Read Onlinepdf 18.98 MB
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Guidelines for Field Triage of Injured Patients (Regional Modifications Are Permissible)
Arizona Guidelines for Field Triage of Injured Patients (Regional modifications are permissible) FIELD TRIAGE DECISION SCHEME Measure vital signs and level of consciousness Glasgow Coma Scale ≤13 Systolic blood pressure (mmHg) <90 mmHg Step One Respiratory rate <10 or >29 breaths per minute (<20 in infant aged < 1 year1), or need for ventilator support YES NO Transport to a Trauma Center2. Steps 1 and 2 attempt to identify the most seriously injured Assess anatomy of injury. patients. These patients should be transported preferentially to the highest level of care within the trauma system. • All penetrating injuries to head, neck, torso, and extremities proximal to elbow or knee • Chest wall instability or deformity (e.g., flail chest) • Two or more proximal long-bone fractures • Crushed, de-gloved, mangled, or pulseless extremity Step Two3 • Amputation proximal to wrist or ankle • Pelvic fractures • Open or depressed skull fracture • Paralysis YES NO Transport to a Trauma Center2. Steps 1 and 2 attempt to identify the most seriously injured Assess mechanism of injury patients. These patients should be transported preferentially to the highest level of care within the and evidence of high-energy trauma system. impact. • Falls o Adults: >20 feet (one story is equal to 10 feet) 4 o Children : >10 feet or two or three times the height of the child • High-risk auto crash 5 Intrusion , including roof: >12 inches occupant site; >18 inches any site Step Three3 o o Ejection (partial or complete) from automobile o Death in same passenger compartment o Vehicle telemetry data consistent with high risk of injury 6 • Auto vs. -

Edition 2 Trauma Basics
Welcome to the Trauma Alert Education Newsletter brought to you by Beacon Trauma Services. Edition 2 Trauma Basics Trauma resuscitation is the initial stabilization and early life saving interventions provided to the trauma patient. It doesn’t mean that CPR was performed. When assessing the trauma patient it is important to recognize clues that indicate what is wrong now and what could go wrong later. Investigating the mechanism of injury is one of the most important clues to evaluate. This can be done by listening carefully to the MIST report from EMS and utilizing the 60 second time out for EMS to give report Source: https://tinyurl.com/ycjssbr3 What is wrong with me? EMS MIST 43 year old male M= unrestrained driver, while texting drove off road at 40 mph into a tree, with impact to driver’s door, 20 minute extrication time I= Deformity to left femur, pain to left chest, skin pink and warm S= B/P- 110/72, HR- 128 normal sinus, RR- 28, Spo2- 94% GCS=14 (Eyes= 4 Verbal= 4 Motor= 6) T= rigid cervical collar, IV Normal Saline at controlled rate, splint left femur What are your concerns? (think about the mechanism and the EMS report), what would you prepare prior to the patient arriving? Ten minutes after arrival in the emergency department the patient starts to have shortness of breath with stridorous sound. He is now diaphoretic and pale. B/P- 80/40, HR- 140, RR- 36 labored. Absent breath sounds on the left. What is the patients’ underlying problem?- Answer later in the newsletter Excellence in Trauma Nursing Award Awarded in May for National Trauma Month This year the nominations were very close so we chose one overall winner and two honorable mentions. -

Intracranial Hemorrhage As Initial Presentation of Cerebral Venous Sinus Thrombosis
Case Report Journal of Heart and Stroke Published: 31 Dec, 2019 Intracranial Hemorrhage as Initial Presentation of Cerebral Venous Sinus Thrombosis Joseph Y Chu1* and Marc Ossip2 1Department of Medicine, University of Toronto, Canada 2Department of Diagnostic Imaging, William Osler Health System, Canada Abstract Intracranial Hemorrhage (ICH) as initial presentation is an uncommon complication of Cerebral Venous-Sinus Thrombosis (CVT). Clinical and neuro-imaging studies of 4 cases of ICH due cerebral venous-sinus thrombosis seen at the William Osler Health System in Toronto will be presented. Discussion of the immediate and long-term management of these interesting cases will be reviewed with emphasis on the appropriate neuro-imaging studies. Literature review of Direct Oral Anticoagulants (DOAC) in the long-term management of these challenging cases will be discussed. Introduction The following are four cases of Cerebral Venous-Sinus Thrombosis (CVT) who present initially as Intracranial Hemorrhage (ICH). Clinical details, including immediate and long term management and neuro-imaging studies are presented. Results Case 1 A 43 years old R-handed house wife, South-Asian decent, who was admitted to hospital on 06- 10-2014 with sudden headache and right hemiparesis. Her past health shows no prior hypertension or stroke. She is not on any hormone replacement therapy, non-smoker and non-drinker. Married with 1 daughter. Examination shows BP=122/80, P=70 regular, GCS=15, with right homonymous hemianopsia, right hemiparesis: arm=leg 1/5, extensor R. Plantar response. She was started on IV Heparin after her unenhanced CT showed acute left parietal intracerebral hemorrhage and her MRV showed extensive sagittal sinus thrombosis extending into the left transverse OPEN ACCESS sinus (Figures 1,2). -

Early Management of Retained Hemothorax in Blunt Head and Chest Trauma
World J Surg https://doi.org/10.1007/s00268-017-4420-x ORIGINAL SCIENTIFIC REPORT Early Management of Retained Hemothorax in Blunt Head and Chest Trauma 1,2 1,8 1,7 1 Fong-Dee Huang • Wen-Bin Yeh • Sheng-Shih Chen • Yuan-Yuarn Liu • 1 1,3,6 4,5 I-Yin Lu • Yi-Pin Chou • Tzu-Chin Wu Ó The Author(s) 2018. This article is an open access publication Abstract Background Major blunt chest injury usually leads to the development of retained hemothorax and pneumothorax, and needs further intervention. However, since blunt chest injury may be combined with blunt head injury that typically requires patient observation for 3–4 days, other critical surgical interventions may be delayed. The purpose of this study is to analyze the outcomes of head injury patients who received early, versus delayed thoracic surgeries. Materials and methods From May 2005 to February 2012, 61 patients with major blunt injuries to the chest and head were prospectively enrolled. These patients had an intracranial hemorrhage without indications of craniotomy. All the patients received video-assisted thoracoscopic surgery (VATS) due to retained hemothorax or pneumothorax. Patients were divided into two groups according to the time from trauma to operation, this being within 4 days for Group 1 and more than 4 days for Group 2. The clinical outcomes included hospital length of stay (LOS), intensive care unit (ICU) LOS, infection rates, and the time period of ventilator use and chest tube intubation. Result All demographics, including age, gender, and trauma severity between the two groups showed no statistical differences. -

Anaphylaxis and Rhabdomyolysis. Any Early Relationship?
Review Article Crit Care & Shock (2012) 15:88-94 Anaphylaxis and rhabdomyolysis. Any early relationship? Amr S. Omar Abstract Introduction: Rhabdomyolysis (RML) had been identified Results: Both patients survived, both developed RML in different traumatic and non-traumatic conditions; shortly after admission, evidenced by 5-fold or greater few reports described its association with anaphylaxis. increase in serum CPK. They had transient hypotension We report two cases of anaphylaxis both complicated through the presentation, but none of them had persistent with RML. shock requiring vasopressors or complicated with acute renal failure. Aim of the work: To discus the possible casual relation between anaphylaxis and RML and so the value of early Conclusion: We observed rapid increase in serum CPK screening of creatine phosphokinase (CPK) in patients in our two cases suggesting the potential benefits of early with anaphylaxis. assessment of CPK in such patients which may amplify early goal guided management and avoiding logistic Setting: Two patients were enrolled in a multidisciplinary organ dysfunction. intensive care unit. Key words: Rhabdomyolysis, anaphylaxis. Introduction Background Pathophysiology Anaphylaxis is an acute, potentially lethal, multisystem Organ system involvement in anaphylaxis varies from syndrome resulting from the sudden release of mast cell species to species and determines the clinical manifestations and basophile-derived mediators into the circulation. (1) observed. Factors that determine a specific “shock organ” Rhabdomyolysis was first described in the victims of crush include variations in the immune response, the location of injury during the 1940-1941 London, England blitzkrieg smooth muscle, and the distribution, rate of degradation, bombing raids of World War II. -

Symptomatic Intracranial Hemorrhage (Sich) and Activase® (Alteplase) Treatment: Data from Pivotal Clinical Trials and Real-World Analyses
Symptomatic intracranial hemorrhage (sICH) and Activase® (alteplase) treatment: Data from pivotal clinical trials and real-world analyses Indication Activase (alteplase) is indicated for the treatment of acute ischemic stroke. Exclude intracranial hemorrhage as the primary cause of stroke signs and symptoms prior to initiation of treatment. Initiate treatment as soon as possible but within 3 hours after symptom onset. Important Safety Information Contraindications Do not administer Activase to treat acute ischemic stroke in the following situations in which the risk of bleeding is greater than the potential benefit: current intracranial hemorrhage (ICH); subarachnoid hemorrhage; active internal bleeding; recent (within 3 months) intracranial or intraspinal surgery or serious head trauma; presence of intracranial conditions that may increase the risk of bleeding (e.g., some neoplasms, arteriovenous malformations, or aneurysms); bleeding diathesis; and current severe uncontrolled hypertension. Please see select Important Safety Information throughout and the attached full Prescribing Information. Data from parts 1 and 2 of the pivotal NINDS trial NINDS was a 2-part randomized trial of Activase® (alteplase) vs placebo for the treatment of acute ischemic stroke. Part 1 (n=291) assessed changes in neurological deficits 24 hours after the onset of stroke. Part 2 (n=333) assessed if treatment with Activase resulted in clinical benefit at 3 months, defined as minimal or no disability using 4 stroke assessments.1 In part 1, median baseline NIHSS score was 14 (min: 1; max: 37) for Activase- and 14 (min: 1; max: 32) for placebo-treated patients. In part 2, median baseline NIHSS score was 14 (min: 2; max: 37) for Activase- and 15 (min: 2; max: 33) for placebo-treated patients. -
Needs Assessment for New Trauma Center Development in the Commonwealth of Pennsylvania 2014
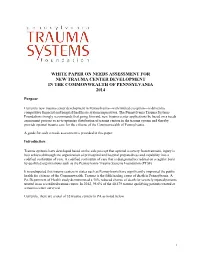
WHITE PAPER ON NEEDS ASSESSMENT FOR NEW TRAUMA CENTER DEVELOPMENT IN THE COMMONWEALTH OF PENNSYLVANIA 2014 Purpose Currently new trauma center development in Pennsylvania—with limited exception—is driven by competitive financial and hospital/healthcare system imperatives. The Pennsylvania Trauma Systems Foundation strongly recommends that going forward, new trauma center applications be based on a needs assessment process so as to optimize distribution of trauma centers in the trauma system and thereby provide optimal trauma care for the citizens of the Commonwealth of Pennsylvania. A guide for such a needs assessment is provided in this paper. Introduction Trauma systems have developed based on the sole precept that optimal recovery from traumatic injury is best achieved through the organization of prehospital and hospital preparedness and capability into a codified continuum of care. A codified continuum of care that is designated/accredited on a regular basis by qualified organizations such as the Pennsylvania Trauma Systems Foundation (PTSF). It is undisputed that trauma centers in states such as Pennsylvania have significantly improved the public health for citizens of the Commonwealth. Trauma is the fifth leading cause of death in Pennsylvania. A Pa. Department of Health study demonstrated a 30% reduced chance of death for severely injured patients treated in an accredited trauma center. In 2012, 95.6% of the 40,479 trauma qualifying patients treated at a trauma center survived. Currently, there are a total of 32 trauma centers in PA as noted below. 1 Figure 1 Source: http://www.rural.palegislature.us/demographics_rural_urban_counties.html As is readily appreciated, the majority of trauma centers are in the most populated counties (Philadelphia and Allegheny) with large areas of the state seemingly having little or no ready access to organized trauma care. -

Canadian Stroke Best Practice Recommendations
CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS MANAGEMENT OF SPONTANEOUS INTRACEREBRAL HEMORRHAGE Seventh Edition - New Module 2020 Ashkan Shoamanesh (Co-chair), M. Patrice Lindsay, Lana A Castellucci, Anne Cayley, Mark Crowther, Kerstin de Wit, Shane W English, Sharon Hoosein, Thien Huynh, Michael Kelly, Cian J O’Kelly, Jeanne Teitelbaum, Samuel Yip, Dar Dowlatshahi, Eric E Smith, Norine Foley, Aleksandra Pikula, Anita Mountain, Gord Gubitz and Laura C. Gioia(Co-chair), on behalf of the Canadian Stroke Best Practices Advisory Committee in collaboration with the Canadian Stroke Consortium and the Canadian Hemorrhagic Stroke Trials Initiative Network (CoHESIVE). © 2020 Heart & Stroke October 2020 Heart and Stroke Foundation Management of Spontaneous Intracerebral Hemorrhage Canadian Stroke Best Practice Recommendations Table of Contents CANADIAN STROKE BEST PRACTICE RECOMMENDATIONS MANAGEMENT OF SPONTANEOUS INTRACERBRAL HEMORRHAGE SEVENTH EDITION, 2020 Table of Contents Topic Page Part One: Canadian Stroke Best Practice Recommendations Introduction and Overview I. Introduction 3 II. Spontaneous Intracerebral Hemorrhage Module Overview 3 III. Spontaneous Intracerebral Hemorrhage Definitions 4 IV. Guideline Development Methodology 4 V. Acknowledgements, Funding, Citation 6 VI. Figure One: Intracerebral Hemorrhage Patient Flow Map 8 Part Two: Canadian Stroke Best Practice Recommendations Spontaneous Intracerebral Hemorrhage 1. Emergency Management of Intracerebral Hemorrhage 9 1.1 Initial Clinical Assessment of Intracerebral Hemorrhage 9 1.2 Blood Pressure Management 10 1.3 Management of Anticoagulation 11 1.4 Consultation with Neurosurgery 12 1.5 Neuroimaging 12 1.5.1 Recommended additional urgent neuroimaging to confirm ICH diagnosis 12 1.5.2 Recommended additional etiological neuroimaging 13 1.6 Surgical management of Intracerebral Hemorrhage 13 Box One: Symptoms of Intracerebral Hemorrhage: 15 Box Two: Modified Boston Criteria (Linn 2010) 16 2. -

The Trauma Center Providing Lifesaving Care for Critically Injured Patients
A community newsletter from Antelope Valley Hospital July/August 2017 The Trauma Center Providing Lifesaving Care for Critically Injured Patients Rapid Response Mental Health Services Team Ready to Expansion on Horizon Provide Early Intervention 24/7 In this issue Growing Excellence 2 CEO Message 3 Mental Health Services Right in Your Expansion on Horizon Own Backyard 4 Rapid Response Team Ready to Provide Early Intervention 24/7 5 Hyperbaric Oxygen erapy he previous issue of HealthConnect featured an article describing the Aids in Wound Healing upcoming reopening of our outpatient surgery center through a part - nership between AV Hospital and a local surgery center. In this issue AVH Trauma Center Provides T 6 we’re announcing the expansion of our mental health services. Combined, Lifesaving Care for Critically these two initiatives signify a renewal as well as a change for both our hospital Injured Patients and the overall healthcare in our community. 9 Amazing Person e renewal, of course, is our continued commitment to ensuring that local From Tragedy Comes Sense families don’t need to travel outside the Antelope Valley to receive exceptional of Community for AVH care. at has never been truer than it is today. AV Hospital is a state-of-the-art Employee and Family medical center offering services, technologies and staffing far beyond what would normally be found in a traditional local community hospital. is includes our Hospital Highlights 10 incredible trauma center, which is also featured in this issue. What’s more is Annual Summer Blood Drive that our 450-member medical staff includes primary care physicians, internists 12 and specialists who have been trained at some of the best medical schools and programs in the world. -

Myoglobinuria, 1984 Lewis P
LE JOURNAL CANAD1EN DES SCIENCES NEUROLOGIQUES CANADIAN NEUROLOGICAL SOCIETY DISTINGUISHED GUEST LECTURE Myoglobinuria, 1984 Lewis P. Rowland This paper was originally presented in June 1982 at the XVII Canadian Congress of Neurological Sciences in Toronto, Ontario where Dr. Rowland was the distinguished guest of the Canadian Neurological Society. Can. J. Neurol. Sci. 1984; 11:1-13 The year is included in the title of this review because the also be important in the pathogenesis of the renal disorder subject is the diversity of conditions that result in myoglobinuria, (Bowden et al., 1956). However, there is reason to believe that and new causes keep appearing as conditions in society change myoglobin (like hemoglobin) is the major nephrotoxin released or new drugs are introduced. The syndrome is often linked to from muscle (Braun et al., 1976). Also, clinical myoglobinuria seamier aspects of society or medicine: war; sadistic drill sergeants; does not occur without muscle necrosis; "rhabdomyolysis" drug abuse; attempted suicide; self-medication or inadequate has been nothing more than a synonym for myoglobinuria for supervision of drug therapy. On the other hand, study of decades. myoglobinuric syndromes has informed us about new hereditable Rarely, rhabdomyolysis has been used in another sense, as a biochemical causes and we have learned more about the action histologic diagnosis, but the old-fashioned term "muscle necro of viruses on muscle. sis" suffices for that purpose and without ambiguity. No The numerous causes of myoglobinuria and the renal effects pathologist could look at an unidentified muscle section and capture the attention of physicians in many different medical proclaim a histologic diagnosis of rhabdomyolysis. -

Spread of Alimentary-Toxic Paroxysmal Myoglobinuria-Haff Disease (Literature Review)
E3S Web of Conferences 254, 09002 (2021) https://doi.org/10.1051/e3sconf/202125409002 FARBA 2021 Spread of alimentary-toxic paroxysmal myoglobinuria-haff disease (literature review) L.A. Glazunova*, A.R. Musina, A.A. Yurchenko, Y.V. Glazunov, and E.M. Gagarin Federal State Budgetary Educational Institution of Higher Education Northern Trans-Ural State Agricultural University, Tyumen, Russia Abstract. In 1924, Haff disease was first detected in East Prussia. Till now, cases of Haff disease have been recorded in Sweden, Russia, the United States, China, Brazil, Japan, and China among people and animals. During the last 40 years, there has been a significant expansion in the geographical range of Haff disease. From 1924 to 2019, 31 outbreaks were recorded in various parts of the world. The total number of victims was about 3,000 people. In Russia, the last cases of human disease were registered in 2019- 2020. In fact, the source of the toxin is fish (crucian carp, carp, pike, burbot, walleye, perch, ruff, ide, yellowtail, black sea bass, eel, silver dollar, brown paku, red paku, cowfish, etc.) or crayfish. Today, the problem of the disease etiology has not been solved; the toxin with the corresponding features has not been isolated, and as a result, causal and pathogenetic treatment of alimentary-toxic paroxysmal myoglobinuria has not been developed. Over this period, several hypotheses were made that are leading in the study of the etiology of the occurrence of Haff disease (thiaminase theory, tannic, arachidonic). This disease-causing substance is known to be heat-resistant and break down the metabolism of skeletal muscles, resulting in the release of myoglobin, which disorders kidney function. -
History of EMS and Trauma
Ronald M. Stewart, MD Austin Trauma and Critical Care Conference June 3, 2016 No Disclosures Thank You to: . Robert Winchell, MD . Peter Fischer, MD . Susan Steinemann, MD . Dave Ciesla, MD Current status Brief history of Trauma Centers and Systems Trauma center care as a business-History The problems with “proliferation” Does trauma center level & volume matter? Current COT approach Summary “One may long, as I do, for a gentler flame, a respite, a pause for musing. But perhaps there is no other peace for the artist than what he finds in the heat of combat…Instead, let us seek the respite where it is-in the very thick of battle. For in my opinion…, it is there.” Albert Camus Robert K. Greenleaf; Larry C. Spears. Servant Leadership: A Journey into the Nature of Legitimate Power and Greatness 25th Anniversary Edition 415 ACS Verified Trauma Centers . Roughly and equal number of other TC Intense controversy in many regions . Number and type of trauma center Relevant . Cost . Stability of system . Outcomes and volume? 1913 The American College of Surgeons 1916 Earnest Codman: “A Study of Hospital Efficiency” 1917 ACS: The Hospital Standardization Program becomes the Joint Commission in 1952 1965 SSA—Medicare/Medicaid conditions of participation 6 National Academy of Sciences: Accidental Death and Disability: The neglected disease of modern society: . EMS . Emergency medicine . Trauma Surgeons . Trauma centers and systems Public Hospitals – de facto trauma centers 7 Structure Processes Outcomes (Structure, process, outcome, access, safety, costs and patient experience) 8 Set relevant high standards Build and insure the right infrastructure, leadership and processes aimed at improving quality and reducing mortality.