160 doi: 10.1002/rcr2.160 Introduction severe left chest pain radiating into the interscapular area. -

Chest and Abdominal Radiograph 101
Chest and Abdominal Radiograph 101 Ketsia Pierre MD, MSCI July 16, 2010 Objectives • Chest radiograph – Approach to interpreting chest films – Lines/tubes – Pneumothorax/pneumomediastinum/pneumopericar dium – Pleural effusion – Pulmonary edema • Abdominal radiograph – Tubes – Bowel gas pattern • Ileus • Bowel obstruction – Pneumoperitoneum First things first • Turn off stray lights, optimize room lighting • Patient Data – Correct patient – Patient history – Look at old films • Routine Technique: AP/PA, exposure, rotation, supine or erect Approach to Reading a Chest Film • Identify tubes and lines • Airway: trachea midline or deviated, caliber change, bronchial cut off • Cardiac silhouette: Normal/enlarged • Mediastinum • Lungs: volumes, abnormal opacity or lucency • Pulmonary vessels • Hila: masses, lymphadenopathy • Pleura: effusion, thickening, calcification • Bones/soft tissues (four corners) Anatomy of a PA Chest Film TUBES Endotracheal Tubes Ideal location for ETT Is 5 +/‐ 2 cm from carina ‐Normal ETT excursion with flexion and extension of neck 2 cm. ETT at carina Right mainstem Intubation ‐Right mainstem intubation with left basilar atelectasis. ETT too high Other tubes to consider DHT down right mainstem DHT down left mainstem NGT with tip at GE junction CENTRAL LINES Central Venous Line Ideal location for tip of central venous line is within superior vena cava. ‐ Risk of thrombosis decreased in central veins. ‐ Catheter position within atrium increases risk of perforation Acceptable central line positions • Zone A –distal SVC/superior atriocaval junction. • Zone B – proximal SVC • Zone C –left brachiocephalic vein. Right subclavian central venous catheter directed cephalad into IJ Where is this tip? Hemiazygous Or this one? Right vertebral artery Pulmonary Arterial Catheter Ideal location for tip of PA catheter within mediastinal shadow. -

Pneumothorax Ex Vacuo in a Patient with Malignant Pleural Effusion After Pleurx Catheter Placement
The Medicine Forum Volume 16 Article 20 2015 Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 Thomas Jefferson University, [email protected] Loheetha Ragupathi, MD Thomas Jefferson University, [email protected] Follow this and additional works at: https://jdc.jefferson.edu/tmf Part of the Medicine and Health Sciences Commons Let us know how access to this document benefits ouy Recommended Citation Bhardwaj, MS4, Meera and Ragupathi, MD, Loheetha (2015) "Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement," The Medicine Forum: Vol. 16 , Article 20. DOI: https://doi.org/10.29046/TMF.016.1.019 Available at: https://jdc.jefferson.edu/tmf/vol16/iss1/20 This Article is brought to you for free and open access by the Jefferson Digital Commons. The Jefferson Digital Commons is a service of Thomas Jefferson University's Center for Teaching and Learning (CTL). The Commons is a showcase for Jefferson books and journals, peer-reviewed scholarly publications, unique historical collections from the University archives, and teaching tools. The Jefferson Digital Commons allows researchers and interested readers anywhere in the world to learn about and keep up to date with Jefferson scholarship. This article has been accepted for inclusion in The Medicine Forum by an authorized administrator of the Jefferson Digital Commons. For more information, please contact: [email protected]. Bhardwaj, MS4 and Ragupathi, MD: Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Pneumothorax ex vacuo in a Patient with Malignant Pleural Effusion After PleurX Catheter Placement Meera Bhardwaj, MS4 and Loheetha Ragupathi, MD INTRODUCTION Pneumothorax ex vacuo (“without vaccuum”) is a type of pneumothorax that can develop in patients with large pleural effusions. -
Needs Assessment for New Trauma Center Development in the Commonwealth of Pennsylvania 2014
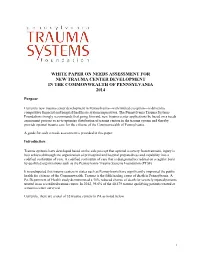
WHITE PAPER ON NEEDS ASSESSMENT FOR NEW TRAUMA CENTER DEVELOPMENT IN THE COMMONWEALTH OF PENNSYLVANIA 2014 Purpose Currently new trauma center development in Pennsylvania—with limited exception—is driven by competitive financial and hospital/healthcare system imperatives. The Pennsylvania Trauma Systems Foundation strongly recommends that going forward, new trauma center applications be based on a needs assessment process so as to optimize distribution of trauma centers in the trauma system and thereby provide optimal trauma care for the citizens of the Commonwealth of Pennsylvania. A guide for such a needs assessment is provided in this paper. Introduction Trauma systems have developed based on the sole precept that optimal recovery from traumatic injury is best achieved through the organization of prehospital and hospital preparedness and capability into a codified continuum of care. A codified continuum of care that is designated/accredited on a regular basis by qualified organizations such as the Pennsylvania Trauma Systems Foundation (PTSF). It is undisputed that trauma centers in states such as Pennsylvania have significantly improved the public health for citizens of the Commonwealth. Trauma is the fifth leading cause of death in Pennsylvania. A Pa. Department of Health study demonstrated a 30% reduced chance of death for severely injured patients treated in an accredited trauma center. In 2012, 95.6% of the 40,479 trauma qualifying patients treated at a trauma center survived. Currently, there are a total of 32 trauma centers in PA as noted below. 1 Figure 1 Source: http://www.rural.palegislature.us/demographics_rural_urban_counties.html As is readily appreciated, the majority of trauma centers are in the most populated counties (Philadelphia and Allegheny) with large areas of the state seemingly having little or no ready access to organized trauma care. -

The Trauma Center Providing Lifesaving Care for Critically Injured Patients
A community newsletter from Antelope Valley Hospital July/August 2017 The Trauma Center Providing Lifesaving Care for Critically Injured Patients Rapid Response Mental Health Services Team Ready to Expansion on Horizon Provide Early Intervention 24/7 In this issue Growing Excellence 2 CEO Message 3 Mental Health Services Right in Your Expansion on Horizon Own Backyard 4 Rapid Response Team Ready to Provide Early Intervention 24/7 5 Hyperbaric Oxygen erapy he previous issue of HealthConnect featured an article describing the Aids in Wound Healing upcoming reopening of our outpatient surgery center through a part - nership between AV Hospital and a local surgery center. In this issue AVH Trauma Center Provides T 6 we’re announcing the expansion of our mental health services. Combined, Lifesaving Care for Critically these two initiatives signify a renewal as well as a change for both our hospital Injured Patients and the overall healthcare in our community. 9 Amazing Person e renewal, of course, is our continued commitment to ensuring that local From Tragedy Comes Sense families don’t need to travel outside the Antelope Valley to receive exceptional of Community for AVH care. at has never been truer than it is today. AV Hospital is a state-of-the-art Employee and Family medical center offering services, technologies and staffing far beyond what would normally be found in a traditional local community hospital. is includes our Hospital Highlights 10 incredible trauma center, which is also featured in this issue. What’s more is Annual Summer Blood Drive that our 450-member medical staff includes primary care physicians, internists 12 and specialists who have been trained at some of the best medical schools and programs in the world. -

TOPIC 2. Airway Patency Impairment. First Aid. Lesson 2 1. Anatomical and Physiological Features of the Respiratory Tract. 2. D
TOPIC 2. Airway patency impairment. First aid. Lesson 2 1. Anatomical and physiological features of the respiratory tract. 2. Definition, causes, types, signs of airway obstruction. 3. Management of airway obstruction. Peculiarities of a foreign body removal from the respiratory tract of a pregnant woman, obese, infants. 4. Technique of ensuring airway patency (head tilt; jaw thrust; insertion of the nasopharyngeal and oropharyngeal airways). 5. Techniques of ventilation (mouth to mouth, mouth to nose, mouth to face mask, Bag-Valve ventilation). 6. Acute respiratory disorders in combat. Pneumothorax: types, signs and symptoms, first aid. Q4. Assessment of the airway patency of the victim. Technique of ensuring airway patency (head tilt; jaw thrust; insertion of the nasopharyngeal and oropharyngeal airways). Assessment of the upper airway of the victim usually requires positioning the individual supine on a flat, firm surface with the arms along the sides of the body. Unless trauma can be definitely excluded, any movement of the victim should consider the possibility of a spine injury. As the patient is placed supine, stabilize the cervical spine by maintaining the head, neck, and trunk in a straight line. If the neck is not already straight, then it should be moved as little as possible to establish the airway. If the patient cannot be placed supine, the jaw thrust maneuver can be applied with the rescuer at the victim’s side. Common causes of airway obstruction in an unconscious patient are occlusion of the oropharynx by the tongue and laxity of the epiglottis. With loss of muscle tone, the tongue or the epiglottis can be forced back into the oropharynx upon inspiration. -
History of EMS and Trauma
Ronald M. Stewart, MD Austin Trauma and Critical Care Conference June 3, 2016 No Disclosures Thank You to: . Robert Winchell, MD . Peter Fischer, MD . Susan Steinemann, MD . Dave Ciesla, MD Current status Brief history of Trauma Centers and Systems Trauma center care as a business-History The problems with “proliferation” Does trauma center level & volume matter? Current COT approach Summary “One may long, as I do, for a gentler flame, a respite, a pause for musing. But perhaps there is no other peace for the artist than what he finds in the heat of combat…Instead, let us seek the respite where it is-in the very thick of battle. For in my opinion…, it is there.” Albert Camus Robert K. Greenleaf; Larry C. Spears. Servant Leadership: A Journey into the Nature of Legitimate Power and Greatness 25th Anniversary Edition 415 ACS Verified Trauma Centers . Roughly and equal number of other TC Intense controversy in many regions . Number and type of trauma center Relevant . Cost . Stability of system . Outcomes and volume? 1913 The American College of Surgeons 1916 Earnest Codman: “A Study of Hospital Efficiency” 1917 ACS: The Hospital Standardization Program becomes the Joint Commission in 1952 1965 SSA—Medicare/Medicaid conditions of participation 6 National Academy of Sciences: Accidental Death and Disability: The neglected disease of modern society: . EMS . Emergency medicine . Trauma Surgeons . Trauma centers and systems Public Hospitals – de facto trauma centers 7 Structure Processes Outcomes (Structure, process, outcome, access, safety, costs and patient experience) 8 Set relevant high standards Build and insure the right infrastructure, leadership and processes aimed at improving quality and reducing mortality. -

Read Onlinepdf 18.98 MB
ResidentOfficial Publication of the Emergency Medicine Residents’ Association December 2018/January 2019 VOL 45 / ISSUE 6 Exertional Rhabdomyolysis EmBassador Travel Team Seeking the Best and Brightest EM Physicians Enjoy the flexibility to live where you want and practice where you are needed. EmBassador TRAVEL TEAM PHYSICIANS RECEIVE: Paid travel and Practice variety accommodations Concierge support Travel convenience package Regional engagements, Paid medical staff dues, equitable scheduling and licenses, certifications and no mandatory long-term applications employment commitment Exceptional Fast track to future compensation package leadership opportunities For More Information: Mansoor Khan, MD National Director, EmBassador Program 917.656.6958 | [email protected] ENVISION PHYSICIAN SERVICES OFFERS ... programs that align physicians to become leaders MANSOOR KHAN, MD, MHA, FAAEM EMERGENCY MEDICINE Why EM Residents choose Envision Physician Services ■ Professional Development and Career Advancement ■ Employment Flexibility: Full-Time, Part-Time, moonlighting and travel team. Employed and Independent Contractor options ■ Practice Variety: Coast-to-coast opportunities at well-recognized hospitals and health systems ■ Unparalleled practice support ■ Earn While You Learn Program: Provides senior residents with $2,500/month while you complete your residency For more information, contact: 877.226.6059 [email protected] TABLE OF CONTENTS EDITORIAL STAFF Categories EDITOR-IN-CHIEF Tommy Eales, DO Indiana University COVER STORY DEPUTY -

Approach to the Trauma Patient Will Help Reduce Errors
The Approach To Trauma Author Credentials Written by: Nicholas E. Kman, MD, The Ohio State University Updated by: Creagh Boulger, MD, and Benjamin M. Ostro, MD, The Ohio State University Last Update: March 2019 Case Study “We have a motor vehicle accident 5 minutes out per EMS report.” 47-year-old male unrestrained driver ejected 15 feet from car arrives via EMS. Vital Signs: BP: 100/40, RR: 28, HR: 110. He was initially combative at the scene but now difficult to arouse. He does not open his eyes, withdrawals only to pain, and makes gurgling sounds. EMS placed a c-collar and backboard, but could not start an IV. What do you do? Objectives Upon completion of this self-study module, you should be able to: ● Describe a focused rapid assessment of the trauma patient using an organized primary and secondary survey. ● Discuss the components of the primary survey. ● Discuss possible pathology that can occur in each domain of the primary survey and recommend treatment/stabilization measures. ● Describe how to stabilize a trauma patient and prioritize resuscitative measures. ● Discuss the secondary survey with particular attention to head/central nervous system (CNS), cervical spine, chest, abdominal, and musculoskeletal trauma. ● Discuss appropriate labs and diagnostic testing in caring for a trauma patient. ● Describe appropriate disposition of a trauma patient. Introduction Nearly 10% of all deaths in the world are caused by injury. Trauma is the number one cause of death in persons 1-50 years of age and results in significant life years lost. According to the National Trauma Data Bank, falls were the leading cause of trauma followed by motor vehicle collisions (MVCs) and firearm related injuries with an overall mortality rate of 4.39% in 2016. -

Clinical Presentation of Patients with Tension Pneumothorax a Systematic Review
META-ANALYSIS Clinical Presentation of Patients With Tension Pneumothorax A Systematic Review Derek J. Roberts, MD,∗†‡§ Simon Leigh-Smith, MBChB,¶ Peter D. Faris, PhD,† Christopher Blackmore, MD,∗ Chad G. Ball, MD, MSc,∗§∗∗ Helen Lee Robertson, MLIS,†† Elijah Dixon, MD, MSc,∗∗∗ Matthew T. James, MD, PhD,†‡‡ Andrew W. Kirkpatrick, MD, MHSc,∗‡§ John B. Kortbeek, MD,∗‡§ and Henry T. Stelfox, MD, PhD†‡‡‡ assisted ventilation who experienced hypotension or cardiac arrest developed Objective: To determine whether the reported clinical presentation of tension these signs within minutes of clinical presentation. pneumothorax differs between patients who are breathing unassisted versus Discussion: The reported clinical presentation of tension pneumothorax de- receiving assisted ventilation. pends on the ventilatory status of the patient. This may have implications for Background: Animal studies suggest that the pathophysiology and physical improving the diagnosis and treatment of this life-threatening disorder. signs of tension pneumothorax differ by subject ventilatory status. Methods: We searched electronic databases through to October 15, 2013 for Keywords: assisted ventilation, breathing unassisted, clinical manifestations, observational studies and case reports/series reporting clinical manifestations clinical presentation, diagnosis, management, signs and symptoms, tension of tension pneumothorax. Two physicians independently extracted clinical pneumothorax manifestations reported at diagnosis. (Ann Surg 2014;00:1–11) Results: We identified 5 cohort studies (n = 310 patients) and 156 case series/reports of 183 cases of tension pneumothorax (n = 86 breathing unas- sisted, n = 97 receiving assisted ventilation). Hypoxia was reported among 43 ension pneumothorax is an uncommon condition with a high (50.0%) cases of tension pneumothorax who were breathing unassisted versus mortality rate most frequently reported to occur in prehospital, 89 (91.8%) receiving assisted ventilation (P < 0.001). -

Anytown Trauma Center Trauma Protocols
ANYTOWN TRAUMA CENTER TRAUMA PROTOCOLS TITLE: TRAUMA TEAM ACTIVATION PROTOCOL PURPOSE: The purpose of the protocol is to establish guidelines for trauma team activation and define the members of the responding trauma team to facilitate the resuscitation and management of critical or seriously injured patients who require rapid, organized resuscitation, evaluation and stabilization to promote optimal outcomes. It also serves to provide triage guidelines for adult and pediatric patients. PROCESS: 1. TRAUMA TEAM ACTIVATION PROTCOL A. The criteria for activation of the trauma team is clearly defined and posted at the Emergency Department triage desk, by the EMS communication station and in the resuscitation rooms. B. The trauma team may be activated prior to arrival based on the EMS communication and their assessment. C. The trauma surgeon, emergency medicine physician, emergency department charge nurse/ house supervisor, emergency department nurses and the Trauma Program Manager may activate the trauma team. D. The person calling the trauma activation will initiate the trauma page to group page the trauma team and will specify the MOI, BP, HR, ETA and level of activation required and age if available. E. If the trauma team members are present in the emergency department and alert is still communicated to ensure everyone is notified. F. Trauma team member notification and arrival times will be documented on the trauma flow sheet (paper or electronic). G. Trauma team members will sign-in when they arrive. H. Trauma team members will be activated for all patients who meet the following criteria: 1. Level 1 trauma activation (major): life threatening injuries and/or unstable vital signs, limb-threating or disability threatening injury 2.