Mid Highland CHP Committee Minutes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Emergency Department Activity
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: Apr-10 to Mar-11 Source: A&E data mart, ISD Scotland Date: 07 May 2012 List of Tables Table 1: Attendances and performance against 4-hour standard, Apr-10 to Mar-11 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, Apr-10 to Mar-11 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, Apr-10 to Mar-11 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. -

Accident and Emergency: Performance Update
Accident and Emergency Performance update Prepared by Audit Scotland May 2014 Auditor General for Scotland The Auditor General’s role is to: • appoint auditors to Scotland’s central government and NHS bodies • examine how public bodies spend public money • help them to manage their finances to the highest standards • check whether they achieve value for money. The Auditor General is independent and reports to the Scottish Parliament on the performance of: • directorates of the Scottish Government • government agencies, eg the Scottish Prison Service, Historic Scotland • NHS bodies • further education colleges • Scottish Water • NDPBs and others, eg Scottish Police Authority, Scottish Fire and Rescue Service. You can find out more about the work of the Auditor General on our website: www.audit-scotland.gov.uk/about/ags Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. We help the Auditor General for Scotland and the Accounts Commission check that organisations spending public money use it properly, efficiently and effectively. Accident and Emergency | 3 Contents Summary 4 Key messages 7 Part 1. A&E waiting times 9 Part 2. Reasons for delays in A&E 20 Part 3. Action by the Scottish Government 37 Endnotes 41 Appendix 1. NHS Scotland A&E departments and minor injury units 43 Appendix 2. National context for A&E and unscheduled care, 2004 to 2014 45 Exhibit data When viewing this report online, you can access background data by clicking on the graph icon. The data file will -

Emergency Departments
ED Site List 220711 v2.xls NHS Scotland - Emergency Departments Table 1: NHS Scotland - list of sites providing emergency care File NHS Board Site Type Location Name Location Address Comments Type Ayrshire & Arran ED Ayr Hospital DALMELLINGTON ROAD, AYR, KA6 6DX E Crosshouse Hospital KILMARNOCK ROAD, KILMARNOCK, AYRSHIRE, KA2 0BE E MIU/Other Arran War Memorial Hospital LAMLASH, ISLE OF ARRAN, KA27 8LF A Davidson Cottage Hospital THE AVENUE, GIRVAN, KA26 9DS A Closed from May-10 Girvan Community Hospital BRIDGEMILL, GIRVAN, AYRSHIRE, KA26 9HQ A Opened from May-10 Lady Margaret Hospital COLLEGE ST, MILLPORT, ISLE OF CUMBRAE, KA28 0HF A Opened from Oct-07 Borders ED Borders General Hospital MELROSE, TD6 9BS E MIU/Other Hawick Cottage Hospital VICTORIA ROAD, HAWICK, TD9 7AH A Hay Lodge Hospital NEIDPATH ROAD, PEEBLES, EH45 8JG A Kelso Hospital INCH ROAD, KELSO, TD5 7JP A Knoll Hospital STATION ROAD, DUNS, TD11 3EL A Dumfries & Galloway ED Dumfries & Galloway Royal Infirmary BANKEND ROAD, DUMFRIES, DG1 4AP E Galloway Community Hospital DALRYMPLE STREET, STRANRAER, DG9 7DQ E MIU/Other Castle Douglas Hospital ACADEMY STREET, CASTLE DOUGLAS, DG7 1EE A Kirkcudbright Hospital TOWNEND, KIRKCUDBRIGHT, DG6 4BE A Moffat Hospital HOLMEND, MOFFAT, DG10 9JY A Newton Stewart Hospital NEWTON STEWART, DG8 6LZ A Fife ED Victoria Hospital HAYFIELD ROAD, KIRKCALDY, KY2 5AH E MIU/Other Adamson Hospital BANK STREET, CUPAR, KY15 4JG A Queen Margaret Hospital WHITEFIELD ROAD, DUNFERMLINE, KY12 0SU E St Andrews Memorial Hospital ABBEY WALK, ST ANDREWS, KY16 9LG -

Item 17 on the Agenda)
Mid Highland Community Health Partnership CHP General Manager’s Office Larachan House Docharty Road APPROVAL Dingwall IV15 9UG Telephone: 01349 869221 Fax: 01349 865870 PENDING www.nhshighland.scot.nhs.uk MINUTE of MEETING MID HIGHLAND CHP Friday 28 October 2011 GOVERNANCE COMMITTEE (10.00 am – 2.00 pm) The Moorings Hotel Banavie, Fort William Present: Mr Okain McLennan (Chair) Non Executive Director, Highland NHS Board Mrs Gill McVicar CHP General Manager Mr Tom Slavin CHP Head of Finance Mrs Alison Hudson CHP Lead Nurse Mrs Margaret Moss CHP Lead, Allied Health Professions Mr Findlay Hickey CHP Lead Pharmacist Mr Colin Shields CHP Health & Safety Manager Mrs Tracy Ligema Locality General Manager Lochaber/Out of Hours and Unscheduled Care Development Manager Dr Jim Douglas Clinical Lead, Lochaber Dr Brian Tregaskis Clinical Director, Belford Hospital (from 11.15 am) Mrs Isabelle Campbell Local Councillor, Wester Ross, Strathpeffer & Lochalsh Mr Hamish Fraser Local Councillor, Skye Mr Bren Gormley Local Councillor, Fort William & Ardnamurchan Mr Brian Murphy Local Councillor, Lochaber Mrs Margaret Paterson Local Councillor, Dingwall & Seaforth Ms Sarah Wedgwood Non Executive Member Highland NHS Board Ms Mandy Sillars Area Partnership Forum Representative Mr Gavin Hogg Patient/Public Representative Mr Alan Knox Scottish Ambulance Service Representative In Ms Joanna Hynd Assistant Area Community Care Manager (Ross, Skye Attendance: & Lochaber) By Invitation: Ms Claire Savage CHP Learning & Development Facilitator Ms Michelle Duffy COPD -

Highland Healthvoices Network News
Highland HealthVOICES July 2010 Issue 52 Highland HealthVOICES G U T H S l à i n t e n a G a i d h e a l t a c h d Network News Inside this issue: 1. Forthcoming meetings........................................................................ 1 2. Future health services in West Caithness ........................................ 2 3. New cardiology service for Highland patients.................................. 3 4. Second MRI Scanner introduced at Raigmore Hospital .................. 3 5. Redesign of East Sutherland Midwifery Services ............................ 4 6. Member committee reports ................................................................ 4 7. First Scottish Dementia Strategy launch .......................................... 5 8. Guide dogs change your life .............................................................. 5 9. Nature as a healer................................................................................ 6 10. Improvement work for Ross Memorial Hospital............................ 6 11. Work starts on Action Plan for Skye and Lochalsh...................... 7 12. Breastfeeding Awareness ............................................................... 8 13. On line Stroke Carers Information Project .................................... 8 14. Support needs for patients.............................................................. 8 15. X Programme .................................................................................... 9 16. Falls prevention plan .................................................................... -

Team Update Issue 32 November 2006 N Orth East Floods—A M Ajor Incident for N H S H Ighland
Team Update Issue 32 November 2006 www.nhshighland.scot.nhs.uk N orth East Floods—A M ajor incident for N H S H ighland A multi-agency major incident was called in High- land in response to the storm and flooding on 26 October in East Highland. Management Teams and staff in Ross and Cro- marty and Caithness and Sutherland co-ordinated actions and interventions for the continuity for ser- vices in these areas and support for other agen- cies. The level of risk was assessed with regard to po- tential flooding and loss of sanitation at Ross Me- morial Hospital. Staff liased throughout with Scot- tish Ambulance Service and with Raigmore Hospi- tal over the possible need to evacuate patients. The situation with regard to hospital services at Dingwall was under constant assessment and re- Picture: Anne Macleod, Senior Radiographer and Tina assessment and the high tide passed without inci- Rae, Enrolled Nurse, Ross Memorial Hospital. dent. Management also kept in touch with the OOH hub Service Continuity Group, which has been set up to ensure there was appropriate OOH doctor cov- to review and harmonise NHS Highland’s Major erage in light of the road closures and worsening Incident Plan and Service Continuity arrange- weather expected. ments. Highland Council contacted Ross Memorial Hospi- tal for the supply of blankets and towels for several evacuated people. Public Holiday Dates are on “Everyone was superb, calm and supportive of oth- ers, all pulling together, considered in their re- p ag e 5 sponses and going that extra little bit that makes these things easier to manage. -
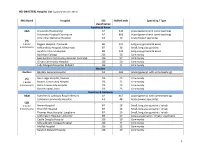
MASTER) Hospital List (Updated October 2015
HEI (MASTER) Hospital List (updated October 2015) NHS Board Hospital ISD Staffed beds Speciality / Type classification Ayrshire & Arran A&A University Hospital Ayr A2 343 Acute (general with some teaching) University Hospital Crosshouse A2 666 Acute (general with some teaching) Arran War Memorial Hospital A3 19 Acute (mixed speciality) (9) 3 acute Biggart Hospital, Prestwick B6 121 Long stay geriatric & acute 6 community Kirklandside Hospital, Kilmarnock B7 36 Small, long stay geriatric Ayrshire Central Hospital B8 142 Long stay geriatric & acute Davidson Cottage J26 26 Community East Ayrshire Community Hospital, Cumnock J26 57 Community Girvan Community Hospital J26 20 Community Lady Margaret Hospital, Millport J26 9 Community Borders Borders Borders General Hospital A2 265 Acute (general, with some teaching) (5) Hay Lodge Hospital, Peebles J26 23 Community 1 acute Hawick Community Hospital J26 22 Community 4 community Kelso Community Hospital J26 23 Community Knoll Hospital, Duns J26 23 Community Dumfries & Galloway D&G Dumfries & Galloway Royal Infirmary A2 367 Acute (general, with some teaching) Galloway Community Hospital A3 48 Acute (mixed speciality) (10) 2 acute Annan Hospital B7 18 Small, long stay geriatric / rehab 8 community Thornhill Hospital B7 13 Small, long stay geriatric / rehab Thomas Hope Hospital, Langholm B7 10 Small, long stay geriatric / rehab Lochmaben Hospital, Lockerbie B9 17 Long stay geriatric / rehab / psychiatry Castle Douglas Hospital J26 19 Community Kirkcudbright Cottage Hospital J26 9 Community Moffat Hospital J26 12 Community Newton Stewart Hospital J26 19 Community 1 HEI (MASTER) Hospital List (updated October 2015) Fife Fife Victoria Hospital, Kirkcaldy A2 621 Acute (general with some teaching) (7) Queen Margaret Hospital, Dunfermline A3 196 Acute (mixed speciality) 2 acute 5 community Cameron Hospital, Leven B7 95 Small, long stay geriatric Adamson Hospital, Cupar J26 19 Community Glenrothes Hospital J26 74 Community Randolph Wemyss Memorial Hospital J26 16 Community St. -

Remembering the Strathpeffer Area: 1. Jamestown
Remembering the Strathpeffer Area: 1. Jamestown During 2015 people gathered at Strathpeffer Community Centre and Achterneed Hall to remember the physical remains of the Strathpeffer area – Jamestown, Strathpeffer, the Heights, Achterneed and Milnain – focussing on buildings, sites, or monuments which were new, modified or no longer there. They built on previous sessions which had begun to look at Strathpeffer. Using old maps, photographs (some more than a century old), various printed sources, and memories spanning over 80 years, information about over 350 sites was gathered. Some pupils from the school joined us as well for Strathpeffer sessions as part of their project investigating World War II. This report summarises the results of the meetings focussing on Jamestown, with a few extra memories of places further west. The details have also been forwarded to heritage databases: the Highland Council Historic Environment Record (HER) (her.highland.gov.uk) and Historic Environment Scotland’s Canmore (canmore.org.uk) where they will provide valuable new information about the heritage of the area. The 2015 sessions were part of a project organised by ARCH and Strathpeffer Community Centre, and funded by the Heritage Lottery Fund and the Mackenzie New York Villa Trust. Funding for the smaller projects in previous years was provided by Generations Working Together and High Life Highland. Thanks also to the Highland Museum of Childhood for allowing us to see text panels from their 2009 ‘Hands Across the Sea’ exhibition. But most of all thanks to everyone who has shared their memories and photographs, often braving difficult weather. Any additions or corrections should be sent to ARCH at [email protected] or The Goods Shed, The Old Station, Strathpeffer, IV14 9DH. -

North and West Operational Unit Occupational Therapy & Physiotherapy Leadership and Management Structure – January 2015
North and West Operational Unit Occupational Therapy & Physiotherapy Leadership and Management structure – January 2015 Within North and West Unit we have leads for both Occupational Therapy and Physiotherapy who have area wide governance roles for these professions and they link into the Highland wide governance networks for their profession. All Allied Health Professional staff are professionally led by those listed in the tables below and operationally managed via an integrated team structure within districts which sit under an area and Unit level management structure to the Director of Operations. Our only Mental Health Occupational Therapist is operationally managed in the Mental Health Integrated Team but professionally reports to the Lead Occupational Therapist within their area. Name Profession Post Base Dawn Mohun OT North Area Professional Migdale Hospital Lead Cherry Grove Bonar Bridge IV24 3ER Kerry Watson OT West Area Professional Kyle Health Centre, Lead Station Road Kyle of Lochalsh IV40 8AE Liz Morrison Physio Acting West Area Fort Willian Health Centre Professional Lead Fort William Lochaber PH33 7AQ Shona Paterson Physio North Area Professional Lawson Memorial Hospital Lead Golspie Sutherland KW10 6SS South and Mid Unit Management Structure Within South & Mid we have Unit Leads for both Occupational Therapy and Physiotherapy who have unit wide governance roles for these professions and they link into the Highland wide governance networks for their profession. Community Physiotherapy and Occupational Therapy sits within -

ED Pub 4Hr 2009-10
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: 2009/10 (Apr-09 to Mar-10) Source: A&E data mart, ISD Scotland Date: 04 August 2011 List of Tables Table 1: Attendances and performance against 4-hour standard, 2009/10 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, 2009/10 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, 2009/10 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. 4) The information presented is based on data under development, the quality and accuracy are being monitored. -

Scotland) 15 June 2021
Version 1.6 (Scotland) 15 June 2021 ISARIC/WHO Clinical Characterisation Protocol UK (Scotland) Recruitment Procedures for FRONTLINE CLINICAL RESEARCH STAFF The most up to date versions of the protocol and case report form are available at isaric4c.net/protocols/ A virtual site visit is available at isaric4c.net/virtual_site_visit/ AIM: Please recruit the following patients only: • Vaccine failure (positive COVID test - rather than displaying symptoms – >28d after having received a vaccine) • Reinfection (proven after proven) • Co-infection (flu/RSV) • COVID associated hyper inflammation (MIS-A/MIS-C/PINS-TS) at any age • Samples from patients with pathogens of public health interest including people identified as infected with SARS-CoV “variants of concern” • All children CONSENT: once the form is signed by a participant it is hazardous. To record consent, we suggest an independent witness observes the completed form then signs a fresh copy outside of the isolation area. Consent can also be obtained by telephone from participants or from relatives for proxy consent. RECRUITMENT PACKS: Sample collection kits will be supplied to sites. Sample collections kits can be requested from: [email protected] Each kit will have a specific kit ID number, with each component within showing this kit ID and its own respective component ID for audit purposes. Pods and bio-bags for shipping will also be supplied to sites. These can be requested from [email protected] OBTAIN SAMPLES according to the schedule. You can find out which tier you are operating at in the front page of the site file. If you have capacity to recruit at TIER 2: Day 1 2 3 4 5 6 7 8 9 28 days after discharge Samples R S S C Sample priority 1 2 3 4 R: recruitment sample; S: serial sample; C: convalescent sample. -

FOI Act Report - Asbestos Removal / Repair Works by Company and Year - Maximo 7.6
10/02/2017 FOI Act Report - Asbestos Removal / Repair Works By Company and Year - Maximo 7.6 NASBESTOS - NORTHERN ASBESTOS SERVICES LTD 2016 Order Number Order Description Location GL Account Number Order Date Total Cost HMD 1059 Northern Asbestos Services sample taken for analysis from insulation material at Raigmore HNS 158-00001-3019 21/01/2016 £ 50.00 HMD 1887 Carry out removal of asbestos seal from window frame at Boiler House, Raigmore H28/Z09/1638 HNS 158-00001-3012 07/03/2016 £ 422.40 HMD 3646 Carry out emergency removal/disposal of fibre cement board at Maternity Entrance H28/Z08/00/1631 HNS 158-00001-3019 13/06/2016 £ 360.00 HMD 5328 carry out refurbishment & demolition survey on flat roof - RMH H29/00 HNS 149-00001-3019 15/09/2016 £ 471.00 HMD 6147 Portree Hospital Generator room Asbestos removal. Northern Asbestos quote ref 6725/DC2. MH -H27 H99999-00001-A411-HCNH 0396 31/10/2016 £ 6,534.00 ROBERTMCGREG - Robertson McGregor Property Solutions Ltd (RMG ) 2016 Order Number Order Description Location GL Account Number Order Date Total Cost HMD 4572 Asbestos Consultancy Services, per Quote IM/Q1237 dated 6 May 2016 SH -F16 HNR 143-00001-3019 04/08/2016 £ 24 ,228.00 HMD 4809 Carry out demolition and refurbishment survey of Drum Court, Accommodation Block, Raigmore RG -H28 HNS 166-00001-3019 19/08/2016 £ 1,674.00 HMD 5046 Air Sampling for removal of asbestos containing material from Drum Court Accommodation at Raigmore RG -H28 HNS 166-00001-3019 01/09/2016 £ 1,980.00 HMD 5469 Asbestos Consultancy Services - additional training & taking/analysing sample RG -H28 HNS 166-00001-3019 22/09/2016 £ 480.00 HMD 5582 To test for Asbestos for Hotel Services at Belford MH -H11 HEB 028-00001-3019 30/09/2016 £ 81.60 HMD 6398 RMG Property Services Asbestos Survey, Plant Rooms, Raigmore (Ryan Muffett) RG -H28 H99999-00001-A411-HCNH 0404 14/11/2016 £ 3,594.00 HMD 6510 RMG to carry out an asbestos survey at Assynt House (Z.