Formulae for Afferent and Efferent Arteriolar Resistance in the Human Kidney: an Application to the Effects of Spinal Anesthesia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Excretory Products and Their Elimination
290 BIOLOGY CHAPTER 19 EXCRETORY PRODUCTS AND THEIR ELIMINATION 19.1 Human Animals accumulate ammonia, urea, uric acid, carbon dioxide, water Excretory and ions like Na+, K+, Cl–, phosphate, sulphate, etc., either by metabolic System activities or by other means like excess ingestion. These substances have to be removed totally or partially. In this chapter, you will learn the 19.2 Urine Formation mechanisms of elimination of these substances with special emphasis on 19.3 Function of the common nitrogenous wastes. Ammonia, urea and uric acid are the major Tubules forms of nitrogenous wastes excreted by the animals. Ammonia is the most toxic form and requires large amount of water for its elimination, 19.4 Mechanism of whereas uric acid, being the least toxic, can be removed with a minimum Concentration of loss of water. the Filtrate The process of excreting ammonia is Ammonotelism. Many bony fishes, 19.5 Regulation of aquatic amphibians and aquatic insects are ammonotelic in nature. Kidney Function Ammonia, as it is readily soluble, is generally excreted by diffusion across 19.6 Micturition body surfaces or through gill surfaces (in fish) as ammonium ions. Kidneys do not play any significant role in its removal. Terrestrial adaptation 19.7 Role of other necessitated the production of lesser toxic nitrogenous wastes like urea Organs in and uric acid for conservation of water. Mammals, many terrestrial Excretion amphibians and marine fishes mainly excrete urea and are called ureotelic 19.8 Disorders of the animals. Ammonia produced by metabolism is converted into urea in the Excretory liver of these animals and released into the blood which is filtered and System excreted out by the kidneys. -

Renal Corpuscle Renal System > Histology > Histology
Renal Corpuscle Renal System > Histology > Histology Key Points: • The renal corpuscles lie within the renal cortex; • They comprise the glomerular, aka, Bowman's capsule and capillaries The capsule is a double-layer sac of epithelium: — The outer parietal layer folds upon itself to form the visceral layer. — The inner visceral layer envelops the glomerular capillaries. • As blood passes through the glomerular capillaries, aka, glomerulus, specific components, including water and wastes, are filtered to create ultrafiltrate. • The filtration barrier, which determines ultrafiltrate composition, comprises glomerular capillary endothelia, a basement membrane, and the visceral layer of the glomerular capsule. • Nephron tubules modify the ultrafiltrate to form urine. Overview Diagram: • Tuft of glomerular capillaries; blood enters the capillaries via the afferent arteriole, and exits via efferent arteriole. • The visceral layer of the glomerular capsule envelops the capillaries, then folds outwards to become the parietal layer. • The capsular space lies between the parietal and visceral layers; this space fills with ultrafiltrate. • Vascular pole = where the arterioles pass through the capsule • Urinary pole = where the nephron tubule begins • Distal tubule passes by the afferent arteriole. Details of Capillary and Visceral Layer: • Fenestrated glomerular capillary; fenestrations are small openings, aka, pores, in the endothelium that confer permeability. • Thick basement membrane overlies capillaries • Visceral layer comprises podocytes: — Cell bodies — Cytoplasmic extensions, called primary processes, give rise to secondary foot processes, aka, pedicles. • The pedicles interdigitate to form filtration slits; molecules pass through these slits to form the ultrafiltrate in the 1 / 3 capsular space. • Subpodocyte space; healthy podocytes do not adhere to the basement membrane. Clinical Correlation: • Podocyte injury causes dramatic changes in shape, and, therefore, their ability to filter substances from the blood. -

Kidney Function • Filtration • Reabsorption • Secretion • Excretion • Micturition
About This Chapter • Functions of the kidneys • Anatomy of the urinary system • Overview of kidney function • Filtration • Reabsorption • Secretion • Excretion • Micturition © 2016 Pearson Education, Inc. Functions of the Kidneys • Regulation of extracellular fluid volume and blood pressure • Regulation of osmolarity • Maintenance of ion balance • Homeostatic regulation of pH • Excretion of wastes • Production of hormones © 2016 Pearson Education, Inc. Anatomy of the Urinary System • Kidneys, ureters, bladder, and urethra • Kidneys – Bean-shaped organ – Cortex and medulla © 2016 Pearson Education, Inc. Anatomy of the Urinary System • Functional unit is the nephron – Glomerulus in the Bowman’s capsule – Proximal tubule – The loop of Henle • Descending limb and ascending limb twisted between arterioles forming the juxtaglomerular apparatus – Distal tubule – Collecting ducts © 2016 Pearson Education, Inc. Figure 19.1b Anatomy summary The kidneys are located retroperitoneally at the level of the lower ribs. Inferior Diaphragm vena cava Aorta Left adrenal gland Left kidney Right kidney Renal artery Renal vein Ureter Peritoneum Urinary Rectum (cut) bladder (cut) © 2016 Pearson Education, Inc. Figure 19.1c Anatomy summary © 2016 Pearson Education, Inc. Figure 19.1d Anatomy summary © 2016 Pearson Education, Inc. Figure 19.1f-h Anatomy summary Some nephrons dip deep into the medulla. One nephron has two arterioles and two sets of capillaries that form a portal system. Efferent arteriole Arterioles Peritubular Juxtaglomerular capillaries The cortex apparatus contains all Bowman’s Nephrons Afferent capsules, arteriole Glomerulus proximal Juxtamedullary nephron and distal (capillaries) with vasa recta tubules. Peritubular capillaries Glomerulus The medulla contains loops of Henle and Vasa recta collecting ducts. Collecting duct Loop of Henle © 2016 Pearson Education, Inc. -

Urinary System
OUTLINE 27.1 General Structure and Functions of the Urinary System 818 27.2 Kidneys 820 27 27.2a Gross and Sectional Anatomy of the Kidney 820 27.2b Blood Supply to the Kidney 821 27.2c Nephrons 824 27.2d How Tubular Fluid Becomes Urine 828 27.2e Juxtaglomerular Apparatus 828 Urinary 27.2f Innervation of the Kidney 828 27.3 Urinary Tract 829 27.3a Ureters 829 27.3b Urinary Bladder 830 System 27.3c Urethra 833 27.4 Aging and the Urinary System 834 27.5 Development of the Urinary System 835 27.5a Kidney and Ureter Development 835 27.5b Urinary Bladder and Urethra Development 835 MODULE 13: URINARY SYSTEM mck78097_ch27_817-841.indd 817 2/25/11 2:24 PM 818 Chapter Twenty-Seven Urinary System n the course of carrying out their specific functions, the cells Besides removing waste products from the bloodstream, the uri- I of all body systems produce waste products, and these waste nary system performs many other functions, including the following: products end up in the bloodstream. In this case, the bloodstream is ■ Storage of urine. Urine is produced continuously, but analogous to a river that supplies drinking water to a nearby town. it would be quite inconvenient if we were constantly The river water may become polluted with sediment, animal waste, excreting urine. The urinary bladder is an expandable, and motorboat fuel—but the town has a water treatment plant that muscular sac that can store as much as 1 liter of urine. removes these waste products and makes the water safe to drink. -
Studies from the Institute of Pathology, No. 14 A
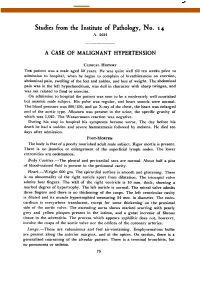
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by PubMed Central Studies from the Institute of Pathology, No. 14 A. 5691 A CASE OF MALIGNANT HYPERTENSION CLINICAI HISTORY THE patient was a male aged 50 years. He was quite well till ten weeks prior to admission to hospital, when he begani to complain of breathlessness on exertion, abdominal pain, swelling of the feet and ankles, and loss of weight. The abdominal pain was in the left hypochondrium, was dull in character with sharp twinges, and was not related to food or exercise. On admission to hospital the patient was seen to be a moderately well nourished but anamic male subject. His pulse was regular, and heart sounds were normal. The blood pressure was 200'/150, and on X-ray of the chest, the heart was enlarged and of the aortic type. Albumen was present in the urine, the specific gravity of which was 1,025. The Wassermann reaction was negative. During his stay in hospital his symptoms became worse. The day before his death he had a sudden and severe hkematemesis followed by melkna. He died ten days after admission. POST-MORTEM The body is that of a poorly nourished adult male subject. Rigor mortis is present. There is no jaundice or enlargement of the superficial lymph nodes. The lower extremities are oedematous. Body Cavities.-The pleural and pericardial sacs are normal. About half a pint of blood-stained fluid is present in the peritoneal cavity. Heart.-Weight 600 gm. The epicardial surface is smooth and glistening. -

The Distal Convoluted Tubule and Collecting Duct
Chapter 23 *Lecture PowerPoint The Urinary System *See separate FlexArt PowerPoint slides for all figures and tables preinserted into PowerPoint without notes. Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Introduction • Urinary system rids the body of waste products. • The urinary system is closely associated with the reproductive system – Shared embryonic development and adult anatomical relationship – Collectively called the urogenital (UG) system 23-2 Functions of the Urinary System • Expected Learning Outcomes – Name and locate the organs of the urinary system. – List several functions of the kidneys in addition to urine formation. – Name the major nitrogenous wastes and identify their sources. – Define excretion and identify the systems that excrete wastes. 23-3 Functions of the Urinary System Copyright © The McGraw-Hill Companies, Inc. Permission required for reproduction or display. Diaphragm 11th and 12th ribs Adrenal gland Renal artery Renal vein Kidney Vertebra L2 Aorta Inferior vena cava Ureter Urinary bladder Urethra Figure 23.1a,b (a) Anterior view (b) Posterior view • Urinary system consists of six organs: two kidneys, two ureters, urinary bladder, and urethra 23-4 Functions of the Kidneys • Filters blood plasma, separates waste from useful chemicals, returns useful substances to blood, eliminates wastes • Regulate blood volume and pressure by eliminating or conserving water • Regulate the osmolarity of the body fluids by controlling the relative amounts of water and solutes -

Urinary System Kidney Anatomy Nephrons Let's Make the Filtrate
Kidney anatomy Urinary system Renal Aids homeostasis by cortex removing cellular wastes and Renal medulla foreign compounds, and Cortex maintains salt and water Renal balance of plasma pelvis Medulla Ureter Nephrons Let’s make the filtrate... Each kidney has about one million nephrons Blood is filtered at the glomerulus. Water Afferent arteriole brings and solutes leave the blood to glomerulus and blood and enter then forms efferent Bowman’s capsule. arteriole. Efferent arteriole branches to peritubular capillaries 1 Glomerulus physiology Bowman’s capsule contains podocytes that encircle Glomerular filtration the glomerulus. Glomerular filtration Normally blood cells and plasma proteins are not is similar to Capillary filtered ultrafiltration of 55 blood pressure capillaries Osmotic Hydrostatic 20% of plasma pressure 30 15 pressure becomes filtrate Glomerular filtration rate (GFR) determined by: Net filtration pressure and glomerulus permeability Adjusting GFR Filtrate is adjusted along the nephron Distal Blood pressure tubule Proximal tubule Cortex region Bowman’s capsule Radius of afferent arteriole Juxtaglomerular apparatus - helps in Decreasing GFR helps retain adjustments to filtration rate fluid and salts Loop of Henle Medulla region 2 Tubular reabsorption and secretion 180 liters per day are filtered, most is reabsorbed Reabsorption: filtered substances leave the nephron and enter peritubular capillaries Secretion: some substances from the peritubular capillaries enter the nephron So what is urine, then? Everything in the nephron that does not get Reabsorption physiology reabsorbed into the blood leaves as ….urine!!! 3 + Reabsorption of Na + (the key to it all…) Na reabsorption Na+ reabsorption (RA) drives the movement of many other substances in the tubule Water will “follow” Na+ movement Lumen Proximal tubular cell Control of sodium RA Page 533 When ECF volume is low, need to Na+ RA Osmosis Interstitial fluid Peritubular + Water capillary Na RA at distal and collection tubules with channel aldosterone. -
Introduction to the Urinary System
Tips for Success 1. Show up 2. Participate in lab 3. Show up 4. Turn in assignments (completed, refer to #6) 5. Show up 6. Communicate with me, e-mail is best 7. Show up Every point counts! Business Homework due in lab Label the handout provided today Front and back Use your book! There should be at least 18 items labeled Part 1 Urinary System Wastes Gases versus fluids Urinary system Dispose of water soluble wastes Electrolyte regulation Acid-base regulation Urinary System Other functions Kidneys Renin Erythropoietin Vitamin D activation Nitrogenous Wastes Urine is about 95% water Second largest component is urea Urea derived from breakdown of amino acids Nitrogenous Wastes TOXIC! + 1. Dietary amino acids → NH2 removed → NH2 + H → NH3 500 ml of urine removes only 1 gram of nitrogen as ammonia 2. Ammonia can be converted to urea Requires energy 50 ml of urine removes 1 gram of nitrogen as urea 3. Ammonia can be converted to uric acid Requires lots of energy 10 ml of urine removes 1 gram of nitrogen as uric acid Urinary System Organs Kidneys Major excretory organs Urinary bladder Temporary storage reservoir for urine Ureters Transport urine from the kidneys to the bladder Urethra Transports urine out of the body Hepatic veins (cut) Esophagus (cut) Inferior vena cava Renal artery Adrenal gland Renal hilum Aorta Renal vein Kidney Iliac crest Ureter Rectum (cut) Uterus (part of female reproductive Urinary system) bladder Urethra Figure 25.1 Kidney: Urinary System page 6 Anterior Inferior vena cava Peritoneal -

Chapter 4 Central Nervous System and Sensory Organs
Chapter 4 Central Nervous System and Sensory Organs © David G. Ward © David Dendrites of Neuron Showing Dendritic Spines (Brighteld, Silver, x1880) 79 Sensory and Motor Neurons Cell Body Synaptic Bulb Dendrite / Receptor Axon (Central Process) Axon (Peripheral Process) Figure 4.1: Unipolar neuron (sensory). © David G. Ward. Dendrites Dendrites Cell Body Axon Hillock Synaptic Bulb Dendrites Axon Figure 4.2: Multipolar neuron (motor). © David G. Ward. 80 Chapter 4: Central Nervous System and Sensory Organs Communication Between Neurons Cell Body Dendrites Axon Cell Body Enlargement Synaptic Axon Synaptic Bulb Hillock Vesicles Synaptic Bulb Presynaptic Axon Membrane Postsynaptic Membrane Dendrite Synaptic Cleft Figure 4.3: Synaptic communication. © David G. Ward. Synaptic Bulb* Axon Dendrite Dendrite Synaptic Bulb* Synaptic Bulb Nucleus Axon Synaptic Vessicles *The synaptic bulbs are from other neurons communicating with this neuron. Presynaptic Membrane Figure 4.4: Mutlipolar neuron. Figure 4.5: Synaptic bulb. © David G. Ward. © David G. Ward. Chapter 4: Central Nervous System and Sensory Organs 81 Motor Neurons, Glial and Schwann Cells Multipolar Neurons Glial Cells Figure 4.6: Spinal multipolar neurons. © David G. Ward. Node Node Schwann Cell Axon Endoneurium Axon Myelin Sheath Figure 4.7: Myelinated neuron. © David G. Ward. Axon Node Axon Schwann Cell Schwann Cell 400x+ Axon Schwann Cell / Myelin Sheath Figure 4.8: Schwann cell. © David G. Ward. 82 Chapter 4: Central Nervous System and Sensory Organs Nerve and Schwann Cells Fascicle Perineurium Epineurium Perineurium Epineurium Fascicle Figure 4.9: Nerve cell, histology. © David G. Ward. Epineurium Perineurium Endoneurium Axons Perineurium Perineurium Fascicle Figure 4.10: Nerve. Figure 4.11: Nerve fascicle. -

Juxtamedullary Afferent and Efferent Arterioles Constrict to Renal Nerve Stimulation
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Kidney International, Vol. 44 (1993), pp. 684—691 Juxtamedullary afferent and efferent arterioles constrict to renal nerve stimulation JING CHEN and JOHN T. FLEMING Department of Physiology and Biophysics, School of Medicine, University of Louisville, and Center for Applied Microcirculatory Research, Louisville, Kentucky, USA Juxtamedullary afferent and efferent arterioles constrict to renal nerve preferential preglomerular action may not be applicable to the stimulation. Sympathetic neural control of afferent and efferent arteri- arterioles of inner cortical (juxtamedullary) glomeruli. oles of inner cortical (juxtamedullary) glomeruli has not been estab- lished, in part, because of difficulty accessing these vessels, normally A reduction of medullary blood flow during renal nerve located deep below the kidney surface. In this study we utilized the rat stimulation [15] confirms the histological evidence for innerva- hydronephrotic kidney model to visualize the renal microcirculation tion of vessels in the inner cortex [2, 3, 12, 14, 20]. However, and to quantitate the responses ofjuxtamedullary arterioles to brief (30 these data do not provide evidence for the relative response of see) renal nerve stimulation (RNS). Juxtamedullary afferent and effer- ent arterioles constricted in a frequency-dependent fashion to RNS, the pre- versus postglomerular vessels to nerve stimulation. achieving a maximal constriction of 35% to 8 Hz stimulation. In these According to Gorgas [14], the juxtamedullary efferent arterioles same kidneys, outer cortical afferent arterioles also constricted to RNS are surrounded by a denser nerve plexus than cortical efferent but outer cortical efferent arterioles did not. -

Pressure Induces Intracellular Calcium Changes in Juxtaglomerular Cells in Perfused Afferent Arterioles
Hypertension Research (2011) 34, 942–948 & 2011 The Japanese Society of Hypertension All rights reserved 0916-9636/11 www.nature.com/hr ORIGINAL ARTICLE Pressure induces intracellular calcium changes in juxtaglomerular cells in perfused afferent arterioles En Yin Lai1,3,5, Yibing Wang2,4,5, Anders Erik Gosta Persson1, Roy Davis Manning Jr2 and Ruisheng Liu2 Calcium (Ca2+) has an important role in nearly all types of cellular secretion, with a particularly novel role in the juxtaglomerular (JG) cells in the kidney. In JG cells, Ca2+ inhibits renin secretion, which is a major regulator of blood pressure and renal hemodynamics. However, whether alterations in afferent arteriolar (Af-Art) pressure change intracellular Ca2+ concentration 2+ 2+ ([Ca ]i) in JG cells and whether [Ca ]i comes from extracellular or intracellular sources remains unknown. We hypothesize 2+ that increases in perfusion pressure in the Af-Art result in elevations in [Ca ]i in JG cells. We isolated and perfused Af-Art of 2+ 2+ C57BL6 mice and measured changes in [Ca ]i in JG cells in response to perfusion pressure changes. The JG cells’ [Ca ]i was 93.3±2.2 nM at 60 mm Hg perfusion pressure and increased to 111.3±13.4, 119.6±7.3, 130.3±2.9 and 140.8±12.1 nM 2+ at 80, 100, 120 and 140 mm Hg, respectively. At 120 mm Hg, increases in [Ca ]i were reduced in mice receiving the following treatments: (1) the mechanosensitive cation channel blocker, gadolinium (94.6±7.5 nM); (2) L-type calcium channel blocker, nifedipine (105.8±7.5 nM); and (3) calcium-free solution plus ethylene glycol tetraacetic acid (96.0±5.8 nM). -
The Morphology of the Afferent and Efferent Domain of the Sheep Glomerulus
ONLINE FIRST This is a provisional PDF only. Copyedited and fully formatted version will be made available soon. ISSN: 0015-5659 e-ISSN: 1644-3284 The morphology of the afferent and efferent domain of the sheep glomerulus Authors: K. Aycan, T. Ulcay, B. Kamaşak DOI: 10.5603/FM.a2020.0124 Article type: ORIGINAL ARTICLES Submitted: 2020-04-09 Accepted: 2020-09-16 Published online: 2020-10-12 This article has been peer reviewed and published immediately upon acceptance. It is an open access article, which means that it can be downloaded, printed, and distributed freely, provided the work is properly cited. Articles in "Folia Morphologica" are listed in PubMed. Powered by TCPDF (www.tcpdf.org) The morphology of the afferent and efferent domain of the sheep glomerulus Running Head: The morphology of the sheep glomerulus K. Aycan, T. Ulcay, B. Kamaşak Department of Anatomy, Faculty of Medicine, Kırşehir Ahi Evran University, Kırşehir, Turkey Address for correspondence: Prof. Dr. Kenan Aycan, Department of Anatomy, Faculty of Medicine, Kırşehir Ahi Evran University, Kırşehir, Turkey, tel: + 90 533 6405660, e-mail: [email protected] ABSTRACT Background: It is important to know the morphology of the glomerulus in order to explain kidney infiltration. The present study aims to research the morphology of afferent and efferent domains of sheep kidney glomeruli. Materials and methods: In this study, 2000 glomeruli from 20 kidneys of Akkaraman sheep were examined using the polyester resin method. Results: It was found that the glomeruli of sheep kidney usually have an afferent arteriole as well as an efferent arteriole. Besides, it was also found that five glomeruli have two efferent arterioles.