French SOCIO.DEMOGRAPHIC STUDY in the UPPER-NIGER
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Climatic Information of Western Sahel F
Discussion Paper | Discussion Paper | Discussion Paper | Discussion Paper | Clim. Past Discuss., 10, 3877–3900, 2014 www.clim-past-discuss.net/10/3877/2014/ doi:10.5194/cpd-10-3877-2014 CPD © Author(s) 2014. CC Attribution 3.0 License. 10, 3877–3900, 2014 This discussion paper is/has been under review for the journal Climate of the Past (CP). Climatic information Please refer to the corresponding final paper in CP if available. of Western Sahel V. Millán and Climatic information of Western Sahel F. S. Rodrigo (1535–1793 AD) in original documentary sources Title Page Abstract Introduction V. Millán and F. S. Rodrigo Conclusions References Department of Applied Physics, University of Almería, Carretera de San Urbano, s/n, 04120, Almería, Spain Tables Figures Received: 11 September 2014 – Accepted: 12 September 2014 – Published: 26 September J I 2014 Correspondence to: F. S. Rodrigo ([email protected]) J I Published by Copernicus Publications on behalf of the European Geosciences Union. Back Close Full Screen / Esc Printer-friendly Version Interactive Discussion 3877 Discussion Paper | Discussion Paper | Discussion Paper | Discussion Paper | Abstract CPD The Sahel is the semi-arid transition zone between arid Sahara and humid tropical Africa, extending approximately 10–20◦ N from Mauritania in the West to Sudan in the 10, 3877–3900, 2014 East. The African continent, one of the most vulnerable regions to climate change, 5 is subject to frequent droughts and famine. One climate challenge research is to iso- Climatic information late those aspects of climate variability that are natural from those that are related of Western Sahel to human influences. -

Are the Fouta Djallon Highlands Still the Water Tower of West Africa?
water Article Are the Fouta Djallon Highlands Still the Water Tower of West Africa? Luc Descroix 1,2,*, Bakary Faty 3, Sylvie Paméla Manga 2,4,5, Ange Bouramanding Diedhiou 6 , Laurent A. Lambert 7 , Safietou Soumaré 2,8,9, Julien Andrieu 1,9, Andrew Ogilvie 10 , Ababacar Fall 8 , Gil Mahé 11 , Fatoumata Binta Sombily Diallo 12, Amirou Diallo 12, Kadiatou Diallo 13, Jean Albergel 14, Bachir Alkali Tanimoun 15, Ilia Amadou 15, Jean-Claude Bader 16, Aliou Barry 17, Ansoumana Bodian 18 , Yves Boulvert 19, Nadine Braquet 20, Jean-Louis Couture 21, Honoré Dacosta 22, Gwenaelle Dejacquelot 23, Mahamadou Diakité 24, Kourahoye Diallo 25, Eugenia Gallese 23, Luc Ferry 20, Lamine Konaté 26, Bernadette Nka Nnomo 27, Jean-Claude Olivry 19, Didier Orange 28 , Yaya Sakho 29, Saly Sambou 22 and Jean-Pierre Vandervaere 30 1 Museum National d’Histoire Naturelle, UMR PALOC IRD/MNHN/Sorbonne Université, 75231 Paris, France; [email protected] 2 LMI PATEO, UGB, St Louis 46024, Senegal; [email protected] (S.P.M.); [email protected] (S.S.) 3 Direction de la Gestion et de la Planification des Ressources en Eau (DGPRE), Dakar 12500, Senegal; [email protected] 4 Département de Géographie, Université Assane Seck de Ziguinchor, Ziguinchor 27000, Senegal 5 UFR des Sciences Humaines et Sociales, Université de Lorraine, 54015 Nancy, France 6 Master SPIBES/WABES Project (Centre d’Excellence sur les CC) Bingerville, Université Félix Houphouët Boigny, 582 Abidjan 22, Côte d’Ivoire; [email protected] 7 Doha Institute for Graduate Studies, -

Pastoralism and Security in West Africa and the Sahel
Pastoralism and Security in West Africa and the Sahel Towards Peaceful Coexistence UNOWAS STUDY 1 2 Pastoralism and Security in West Africa and the Sahel Towards Peaceful Coexistence UNOWAS STUDY August 2018 3 4 TABLE OF CONTENTS Abbreviations p.8 Chapter 3: THE REPUBLIC OF MALI p.39-48 Acknowledgements p.9 Introduction Foreword p.10 a. Pastoralism and transhumance UNOWAS Mandate p.11 Pastoral Transhumance Methodology and Unit of Analysis of the b. Challenges facing pastoralists Study p.11 A weak state with institutional constraints Executive Summary p.12 Reduced access to pasture and water Introductionp.19 c. Security challenges and the causes and Pastoralism and Transhumance p.21 drivers of conflict Rebellion, terrorism, and the Malian state Chapter 1: BURKINA FASO p.23-30 Communal violence and farmer-herder Introduction conflicts a. Pastoralism, transhumance and d. Conflict prevention and resolution migration Recommendations b. Challenges facing pastoralists Loss of pasture land and blockage of Chapter 4: THE ISLAMIC REPUBLIC OF transhumance routes MAURITANIA p.49-57 Political (under-)representation and Introduction passivity a. Pastoralism and transhumance in Climate change and adaptation Mauritania Veterinary services b. Challenges facing pastoralists Education Water scarcity c. Security challenges and the causes and Shortages of pasture and animal feed in the drivers of conflict dry season Farmer-herder relations Challenges relating to cross-border Cattle rustling transhumance: The spread of terrorism to Burkina Faso Mauritania-Mali d. Conflict prevention and resolution Pastoralists and forest guards in Mali Recommendations Mauritania-Senegal c. Security challenges and the causes and Chapter 2: THE REPUBLIC OF GUINEA p.31- drivers of conflict 38 The terrorist threat Introduction Armed robbery a. -

Kouroussa Diplomatie
République de Guinée Travail-Justice-Solidarité Volonté d’engagement de la commune urbaine de Kouroussa dans une coopération décentralisée avec des communes étrangères Ed 2021 MOT DU MAIRE DE KOUROUSSA Chers futurs partenaires, J’ai l’immense honneur de vous présenter la commune de Kouroussa et d’exprimer notre volonté de tisser des relations de coopération avec votre collectivité. Nous croyons aux vertus de la coopération décentralisée: elle est un moyen précieux pour favoriser les échanges entre peuples qui partagent les mêmes valeurs de solidarité internationale. En Guinée, Kouroussa est située à 582 km de la capitale, Conakry et à 83 km de Kankan, la deuxième ville du pays. Riche en eau et en or, il existe d’importantes activités minières sur le territoire. Chef-lieu de la préfecture, la ville a été érigée en commune urbaine en 1991. Le conseil communal, composé de 23 élus, que j’ai l’honneur de présider, a été installé le 29 octobre 2019 pour un mandat de 5 ans. Notre ambition est de renforcer notre capacité de mobilisation des ressources locales, d'ouvrir notre ville au monde et bâtir des projets de coopération sur les grands enjeux du développement durable. Nous souhaitons un partenariat qui profite à l'agriculture dont vit 90% de notre population. Une coopération qui favorise l’émergence d’une ville durable, les échanges d'idées, de savoirs et de savoir-faire. Les potentiels de rapprochement entre Kouroussa et les communes françaises ou étrangères sont inestimables notamment dans le domaine de la culture, de l'éducation, la santé, la démocratie participative, la promotion et la défense des droits des femmes et des 1 MOT DU MAIRE DE KOUROUSSA enfants. -

Appraisal Report Kankan-Kouremale-Bamako Road Multinational Guinea-Mali
AFRICAN DEVELOPMENT FUND ZZZ/PTTR/2000/01 Language: English Original: French APPRAISAL REPORT KANKAN-KOUREMALE-BAMAKO ROAD MULTINATIONAL GUINEA-MALI COUNTRY DEPARTMENT OCDW WEST REGION JANUARY 1999 SCCD : N.G. TABLE OF CONTENTS Page PROJECT INFORMATION BRIEF, EQUIVALENTS, ACRONYMS AND ABBREVIATIONS, LIST OF ANNEXES AND TABLES, BASIC DATA, PROJECT LOGICAL FRAMEWORK, ANALYTICAL SUMMARY i-ix 1 INTRODUCTION.............................................................................................................. 1 1.1 Project Genesis and Background.................................................................................... 1 1.2 Performance of Similar Projects..................................................................................... 2 2 THE TRANSPORT SECTOR ........................................................................................... 3 2.1 The Transport Sector in the Two Countries ................................................................... 3 2.2 Transport Policy, Planning and Coordination ................................................................ 4 2.3 Transport Sector Constraints.......................................................................................... 4 3 THE ROAD SUB-SECTOR .............................................................................................. 5 3.1 The Road Network ......................................................................................................... 5 3.2 The Automobile Fleet and Traffic................................................................................. -

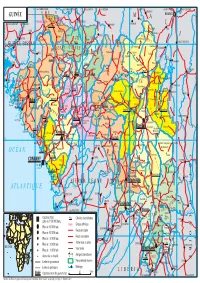
Guinea : Reference Map of Kankan Region (As of 3 March 2015)
Guinea : Reference Map of Kankan Region (as of 3 March 2015) Bankolen Mambifagalena Niagassola Kry Tourelen Berlen Sokoromansa Magadiano Faraboloni Linkekoro KIGNEKOUROU CENTRE Bouyido Malsadou Seourou Konfara 2 Gnembou Tanssa Magnaka KOTE CENTRE Balenda SOUMBARAYA CENTRE Kourelen TALABE CENTRE Dialawassa II Kondoko Djanwely Itipony Dougounta Dora Kourakoda DIBIA CENTRE Djinko Ilimalo Naboun Kanimbakalako Kodougoulen KAKAMA CENTRE Tondo Komagron Kayaga Kignedi Sininko Kadabili Kignero Gnere Sininkoro Badamako Kounsounkoro Yirikelèma Kanikoumbaya SOKORO CENTRE DIATEA CENTRE Dita Salla Tondji1 Koda Kebesabaya Siguirini Sakounou Malea Bembéta Megnèkoma Silabado Diakan Toukönö BOULAN CENTRE Gbèdela MANKADIAN CENTRE Gbörökola Doko Tombani Maragbè Kana Sékela Mansadji Sidao Tonso Banankölö Tomba Doula Amina Amina Kinièba Franwalia Tinko Diatifere Fountou Soumbalakölen Iroda Kounkoun Koda Mainou SARAYA CENTRE Tomboni Sinimbaya KOBEDRA CENTRE MIGNADA CENTRE Bökökö Farani Banora Simbona Bida Tomba Boufe Bandioula FOULATA CENTRE Kintinian Yorola Tougnou Sanouna SEELA CENTRE Bankon MALI Tinkoba Kobada Beretela Sando Noumandiana Kandani Fodela Bèrèko Tabakoro BAMBALA Tabako Madila Moyafara Kourouni Banantamou Siguiri FALAMA BANFARA CENTRE Saint Alexis Dialakoro Nedekoroko Banantou Lansanaya Sakolado Manakoro Farabada Dounin Farabelen Bida Bantambaye Woléwoléya Koda Koda Kogne Tambabougou Gbongoroma Kigne Kokoudouninda Dinguiraye Gbilin Balandougouba KONKOYE CENTRE Waran-Fougou Kiniebakoura DIARRADOU CENTRE Sansani Faradjian Tassiliman Centre Kewoulé -

Région De Kankan 2018
REPUBLIQUE DE GUINEE Travail - Justice- Solidarité MINISTERE DU PLAN ET DU DEVELOPPEMENT ECONOMIQUE La région de Kankan en chiffres Edition 2020 GEOGRAPHIE ET ORGANISATION ADMINISTRATIVE Géographie 0rganisation administrative en 2018 5 préfectures ; 53 sous-préfectures ; 5 communes urbaines, Superficie = 72 145km2 920 districts/quartiers ; 2 117 secteurs 53 communes rurales Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) Préfectures Sous-préfectures Balandougou, Bate-Nafadji, Boula, Gberedou-Baranama, Karifamoriyah, Koumban, Kankan Mamouroudou, Missamana, Moribayah, Sabadou-Baranama, Tinti-Oulen, Tokounou Kérouané Banankoro, Damaro, Komodou, Kounsankoro, Linko, Sibiribaro, Soromaya Babila, Balato, Banfele, Baro, Cissela, Douako, Doura, Kiniero, Komola-Koura, Koumana, Kouroussa Sanguiana Balandougouba, Dialakoro, Faralako, Kantoumania, Kinieran, Kondianakoro, Koundian, Morodou, Mandiana Niantania, Saladou, Sansando Banko, Doko, Faranwalia, Kiniebakoura, Kintinian, Malea, Naboun, Niagossola, Niandankoro, Siguiri Norassoba, Nounkounkan, Siguirini Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) STATISTIQUES DEMOGRAPHIQUES Population 1983 1996 2014 Population région de Kankan 640 432 1 011 644 1 972 537 Population de la principale préfecture : Siguiri 161 303 271 224 687 002 Part de la population nationale en 2014 : 18,7 % Rang régional en 2018 : 1/8 Sources : Institut national de la statistique/RGPH Population au 1er -

Download Map (PDF | 1.37
GUINEE: Couverture des bureaux de zones ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Sambailo ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! SENEGAL ! ! ! ! ! Koundara Ctre ! ! ! ! ! ! ! ! ! ! Youkounkoun ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Sareboido ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Termesse ! ! ! ! ! ! ! ! ! Koundara ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Kamabi ! ! ! ! ! ! ! ! Guinguan ! ! ! ! Balaki ! ! !! ! ! ! ! Lebekeren ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Touba ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Foulamory ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Niagassola ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Mali Mali Ctre ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Naboun ! ! ! ! ! ! ! ! ! ! ! ! ! ! Madina Wora ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Gadha Woundou ! Hidayatou ! ! GUINEE BISSAU ! ! ! ! ! ! ! Gayah ! ! ! ! ! ! ! ! ! ! Salambande ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Labe ! ! ! ! Fougou ! ! ! ! ! ! ! ! ! ! ! ! Telire ! ! Kounsitel ! ! ! ! ! ! ! ! ! ! Dougountouny ! ! Fello Koundoua ! Siguirini ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Gagnakaly ! ! ! ! ! ! MALI ! ! ! ! ! ! Franwalia ! Fafaya ! ! ! ! Linsan Saran Yimbering Donghol Sigon Diatifere ! ! ! Banora ! Matakaou ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Gaoual Ctre ! ! ! ! Koumbia ! ! ! ! ! ! ! ! ! ! ! ! Doko ! ! ! ! ! ! ! ! ! ! -

UNMEER) External Situation Report 22 January 2015
UN Mission for Ebola Emergency Response (UNMEER) External Situation Report 22 January 2015 KEY POINTS World Bank report forecast higher economic loses for affected countries SE Nabarro provides an updated ONR in global efforts to stop Ebola Border surveillance initiatives intensify Key Political and Economic Developments 1. In a World Bank Report prepared for the 2015 World Economic Forum in Davos, the Bank acknowledged progress made in slowing the EVD transmission rate, but cautioned that recent efforts have likely reduced the impact of Ebola on the African economy perhaps from USD 30 billion to USD 6 billion. The report noted that most of these losses are forecasted to hit the affected countries. 2. In Davos, Switzerland, Special Envoy David Nabarro provided an updated Overview of Needs and Requirements in the global efforts to stop Ebola. The financial needs for the first six month of 2015 amount to 1.5 billion USD. Almost 500 million USD is already available and the appeal is now for the gap of 1 billion USD. Response Efforts and Health 3. Between 14 and 16 January, UNFPA provided 100 dignity kits (a kit contains a mattress, a set of hygiene supplies and a set of IPC supplies) to 100 female Ebola survivors and widows in Bomi County, Liberia. Similarly, 150 dignity kits were provided to survivors and widows in Grand Cape Mount County. Prior to this, UNFPA had provided expanded kits to 1,000 survivors of Ebola and SGBV in 21 districts in 10 counties. The expanded kits also include food items (500 bags of rice (25 kg), 6,000 energy drinks and non-food items (beddings and clothes)). -

REPUBLIC of GUINEA Labor–Justice–Solidarity
REPUBLIC OF GUINEA Labor–Justice–Solidarity MINISTRY OF AGRICULTURE AND LIVESTOCK NATIONAL STRATEGY FOR THE DEVELOPMENT OF RICE GROWING APRIL 2009 Table of contents LIST OF ACRONYMS AND ABBREVIATIONS 5 SUMMARY 6 I. INTRODUCTION 8 II. REVIEWING THE RICE SECTOR 9 2.1. The policy position of rice 10 2.2 Preferences and demand estimates 10 2.3 Typology and number of rice farmers, processors and marketers 11 2.4. Gender dimensions 13 2.5. Comparative advantage of national rice production 14 III. CHALLENGES AND OPPORTUNITIES 14 3.1. The potential of local rice for rural poverty reduction and economic growth 14 3.2. The land system 15 3.3. Social issues 16 3.4. Trans-border and regional issues 16 3.5. Knowledge and lessons learnt from R&D in rice 16 VI. PRIORITY AREAS AND PERSPECTIVES 17 4.1. Ranking by order of priority in terms of potential contribution to national production 17 4.2. Identification and ranking specific environmental challenges and related opportunities by order of priority 18 4.3. Identification of policy challenges/opportunities 20 4.3.1. Policy challenges 20 4.3.1. Opportunities 21 V. VISION AND FRAMEWORK OF THE NATIONAL RICE STRATEGY 21 5.1. Objectives of rice production 21 5.5.1. Overall target: 21 5.5.2. Quantified objectives: 21 5.2.3. Strategy development phase 23 5.2.4. Key interventions 24 5.2.5 Scientists, technicians and agricultural advisory agents in 2008 and beyond 25 5.2.6. Governance of the Rice Growing Development Strategy 25 5.2.7. -
GUINÉE Gam L BAMAKO PARC NAT
14° vers TAMBACOUNDA vers TAMBACOUNDA 12° vers SARAYA vers KÉNÉBIA 10° vers KITA vers KITA 8° vers KOULIKORO vers SÉGOU S É N É G A L F SIRAKORO bie a GUINÉE Gam l BAMAKO PARC NAT. é M m A DU KONIAGUI é GALÉ FOULAKOUNDA BADIAR KÉDOUGOU g L n i B vers ZIGUINCHOR vers KOLDA F f SAGABARI a Youkounkoun ARABA a k Koundara o B y ba ï G Niagassola SIBI ê Sarébo do a G GABU Guingan m o T i b B Balandou I o i al K m T e F LÉ é R iba ouba A A M ok l i Kifaya Tamgué D A o vers BISSAO o L ro F Á K n 1538 m I BA AT Foulamôri é Balaki I Sou baraya N K A É OUÉLÉSSÉBOUGOU 12° GUINÉE-BISSAO Mali L Boukaria 12° B S m a O a Naboun Kouré alé n l y N E - G U I N É o o KANGABA k Y E N E N k a é XIME O a r M m Madina l Ya béring F a ÉL K andanda Maléa B u B I m n Koumbia Sala bandé Doko o Kounsitél É i a e Siguirini Barrage B bi g è è R al m in Diatif r E de Sélingué vers BISSAO ub Gaoual a f Rio Cor G a IG KANGARÉ BUBA oumb B Banora N é K a Koubia Nafadji n Kintinian é i i Dabalaré F m Malanta ô F o K llé ifa BOUGOUNI Wéndou Mbôrou T Ganiakali Siguiri n Fouta Labé T H Dialakoro o Lélouma ougué A g Tin vers SIKASSO o 1245 U kisso K Hamdallaï Kâkoni F L T E Kiniébakoura K O U A Dinguiraye - G Balandougouba CATIÓ LÉ o U I SANSA g Sélouma N É E o ê Dabiss H rico a Kalinko Koundianakoro n Missira Kankalabé Sangarédi m F YANFOLILA i Chutes arakoba Niandankoro r o e k de Kinkon ka s n Sansalé L A Santou a Pita s i ou i m Sansando c U K B k Ko ola Koura Niantanina a u F O Tén n ié M Niani BADOGO L C ing ilin m é i n GARA O T ta Konsota i T a O io Dobali Djalon B m -
MCHIP Guinea End-Of-Project Report October 2010–June 2014
MCHIP Guinea End-of-Project Report October 2010–June 2014 Submitted on: September 15, 2014 Submitted to: United States Agency for International Development under Coooperative Agreement # GHS-A-00-08-00002-000 Submitted by: Yolande Hyjazi, Rachel Waxman and Bethany Arnold 1 The Maternal and Child Health Integrated Program (MCHIP) is the USAID Bureau for Global Health’s flagship maternal, neonatal and child health (MNCH) program. MCHIP supports programming in maternal, newborn and child health, immunization, family planning, malaria, nutrition, and HIV/AIDS, and strongly encourages opportunities for integration. Cross-cutting technical areas include water, sanitation, hygiene, urban health and health systems strengthening. MCHIP brings together a partnership of organizations with demonstrated success in reducing maternal, newborn and child mortality rates and malnutrition. Each partner will take the lead in developing programs around specific technical areas: Jhpiego, as the Prime, will lead maternal health, family planning/reproductive health, and prevention of mother-to-child transmission of HIV (PMTCT); JSI—child health, immunization, and pediatric AIDS; Save the Children—newborn health, community interventions for MNCH, and community mobilization; PATH—nutrition and health technology; JHU/IIP—research and evaluation; Broad Branch—health financing; PSI—social marketing; and ICF International—continues support for the Child Survival and Health Grants Program (CSHGP) and the Malaria Communities Program (MCP). This report was made possible by the generous support of the American people through the United States Agency for International Development (USAID), under the terms of the Leader with Associates Cooperative Agreement GHS-A-00-08-00002-00. The contents are the responsibility of the Maternal and Child Health Integrated Program (MCHIP) and do not necessarily reflect the views of USAID or the United States Government.