Predictive Factors for Invasive Fungal Rhinosinusitis in Diabetic Patients: Systematic Review and Data Re-Analysis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Epidemiological, Clinical and Diagnostic Aspects of Sheep Conidiobolomycosis in Brazil
Ciência Rural, Santa Maria,Epidemiological, v.46, n.5, p.839-846, clinical mai, and 2016 diagnostic aspects of sheep conidiobolomycosis http://dx.doi.org/10.1590/0103-8478cr20150935 in Brazil. 839 ISSN 1678-4596 MICROBIOLOGY Epidemiological, clinical and diagnostic aspects of sheep conidiobolomycosis in Brazil Aspectos epidemiológicos, clínicos e de diagnóstico da conidiobolomicose ovina no Brasil Carla WeiblenI Daniela Isabel Brayer PereiraII Valéria DutraIII Isabela de GodoyIII Luciano NakazatoIII Luís Antonio SangioniI Janio Morais SanturioIV Sônia de Avila BottonI* — REVIEW — ABSTRACT As lesões da conidiobolomicose normalmente são de caráter granulomatoso e necrótico, apresentando-se sob duas formas Conidiobolomycosis is an emerging disease caused clínicas: rinofacial e nasofaríngea. O presente artigo tem como by fungi of the cosmopolitan genus Conidiobolus. Particular objetivo revisar as principais características da doença em ovinos, strains of Conidiobolus coronatus, Conidiobolus incongruus and particularizando a epidemiologia, assim como os aspectos clínicos Conidiobolus lamprauges, mainly from tropical or sub-tropical e o diagnóstico das infecções causadas por Conidiobolus spp. no origin, cause the mycosis in humans and animals, domestic or Brasil. Neste País, a enfermidade é endêmica nas regiões nordeste wild. Lesions are usually granulomatous and necrotic in character, e centro-oeste, afetando ovinos predominantemente de raças presenting two clinical forms: rhinofacial and nasopharyngeal. deslanadas, ocasionando a morte na grande maioria dos casos This review includes the main features of the disease in sheep, with estudados. As espécies do fungo responsáveis pelas infecções an emphasis on the epidemiology, clinical aspects, and diagnosis em ovinos são C. coronatus e C. lamprauges e a forma clínica of infections caused by Conidiobolus spp. -

Mediastinal Mass in a Healthy Adolescent at the Children's
Chest clinic CASE BASED DISCUSSIONS Thorax: first published as 10.1136/thoraxjnl-2014-205764 on 10 October 2014. Downloaded from Mediastinal mass in a healthy adolescent at The Children’s Hospital at Westmead, Australia Ameneh Khatami,1 Alex C Outhred,1 Philip N Britton,1,2 Emilie Huguon,3 David J E Lord,4 Melanie Wong,5 Amanda Charlton,6 Alison M Kesson,1,2 David Isaacs1 For numbered affiliations see Ameneh Khatami and Emilie Huguon gamma release assay (IGRA) on whole blood was end of article. A previously well adolescent from the tropical positive. Percutaneous core biopsies of the medias- fi fi Correspondence to South Paci c island of Futuna was transferred due tinal mass demonstrated fungal hyphae in a broin- Dr Ameneh Khatami, to a 3-month to 4-month history of intermittent flammatory background and Splendore–Hoeppli Department of Infectious fevers, anorexia, weight loss, lethargy and haemop- phenomena (SHP) (figure 2A). Diseases and Microbiology, tysis. A Mantoux test was negative. CT scan ’ The Children s Hospital at demonstrated a large mediastinal mass and lymph- Westmead, Locked Bag 4001, Alison M Kesson and David Isaacs Westmead 2145, Australia; adenopathy with broncho-vascular compression, A positive IGRA in an adolescent from a [email protected]. and bilateral pleural and pericardial effusions, TB-endemic region is not unexpected. The histo- gov.au, ameneh.khatami@ (figure 1A). At admission, he was persistently gmail.com pathology suggests an invasive fungal infection, and febrile with non-tender cervical lymphadenopathy the patient’s raised eosinophil count would be con- Received 19 May 2014 and hepatomegaly, and had moderate respiratory sistent with this. -

Human Fungal Pathogens
This is a free sample of content from Human Fungal Pathogens. Click here for more information on how to buy the book. The Spectrum of Fungi That Infects Humans Julia R. Ko¨hler1, Arturo Casadevall2, and John Perfect3 1Division of Infectious Diseases, Children’s Hospital, Harvard Medical School, Boston, Massachusetts 02115 2Departments of Microbiology and Immunology and Medicine, Division of Infectious Diseases, Albert Einstein College of Medicine, New York, New York 10461 3Division of Infectious Diseases, Duke Medical Center, Durham, North Carolina 27710 Correspondence: [email protected] Few among the millions of fungal species fulfill four basic conditions necessary to infect humans: high temperature tolerance, ability to invade the human host, lysis and absorption of human tissue, and resistance to the human immune system. In previously healthy individu- als, invasive fungal disease is rare because animals’sophisticated immune systems evolved in constant response to fungal challenges. In contrast, fungal diseases occur frequently in immunocompromised patients. Paradoxically, successes of modern medicine have put in- creasing numbers of patients at risk for invasive fungal infections. Uncontrolled HIV infection additionally makes millions vulnerable to lethal fungal diseases. A concerted scientific and social effort is needed to meet these challenges. ungal infections today are among the most by which living humans became substrates for Fdifficult diseases to manage in humans. fungi. Given the tremendous wealth of recent Some fungi cause disease in healthy people, but findings on fungal evolution, phylogenetics, ge- most fungal infections occur in individuals al- nomics, development, and pathogenesis, this ready experiencing serious illness, and frequent- overview will necessarily omit much work criti- ly jeopardize the success of the newest medical cal to our understanding of fungi, which the advances in cancer care, solid organ and hema- other articles in this collection will focus on in topoietic stem cell transplantation, neonatal detail. -
Ep 3323422 A1
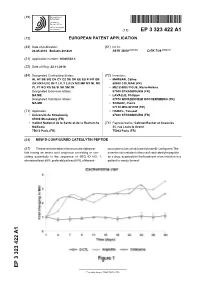
(19) TZZ¥¥ ¥ _T (11) EP 3 323 422 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 23.05.2018 Bulletin 2018/21 A61K 38/00 (2006.01) C07K 7/08 (2006.01) (21) Application number: 16306539.4 (22) Date of filing: 22.11.2016 (84) Designated Contracting States: (72) Inventors: AL AT BE BG CH CY CZ DE DK EE ES FI FR GB • MARBAN, Céline GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO 68000 COLMAR (FR) PL PT RO RS SE SI SK SM TR • METZ-BOUTIGUE, Marie-Hélène Designated Extension States: 67000 STRASBOURG (FR) BA ME • LAVALLE, Philippe Designated Validation States: 67370 WINTZENHEIM KOCHERSBERG (FR) MA MD • SCHAAF, Pierre 67120 MOLSHEIM (FR) (71) Applicants: • HAIKEL, Youssef • Université de Strasbourg 67000 STRASBOURG (FR) 67000 Strasbourg (FR) • Institut National de la Santé et de la Recherche (74) Representative: Cabinet Becker et Associés Médicale 25, rue Louis le Grand 75013 Paris (FR) 75002 Paris (FR) (54) NEW D-CONFIGURED CATESLYTIN PEPTIDE (57) The present invention relates to a cateslytin pep- no acids residues of said cateslytin are D-configured. The tide having an amino acid sequence consisting or con- invention also relates to the use of said cateslytin peptide sisting essentially in the sequence of SEQ ID NO: 1, as a drug, especially in the treatment of an infection in a wherein at least 80%, preferably at least 90%, of the ami- patient in needs thereof. EP 3 323 422 A1 Printed by Jouve, 75001 PARIS (FR) EP 3 323 422 A1 Description Field of the Invention 5 [0001] The present invention relates to the field of medicine, in particular of infections. -

An Integrated Genomic and Transcriptomic Survey of Mucormycosis-Causing Fungi
UCLA UCLA Previously Published Works Title An integrated genomic and transcriptomic survey of mucormycosis-causing fungi. Permalink https://escholarship.org/uc/item/9vc0d1xx Journal Nature communications, 7(1) ISSN 2041-1723 Authors Chibucos, Marcus C Soliman, Sameh Gebremariam, Teclegiorgis et al. Publication Date 2016-07-22 DOI 10.1038/ncomms12218 Peer reviewed eScholarship.org Powered by the California Digital Library University of California ARTICLE Received 3 Dec 2015 | Accepted 9 Jun 2016 | Published 22 Jul 2016 DOI: 10.1038/ncomms12218 OPEN An integrated genomic and transcriptomic survey of mucormycosis-causing fungi Marcus C. Chibucos1,2, Sameh Soliman3,w, Teclegiorgis Gebremariam3, Hongkyu Lee3, Sean Daugherty2, Joshua Orvis2, Amol C. Shetty2, Jonathan Crabtree2, Tracy H. Hazen1,2, Kizee A. Etienne4, Priti Kumari2, Timothy D. O’Connor2,5, David A. Rasko1,2, Scott G. Filler3,6, Claire M. Fraser2, Shawn R. Lockhart4, Christopher D. Skory7, Ashraf S. Ibrahim3,6 & Vincent M. Bruno1,2 Mucormycosis is a life-threatening infection caused by Mucorales fungi. Here we sequence 30 fungal genomes, and perform transcriptomics with three representative Rhizopus and Mucor strains and with human airway epithelial cells during fungal invasion, to reveal key host and fungal determinants contributing to pathogenesis. Analysis of the host transcriptional response to Mucorales reveals platelet-derived growth factor receptor B (PDGFRB) signaling as part of a core response to divergent pathogenic fungi; inhibition of PDGFRB reduces Mucorales-induced damage to host cells. The unique presence of CotH invasins in all invasive Mucorales, and the correlation between CotH gene copy number and clinical prevalence, are consistent with an important role for these proteins in mucormycosis pathogenesis. -

Conidiobolus Pachyzygosporus Invasive Pulmonary Infection in a Patient with Acute Myeloid Leukemia: Case Report and Review of the Literature E
Stavropoulou et al. BMC Infectious Diseases (2020) 20:527 https://doi.org/10.1186/s12879-020-05218-w CASE REPORT Open Access Conidiobolus pachyzygosporus invasive pulmonary infection in a patient with acute myeloid leukemia: case report and review of the literature E. Stavropoulou1, A. T. Coste2, C. Beigelman-Aubry3, I. Letovanec4, O. Spertini5, A. Lovis6, T. Krueger7, R. Burger1, P. Y. Bochud1 and F. Lamoth1,2* Abstract Background: Conidiobolus spp. (mainly C. coronatus) are the causal agents of rhino-facial conidiobolomycosis, a limited soft tissue infection, which is essentially observed in immunocompetent individuals from tropical areas. Rare cases of invasive conidiobolomycosis due to C. coronatus or other species (C.incongruus, C.lamprauges) have been reported in immunocompromised patients. We report here the first case of invasive pulmonary fungal infection due to Conidiobolus pachyzygosporus in a Swiss patient with onco-haematologic malignancy. Case presentation: A 71 year-old female was admitted in a Swiss hospital for induction chemotherapy of acute myeloid leukemia. A chest CT performed during the neutropenic phase identified three well-circumscribed lung lesions consistent with invasive fungal infection, along with a positive 1,3-beta-d-glucan assay in serum. A transbronchial biopsy of the lung lesions revealed large occasionally septate hyphae. A Conidiobolus spp. was detected by direct 18S rDNA in the tissue biopsy and subsequently identified at species level as C. pachyzygosporus by 28S rDNA sequencing. The infection was cured after isavuconazole therapy, recovery of the immune system and surgical resection of lung lesions. Conclusions: This is the first description of C. pachyzygosporus as human pathogen and second case report of invasive conidiobolomycosis from a European country. -

Neglected Fungal Zoonoses: Hidden Threats to Man and Animals
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector REVIEW Neglected fungal zoonoses: hidden threats to man and animals S. Seyedmousavi1,2,3, J. Guillot4, A. Tolooe5, P. E. Verweij2 and G. S. de Hoog6,7,8,9,10 1) Department of Medical Microbiology and Infectious Diseases, Erasmus MC, Rotterdam, 2) Department of Medical Microbiology, Radboud University Medical Centre, Nijmegen, The Netherlands, 3) Invasive Fungi Research Center, Mazandaran University of Medical Sciences, Sari, Iran, 4) Department of Parasitology- Mycology, Dynamyic Research Group, EnvA, UPEC, UPE, École Nationale Vétérinaire d’Alfort, Maisons-Alfort, France, 5) Faculty of Veterinary Medicine, University of Tehran, Tehran, Iran, 6) CBS-KNAW Fungal Biodiversity Centre, Utrecht, 7) Institute for Biodiversity and Ecosystem Dynamics, University of Amsterdam, Amsterdam, The Netherlands, 8) Peking University Health Science Center, Research Center for Medical Mycology, Beijing, 9) Sun Yat-sen Memorial Hospital, Sun Yat-sen University, Guangzhou, China and 10) King Abdullaziz University, Jeddah, Saudi Arabia Abstract Zoonotic fungi can be naturally transmitted between animals and humans, and in some cases cause significant public health problems. A number of mycoses associated with zoonotic transmission are among the group of the most common fungal diseases, worldwide. It is, however, notable that some fungal diseases with zoonotic potential have lacked adequate attention in international public health efforts, leading to insufficient attention on their preventive strategies. This review aims to highlight some mycoses whose zoonotic potential received less attention, including infections caused by Talaromyces (Penicillium) marneffei, Lacazia loboi, Emmonsia spp., Basidiobolus ranarum, Conidiobolus spp. -
Methods and Compositions Related to Riboswitches That Control Alternative Splicing
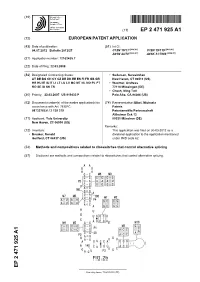
(19) & (11) EP 2 471 925 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 04.07.2012 Bulletin 2012/27 C12N 15/11 (2006.01) C12N 15/115 (2010.01) A01N 43/78 (2006.01) A61K 31/7088 (2006.01) (21) Application number: 12162435.7 (22) Date of filing: 22.03.2008 (84) Designated Contracting States: • Sudarsan, Narasimhan AT BE BG CH CY CZ DE DK EE ES FI FR GB GR New Haven, CT 06511 (US) HR HU IE IS IT LI LT LU LV MC MT NL NO PL PT • Wachter, Andreas RO SE SI SK TR 72116 Mössingen (DE) • Cheah, Ming Tatt (30) Priority: 22.03.2007 US 919433 P Palo Alto, CA 94306 (US) (62) Document number(s) of the earlier application(s) in (74) Representative: Elbel, Michaela accordance with Art. 76 EPC: Pateris 08732765.6 / 2 139 319 Patentanwälte Partnerschaft Altheimer Eck 13 (71) Applicant: Yale University 80331 München (DE) New Haven, CT 06510 (US) Remarks: (72) Inventors: This application was filed on 30-03-2012 as a • Breaker, Ronald divisional application to the application mentioned Guilford, CT 06437 (US) under INID code 62. (54) Methods and compositions related to riboswitches that control alternative splicing (57) Disclosed are methods and compositions related to riboswitches that control alternative splicing. EP 2 471 925 A1 Printed by Jouve, 75001 PARIS (FR) EP 2 471 925 A1 Description FIELD OF THE INVENTION 5 [0001] The disclosed invention is generally in the field of gene expression and specifically in the area of regulation of gene expression. -
Final Contaminant Candidate List 3 Microbes: Screening to PCCL
Final Contaminant Candidate List 3 Microbes: Screening to the PCCL Office of Water (4607M) EPA 815-R-09-0005 August 2009 www.epa.gov/safewater EPA-OGWDW Final CCL 3 Microbes: EPA 815-R-09-0005 Screening to the PCCL August 2009 Contents Abbreviations and Acronyms ......................................................................................................... 2 1.0 Background and Scope ....................................................................................................... 3 2.0 Recommendations for Screening a Universe of Drinking Water Contaminants to Produce a PCCL.............................................................................................................................. 3 3.0 Definition of Screening Criteria and Rationale for Their Application............................... 5 3.1 Application of Screening Criteria to the Microbial CCL Universe ..........................................8 4.0 Additional Screening Criteria Considered.......................................................................... 9 4.1 Organism Covered by Existing Regulations.............................................................................9 4.1.1 Organisms Covered by Fecal Indicator Monitoring ..............................................................................9 4.1.2 Organisms Covered by Treatment Technique .....................................................................................10 5.0 Data Sources Used for Screening the Microbial CCL 3 Universe ................................... 11 6.0 -

8 Clinical Manifestations of Invasive Fungal Infections
DK2996_half-series-title.qxd 6/24/05 12:04 PM Page 1 Fungal Infections in the Immunocompromised Patient DK2996_half-series-title.qxd 6/24/05 12:04 PM Page 2 INFECTIOUS DISEASE AND THERAPY Series Editor Burke A. Cunha Winthrop-University Hospital Mineola, and State University of New York School of Medicine Stony Brook, New York 1. Parasitic Infections in the Compromised Host, edited by Peter D. Walzer and Robert M. Genta 2. Nucleic Acid and Monoclonal Antibody Probes: Applications in Diagnostic Methodology, edited by Bala Swaminathan and Gyan Prakash 3. Opportunistic Infections in Patients with the Acquired Immunodeficiency Syndrome, edited by Gifford Leoung and John Mills 4. Acyclovir Therapy for Herpesvirus Infections, edited by David A. Baker 5. The New Generation of Quinolones, edited by Clifford Siporin, Carl L. Heifetz, and John M. Domagala 6. Methicillin-Resistant Staphylococcus aureus: Clinical Management and Laboratory Aspects, edited by Mary T. Cafferkey 7. Hepatitis B Vaccines in Clinical Practice, edited by Ronald W. Ellis 8. The New Macrolides, Azalides, and Streptogramins: Pharmacology and Clinical Applications, edited by Harold C. Neu, Lowell S. Young, and Stephen H. Zinner 9. Antimicrobial Therapy in the Elderly Patient, edited by Thomas T. Yoshikawa and Dean C. Norman 10. Viral Infections of the Gastrointestinal Tract: Second Edition, Revised and Expanded, edited by Albert Z. Kapikian 11. Development and Clinical Uses of Haemophilus b Conjugate Vaccines, edited by Ronald W. Ellis and Dan M. Granoff 12. Pseudomonas aeruginosa Infections and Treatment, edited by Aldona L. Baltch and Raymond P. Smith 13. Herpesvirus Infections, edited by Ronald Glaser and James F. -
Supplementary Materials Journal of Fungi New Method for Identifying Fungal Kingdom Enzyme Hotspots from Genome Sequences Lene L
Supplementary Materials Journal of Fungi New Method for identifying Fungal Kingdom Enzyme Hotspots from Genome Sequences Lene Lange1, Kristian Barrett2, and Anne S. Meyer2 1 BioEconomy, Research & Advisory, Copenhagen, 2500 Valby, Denmark; [email protected] (L.L) 2 Section for Protein Chemistry and Enzyme Technology, Department of Biotechnology and Biomedicine, Building 221, Technical University of Denmark, DK-2800 Kgs. Lyngby, Denmark; [email protected] (KB), [email protected] (ASM) Table S1. List of the rank of all 1.932 fungal species/strains with regard to biomass degrading capacity based on bioinformatics analysis of their genome sequence. The species are ranked with regard to the Total number of “Function;Family” observations, yet specifying the total number of “Function;Family” observations in each substrate category. The data shown is the full list of data supporting Table 1 in the main manuscript. ACC Submitter Total Xylan Xylan Lignin Pectin Cellulose No Species Class Phylum 1 Pecoramyces ruminatium Neocallimastigo Chytridio 248 85 208 0 541 GCA_000412615.1 Oklahoma State University 2 Neocallimastix californiae Neocallimastigo Chytridio 232 122 172 0 526 GCA_002104975.1 DOE Joint Genome Institute 3 Mycena citricolor Agarico Basidio 91 204 50 149 494 GCA_003987915.1 Universidade de Sao Paulo 4 Verticillium longisporum Sordario Asco 139 176 74 95 484 GCA_001268165.1 SLU 5 Coniochaeta sp. 2T2.1 Sordario Asco 117 102 108 98 425 GCA_009194965.1 DOE Joint Genome Institute 6 Paramyrothecium roridum Sordario Asco 106 163 63 79 411 GCA_003012165.1 USDA, ARS, NCAUR 7 Cadophora sp. DSE1049 Leotio Asco 105 138 75 91 409 GCA_003073865.1 DOE Joint Genome Institute 8 Diaporthe ampelina Sordario Asco 116 129 58 97 400 GCA_001630405.1 Bangalore University 9 Diaporthe longicolla Sordario Asco 111 128 56 90 385 GCA_000800745.1 Purdue University 10 Diaporthe sp. -

Rhinoentomophthoromycosis Caused by Conidiobolous Coronatus in a Diabetic Patient: the Importance of Species Identification
Rhinoentomophthoromycosis caused by Conidiobolous coronatus in a diabetic patient: the importance of species identification Anil Kumar, Vineeth Viswam1, Sukhmani Regi2, Kavitha R. Dinesh, Madhumita Kumar1, Shamsul Karim Departments of Microbiology, 1Otorhinolaryngology, and 2Pathology, Amrita Institute of Medical Sciences, Ponekara, Kochi, Kerala, India CASE REPORT CASE Abstract by swelling of nose, paranasal sinuses, and mouth. We present a case of a 43-year-old male who presented with rightRhinoentomopthoromycosis nasal blockade and paranasal usually sinus presents pain assince a chronic two months. inflammatory The clinical or granulomatous picture was further disease complicated characterized by the fact that neither the patient could tolerate plain amphoterecin B nor could he afford its liposomal derivative. appropriateSpecies identification choice of therapyenabled in us resource to successfully poor settings treat the in developing patient with countries. cheaper and less toxic alternative like itraconazole and potassium iodide. Our case highlights the importance of species identification in making Key words: Conidiobolus coronatus, potassium iodide, Splendore-Hoeppli phenomenon Introduction tomography (CT) of paranasal sinuses revealed a retention cyst in the right maxillary sinus and Entomophthoromycosis (Conidiobolomycosis) is caused a soft tissue mass measuring 5.6 cm × 1.5 cm in by Conidiobolus coronatus, a mould belonging to the the right nasal cavity extending from anterior nare order Entomopthorales of the class Zygomycetes.